External and internal tibial torsion represent common anatomical variants in the paediatric population, thought to be secondary to intrauterine positioning, neuromuscular or hereditary disorders [1,2]. Particularly with internal tibial torsion, the deformity generally improves spontaneously by adolescence without long-term sequelae [3-5] requiring only patient and parent education, observation and reassurance [6]. However, in cases of significant deformity with functional issues, surgical management may be indicated [6,7].
Various technical approaches have been proposed as a means of surgically correcting excessive tibial torsion based on the location and nature of the deformity [8]. Proximal tibial osteotomy has been described, but it does carry a risk of peroneal nerve injury, although this potentially can be mitigated by fibular osteotomy and anterior compartment release [9]. While lower peroneal nerve injury is reported using a distal transverse tibial osteotomy [10,11], it represents a viable alternative to proximal osteotomy. In the proximal tibia, purposeful oblique osteotomy has been described by Rab GT which allows for correction of both coronal plane and rotational plane deformity simultaneously [12]. Meanwhile, the impact of an oblique cut in the distal tibia has not been rigorously studied.
Ankle alignment is generally measured based on ADTA and LDTA. These measurements are made relative to the mechanical or anatomical axis of the tibia in the sagittal plane for ADTA or coronal plane for LDTA. Previous studies have defined normal values for both ADTA (80°±2°) and LDTA (88.6°±4°) [13,14]. Given the known ankle alignment in the coronal and sagittal planes, variances from neutral can be tracked as rotational modifications created in the distal tibia.
As the consequences on ankle alignment following unintended transverse and angled osteotomies in the distal tibia are largely unknown, the purpose of this investigation was to design an anatomical model to assess how changes in the orientation of the cut angle in distal tibial osteotomies affect ankle alignment in specimens with existing rotational deformities. The purpose of this study was to better understand the tolerance and consequences on ankle alignment after unintended angular cuts following derotational distal tibial osteotomies. We hypothesised that as little as 10° variation in cut angle orientation would result in significant changes in ankle alignment, based on changes in ADTA and LDTA.
Materials and Methods
A total 579 skeletons from the Hamann Todd Osteological Collection were previously measured for tibial rotation [5]. Within this database, we identified the ten left-sided specimens, with the greatest degrees of internal (n=5 specimens) and external (n=5 specimens) rotational deformity. The study began in November 2016 and concluded in June 2017. Specimens with the highest degree of internal or medial rotational deformity had a mean 16.4° (range, 23.3° to 11.9°) deviation from neutral while the specimens with external or lateral rotational deformity had a mean 29.6° (range, 32.5° to 27.7°) deviation from neutral. Specimens had a mean age of 51.3 years (range, 40 to 62 years), with demographics listed in [Table/Fig-1].
Demographic data of specimen utilised.
| Specimen | Rotation from Neutral (degrees)* | Cadaver Age (years) | Sex | Race |
|---|
| Internal Rotation | 1 | 23.3 | 50 | M | AA |
| 2 | 22.9 | 57 | M | C |
| 3 | 12.1 | 48 | M | AA |
| 4 | 12.1 | 40 | M | C |
| 5 | 11.9 | 40 | M | AA |
| External Rotation | 6 | 27.7 | 42 | M | AA |
| 7 | 28.1 | 62 | M | C |
| 8 | 28.4 | 53 | M | C |
| 9 | 31.1 | 62 | M | C |
| 10 | 32.5 | 59 | F | C |
*Rotational deformity measurement of left tibia
M: Male; F: Female; AA: African American; C: Caucasian
Tibial specimens were surface scanned using a ROMER 7X Scan Arm (Hexagon, Surrey, United Kingdom) to produce a three-dimensional (3D) image of each tibia using PolyWorks 2014 software (InnovMetric Software, Quebec, Canada). Multiple scans from the anterior and posterior sides of each tibia were assembled and aligned using the software’s best-fit algorithm. These 3D images were exported as polygonal models into stereolithographic (.stl) mesh formatting. Surface scanning file imperfections were corrected using Microsoft 3D Model Repair Service (Microsoft, Redmond, WA). Following model repair, .stl models were uploaded into Blender 2.76 software (Blender Foundation, Amsterdam, Netherlands) and registered to the tibial component of the Human Tibia and Fibula Model (NIH 3D Print Exchange) and served as the template for orientation of scanned tibia files [Table/Fig-2]. The registered files were primarily oriented based on the inferior articular surface of the Human Tibia and Fibula Model, while the medial malleolus and fibular notch served as secondary alignment markers.
Lateral three-dimensional reconstruction images obtained using blender 2.76 software. Angled (a) versus transverse (b) cuts 5 cm above the inferior articular surface of the tibia.
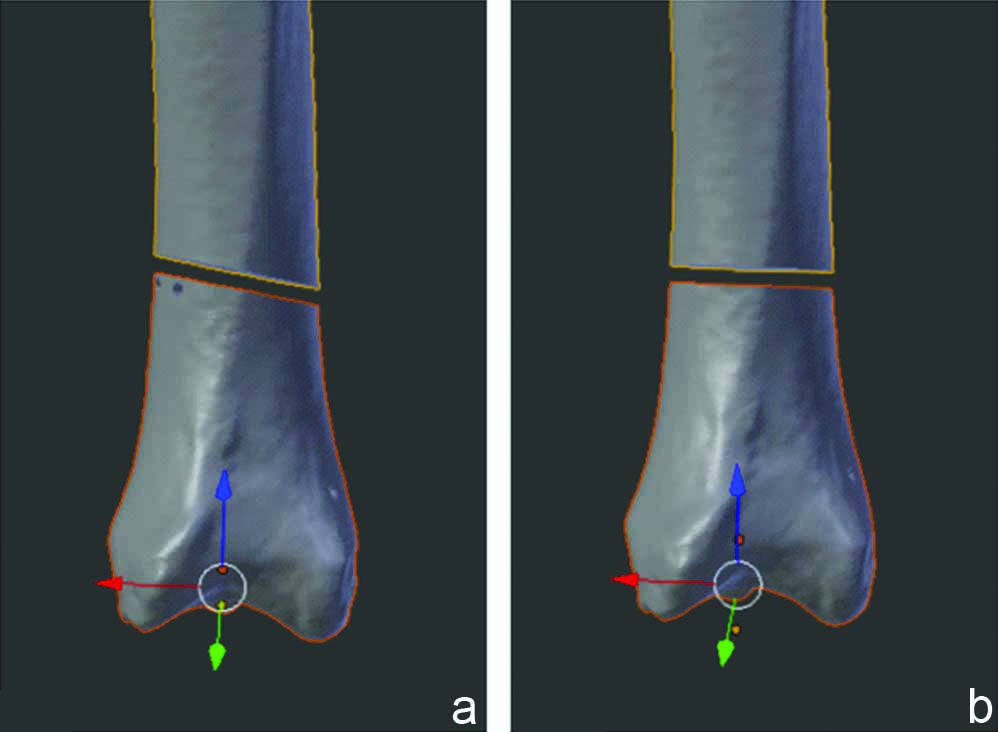
Following registration, tibia models were divided into proximal, middle and distal components. Proximal cuts were made 200-225 cm above the inferior articular surface of the models, and were necessary because our maximal print size could not otherwise accommodate the specimens. A step cut was made proximally to allow easy reconstruction of the natural anatomy after printing. The remaining distal portion of tibia was then divided using a transverse versus angled cut, simulating distal tibial osteotomies oriented perpendicular to the shaft versus parallel to the distal joint surface. Both transverse and angled cuts were made 5 cm above the level of the inferior articular surface of the tibia. The angled cut was made virtually with the aid of geometric triangles at a 10° angle in an anterior-superior to posterior-inferior orientation relative to the tibial shaft, creating a cut nearly parallel to the distal articular surface. After making the tibial subdivisions, pegs and degree markings were added to models, to aid with distal rotation during surgical pinning.
Final files were uploaded from Blender software into Simplify 3D software (Simplify 3D, Cincinnati, Ohio) to set print orientation at 0.3 mm resolution and 10% honey-comb infill of the tibias. All files were printed on a Makerbot Replicator 2 Printer (MakerBot, Brooklyn, New York). A total of 20 models were printed from the 10 specimens, 10 with a transverse cut and 10 with an angled cut. Prior to surgical pinning, printing rafts and external supports were removed, the proximal and middle components of the tibia models were adhered and the models were sanded to remove irregularities.
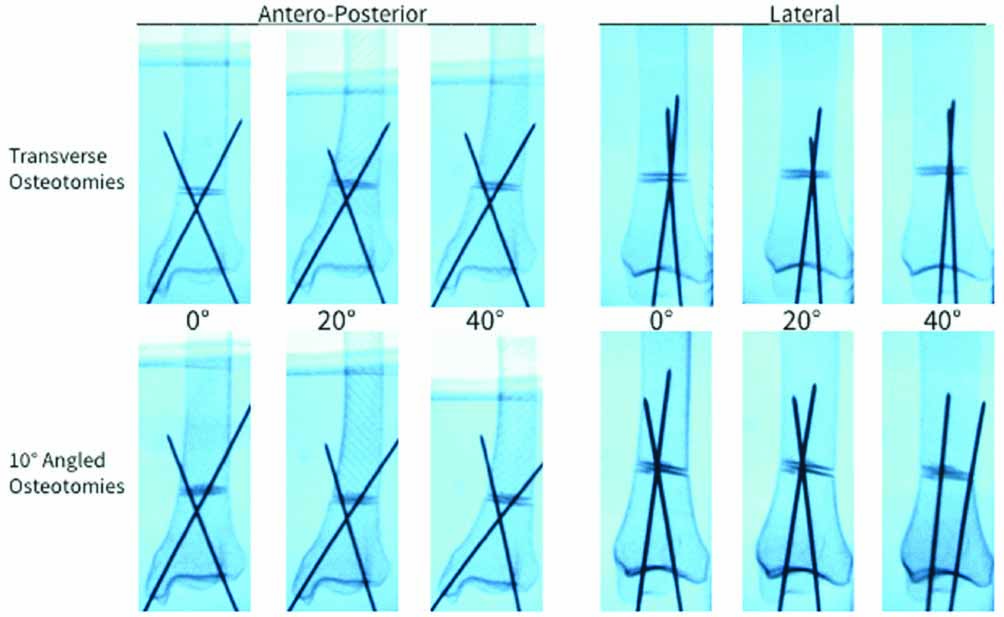
Next, the specimens with external rotational deformity were cross-pinned at 0°, 20° and 40° of internal rotation using two 0.54 Kirscher wires and vice-versa for the specimens with internal rotational deformity. Specimens were then positioned at the level of radiolucent table surface and lateral and anterior-posterior X-rays were obtained at 0°, 20° and 40° of rotation from neutral. Digital images of the X-rays were uploaded to Image J (National Institute of Health, Bethesda, Maryland) and ADTA and LDTA were measured in accordance with previously published guidelines [Table/Fig-3] [13,14].
Antero-posterior and lateral radiographs of transverse and angled osteotomies at 0°, 20° and 40° of external rotation from neutral.
Statistical Analysis
Inter-rater reliability of ADTA and LDTA measurements were established by calculating an Intraclass Correlations Coefficient (ICC) by two study investigators in two specimens undergoing transverse and two specimens undergoing angled osteotomies. Following established recommendations, we considered an ICC of <0.4 to be poor, 0.4-0.75 to be fair to good, and >0.75 to be excellent [15,16]. Comparisons between straight and angled distal tibial osteotomies at 0°, 20° and 40° rotation for ADTA and LDTA were calculated using repeated measures analysis of variance (ANOVA). Angle measurements were compared at 0°, 20° and 40° rotation using a post-hoc test. Statistical significance was defined by p<0.05. Statistical analysis was performed using the SPSS statistical package (Version 23, IBM Corporation, Armonk, New York).
Results
Inter-rater Reliability
ICC values were 0.976 for ADTA measurements and 0.912 for LDTA measurements, indicating excellent inter-rater reliability.
Transverse Osteotomies
In the transverse osteotomies at 0° rotation, both the LDTA and ADTA values (89.6°±2.7° and 83.1°±2.7°, respectively) corresponded approximately to the previously defined normative values (88.6°±4° and 80°±2°, respectively) [14]. After internal or external rotation, post-hoc analysis showed no statistical difference in mean LDTA or ADTA measurements based on degree of rotation [Table/Fig-4].
Measurements for transverse and angled osteotomy cuts.
| Transverse Osteotomy |
|---|
| LDTA | 0° | 20° | 40° | p-value* |
|---|
| External Rotation | 89.8±3.1 | 88.2±2.8 | 88.7±4.3 | .82/.40/.65/.82 |
| Internal Rotation | 89.4±2.5 | 89.7±2.9 | 86.3±2.6 | .69/.86/.09/.09 |
| ADTA | 0° | 20° | 40° | p-value* |
| External Rotation | 81.9±2.6 | 81.8±3.0 | 81.4±3.0 | .35/.93/.78/.85 |
| Internal Rotation | 84.2±2.5 | 83.8±2.5 | 84.4±2.1 | .88/.80/.90/.69 |
| Angled Osteotomy |
| LDTA | 0° | 20° | 40° | p-value* |
| External Rotation | 90.1±2.2 | 93.7±3.7 | 98.1±4.6 | .005†/ .11/.01†/.14 |
| Internal Rotation | 90±2.2 | 83.7±3.6 | 80.4±1.0 | .02†/.01†/.0001†/.10 |
| ADTA | 0° | 20° | 40° | p-value* |
| External Rotation | 82.1±2.3 | 80.8±2.6 | 84.1±3.6 | .40/.42/.32/.13 |
| Internal Rotation | 83.3±2.2 | 85.6±3.2 | 88.9±3.5 | .007†/.23/.02†/.17 |
*First p-value from ANOVA comparison of the three angle measurements; remainder of p-values from post-hoc tests, with second p-value for comparison of 0° versus 20°; third p-value for comparison of 0° versus 40°; fourth p-value for comparison of 20° versus 40°. †Denotes statistical significance
Angled Osteotomies
Repeated measures ANOVA showed that LDTA and ADTA measurements were significantly different based on the degree of angulation in internal rotation angulation and LDTA in external rotation in angled osteotomy [Table/Fig-4]. Significant differences were found in LDTA measurements between 0° and 40° in external rotation and between 0° and 20° and 0° and 40° in internal rotation, as well as ADTA measurements between 0° and 40° in internal rotation.
Discussion
By using three-dimensional reproductions of specimens with tibial deformities, the primary goal of this study was to analyse whether variances in distal tibial cut angles during osteotomies, significantly impact ankle alignment in the coronal and sagittal planes. No prior study in the literature has investigated that how the angle of distal tibial osteotomies affects ankle alignment in patients with rotational deformities. The results of present study demonstrated that a distal tibia osteotomy cut parallel to the distal joint surface (angled with respect to the shaft) results in unanticipated coronal and sagittal plane deformity, while a cut perpendicular to the axis of the tibial shaft did not cause unintended deformity based on previously defined alignment values [14]. Such deformities were more pronounced with greater degrees of rotational correction and correction of internal tibial torsion based on LDTA and ADTA measurements.
The reason for larger differences with angled osteotomy in the internal versus external tibial torsion is unclear. One might question whether this was because the average internal rotational deformity for our sample set was smaller than the average external rotational deformity sample set (16.4° versus 29.6°). Thus, in the internal tibia torsion specimens, the bones were generally overcorrected, which may impact the overall anatomy. However, LDTA was already significantly changed with rotation from 0 to 20 degrees in the internal tibial torsion specimens, before any meaningful overcorrection.
In cases with more complex tibial deformity, such as a combination of rotational, translational and angulation deformity, variations in distal osteotomy cut angle could potentially be performed to correct deformities in the coronal and sagittal planes, using a similar approach to that recommended by Rab GT in the proximal tibia [12]. However, given that the study did not have symmetric results with internal versus external rotation in this study; one can question how predictable such an approach might be, as it may be affected by the rotational orientation of the distal tibia articular surface. Instead, a more standard osteotomy approach for multiplanar deformity is recommended, and the primary application of this study is the importance of making the tibial cut orthogonal to the axis of the shaft in purely derotational osteotomies.
Limitation
This study was not without limitation. First, the present study’s osteotomy methodology isolated the tibial component of the ankle joint which does not take into account potential effects of the adjacent fibula. However, one would expect an intact fibula to affect the angle of the distal tibia only if the tibia was restricted from maintaining a flush position at the osteotomy, which would likely prompt the surgeon to osteotomise the fibula. Secondly, this study utilised a relatively small sample size. We felt that this was reasonable given that the osteotomies were virtually created and rotational amounts marked on the three-dimensional prints, thus greatly improving the accuracy of our physical model. Future studies may build upon our findings with a larger sample set, narrower intervals of rotational correction, and variances in osteotomy cut. This would create a more robust model of how angled de-rotational osteotomies change ankle alignment in the coronal and sagittal planes, and potentially provide enough data to guide surgeons in purposeful multi-planar correction similar to the Rab GT osteotomy in the proximal tibia [12]. Another limitation is that the specimens consisted of adult skeletons, which is questionable, as to whether there is external validity to a paediatric population in which the majority of tibial osteotomies occur. This study design was based on the fact that it would be very difficult to obtain advanced imaging of the entire tibia in a suitable quantity of patients with significant internal and external tibial torsion otherwise. In addition, derotational tibial osteotomy is more commonly performed in patients nearly or past skeletally mature, as remodeling is possible in younger children and significant symptoms often at times do not develop until adolescence. Finally, instead of utilising living patients with rotational deformities, investigating cadaveric specimens does not allow the opportunity to conclude whether our described changes in angle alignment have any clinically measurable effect on short and long-term outcome including ankle stability, ambulation, functional abilities and cosmetic appearance within the paediatric population.
Conclusion
In conclusion, tibial osteotomies are an important surgical management strategy for patients with severe and symptomatic tibial rotational deformities. This study is the first to show that angled distal tibial osteotomies impose statistically significant changes in ankle alignment compared to transverse distal tibial osteotomies. Understanding the subtleties of these changes may help orthopaedic surgeons when treating patients with rotational deformities with contaminant coronal and sagittal deformities in the future. But more importantly the study emphasises that in a purely rotational osteotomy, inadvertent angular deformity can result if the osteotomy cut is not perpendicular to the axis of the tibial shaft.
*Rotational deformity measurement of left tibia
M: Male; F: Female; AA: African American; C: Caucasian