The cervical vertebrae are smallest of the moveable vertebrae and are characterized by a foramen in each transverse process. The transverse process is morphologically composite around the foramen transversarium. Its dorsal and ventral bars terminate laterally as corresponding tubercles which are connected lateral to foramen, by the costal lamellae. In all but the seventh cervical vertebra, the foramen transversarium normally transmits the vertebral artery, vein and vertebral nerve (a branch from cervicothoracic ganglion) [1].
In nearly 90% of cases, vertebral artery usually enters into foramen transversarium of 6th cervical vertebrae but it may also enter cervical vertebrae column through C3 (1%), C4 (2%), C5 (5%) or C7 (2%) [1].
Foramen transversarium gives passage to vertebral artery, vertebral vein and sympathetic fibres from inferior cervical ganglion while C7 vertebra transmits only the vein. Foramen transversarium of C7 may be small or even absent [2]. Variations in Foramina Transversaria (FT) with respect to size, shape, multiplicity or absence of foramina are not uncommon [3]. Accessory costo-transverse foramen was described by Frazer who described it to be present in all cervical vertebrae except C1 and C2. It was said to be divided by a fibrous or bony bridge, separating artery and veins. The smaller posterior part is for a vein or vertebral nerve branch or for fenestrated/duplicated vertebral artery [4].
Pathological conditions may encroach these accessory foramina and can cause hearing loss and cerebral vascular changes [5]. Deformities and different types of variations in FT may affect normal anatomical course of neurovascular structures and may result in various pathological symptoms. It is an established fact that vertebral vessels are an important factor in the formation of FT and reverse is true also. Thus embryological factors may contribute to variations in FT [6].
Variations in number and size of FT may cause vertebral vascular insufficiency leading to neurological symptoms like headache, migraine, fainting attacks [7]. Anatomical details of FT are important for surgeons and radiologist.
Not many studies describing detailed morphology of FT and accessory FT are available in literature. Most of the reported studies have been conducted on random cervical vertebrae. Thus, the aim of present study was to study morphometric details of FT and incidence of accessory FT in all cervical vertebrae of human vertebral column.
Materials and Methods
A total of 319 FT of 161 dry cervical vertebrae of 23 complete human vertebral spines were analysed for this observational study. These vertebral spines were procured from the bone collection of Department of Anatomy at Lady Hardinge Medical College, Delhi, India.
Data on age and sex of individuals from which these vertebral spines were derived was unavailable. All cervical vertebrae were studied macroscopically. Anteroposterior and transverse diameters of FT were measured bilaterally, using a digital vernier calliper with 0.01 mm accuracy. The calliper was placed within each foramen and the widest anteroposterior and transverse diameters were measured. Measurement of diameters could not be done in two C7 vertebrae with missing FT (unilateral in one; bilateral in another). Also, the presence of Accessory Foramina Transversaria (AFT) in each cervical vertebra was observed. A 24 gauze needle was passed through each accessory foramen, if present, for the confirmation of their patency. All significant transverse foramina were photographed and documented.
Statistical Analysis
Statistical evaluation was done for each measurement. The mean, range, standard deviation, p-value were calculated in cervical vertebrae from C1-C7 both on right and left sides in all vertebral spines. These analysis were done to observe and compare different linear parameters of FT of cervical vertebrae.
Results
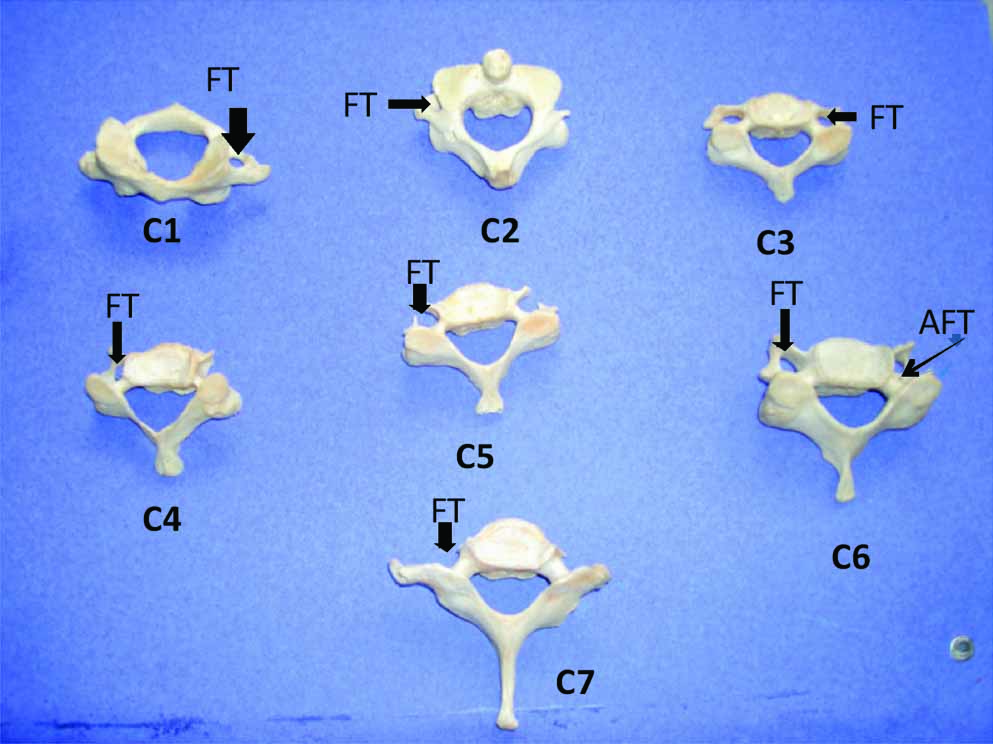
The FT present in the transverse processes of cervical vertebrae showed wide range of variations [Table/Fig-1].
Cervical vertebrae from C1 to C7; superior view showing (FT)-foramen transversarium and (AFT) accessory foramen transversarium.
The transverse diameters of right transverse foramina varied from 2.44 mm to 8.76 mm with a mean diameter of 5.78±1.10 mm. Where as, the anteroposterior diameters of right transverse foramina showed range from 1.91 mm to 8.65 mm with a mean diameter of 5.21±1.15 mm. The transverse diameters of left transverse foramina showed wide variation from 2.53 mm to 8.56 mm with a mean diameter of 5.84±1.03 mm. The anteroposterior diameters of left transverse foramina ranged from 2.12 mm-8.47 mm with a mean diameter of 5.26±1.12 mm. Though transverse and anteroposterior diameters were on a higher note on left side, this difference was not found to be statistically significant.
Comparison was also done between mean transverse and anteroposterior diameters of FT of individual cervical vertebrae from C1-C7. The comparison showed that statistically significant difference was present between mean transverse and anteroposterior diameters of FT of C1, C3, C4, C5 and C7 cervical vertebrae of both right and left side.
On the other hand, cervical vertebrae C2 and C6 showed no statistically significant difference between mean transverse and anteroposterior diameters of FT of right as well as left side.
Mean diameters of transverse foramina of right and left side showed wide range of variations in individual cervical vertebrae from C1-C7 [Table/Fig-2]. Still when compared between right and left side from C1-C7 individual cervical vertebrae, these changes were found statistically insignificant.
Dimensions of foramina transversaria on right and left side in cervical vertebral column (C1-C7).
| Vertebra | Right | Left |
|---|
| Diameters (mm) | No. | Mean | SD | Range | Diameters (mm) | No. | Mean | SD | Range |
|---|
| C1 | AP | 23 | 6.74 | 1.05 | 4.75-8.65 | AP | 23 | 6.56 | 1.00 | 4.92-8.47 |
| TD | 5.85 | 0.83 | 4.75-7.55 | TD | 5.87 | 1.03 | 4.07-8.56 |
| Mean D | 6.30 | 0.68 | | Mean D | 6.21 | 0.69 | |
| C2 | AP | 23 | 5.28 | 0.84 | 4.03-7.46 | AP | 23 | 5.46 | 0.69 | 4.34-6.96 |
| TD | 5.07 | 0.82 | 3.70-6.81 | TD | 5.31 | 0.83 | 3.76-7.06 |
| Mean D | 5.18 | 0.76 | | Mean D | 5.39 | 0.64 | |
| C3 | AP | 23 | 5.03 | 0.58 | 3.87-6.52 | AP | 23 | 4.72 | 0.49 | 3.99-5.72 |
| TD | 6.22 | 0.93 | 4.09-7.58 | TD | 6.36 | 0.54 | 5.52-7.66 |
| Mean D | 5.62 | 0.68 | | Mean D | 5.54 | 0.40 | |
| C4 | AP | 23 | 4.88 | 0.88 | 3.29-6.73 | AP | 23 | 5.03 | 0.84 | 2.69-6.80 |
| TD | 6.10 | 0.92 | 4.06-7.86 | TD | 5.94 | 0.84 | 3.86-7.70 |
| Mean D | 5.49 | 0.81 | | Mean D | 5.49 | 0.74 | |
| C5 | AP | 23 | 5.01 | 0.91 | 1.91-6.20 | AP | 23 | 5.28 | 0.92 | 2.12-7.21 |
| TD | 6.00 | 1.17 | 2.44-7.61 | TD | 5.96 | 1.00 | 2.74-7.18 |
| Mean D | 5.51 | 0.97 | | Mean D | 5.62 | 0.87 | |
| C6 | AP | 23 | 5.25 | 1.01 | 2.95-6.97 | AP | 23 | 5.20 | 1.27 | 2.27-7.28 |
| TD | 5.67 | 1.10 | 2.52-8.06 | TD | 5.74 | 1.33 | 2.53-7.41 |
| Mean D | 5.46 | 0.98 | | Mean D | 5.47 | 1.22 | |
| C7 | AP | 23 | 4.04 | 1.42 | 0.00-6.92 | AP | 23 | 4.12 | 1.77 | 0.00-6.78 |
| TD | 5.27 | 1.85 | 0.00-8.76 | TD | 5.18 | 2.05 | 0.00-8.28 |
| Mean D | 4.66 | 1.49 | | Mean D | 4.65 | 1.81 | |
*The difference in number of foramina in C7 is due to exclusion of absent foramina.
Double foramina transversaria- A total of 42 vertebrae out of 161 cervical vertebrae (26.09%) showed presence of AFT [Table/Fig-3]. Here, 32 AFT were on right side while 27 were on left side.
Frequency/incidence of accessory foramina transversaria on right and left side in cervical vertebral column (C1-C7).
| Number of Accessory Foramen | C1 | C2 | C3 | C4 | C5 | C6 | C7 |
| Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left |
| 0 | 0 | 0 | 0 | 0 | 1 | 7 | 3 | 8 | 5 | 11 | 14 | 6 | 4 |
| Unilaterally Present AFT | 0 | 0 | 0 | 0 | 0 | 1 | 4 | 0 | 5 | 2 | 1 | 4 | 5 | 3 |
| Bilaterally Present AFT | 0 | 0 | 0 | 3 | 3 | 10 | 1 |
| Absence of MFT | NIL | NIL | NIL | NIL | NIL | NIL | 2 | 1 |
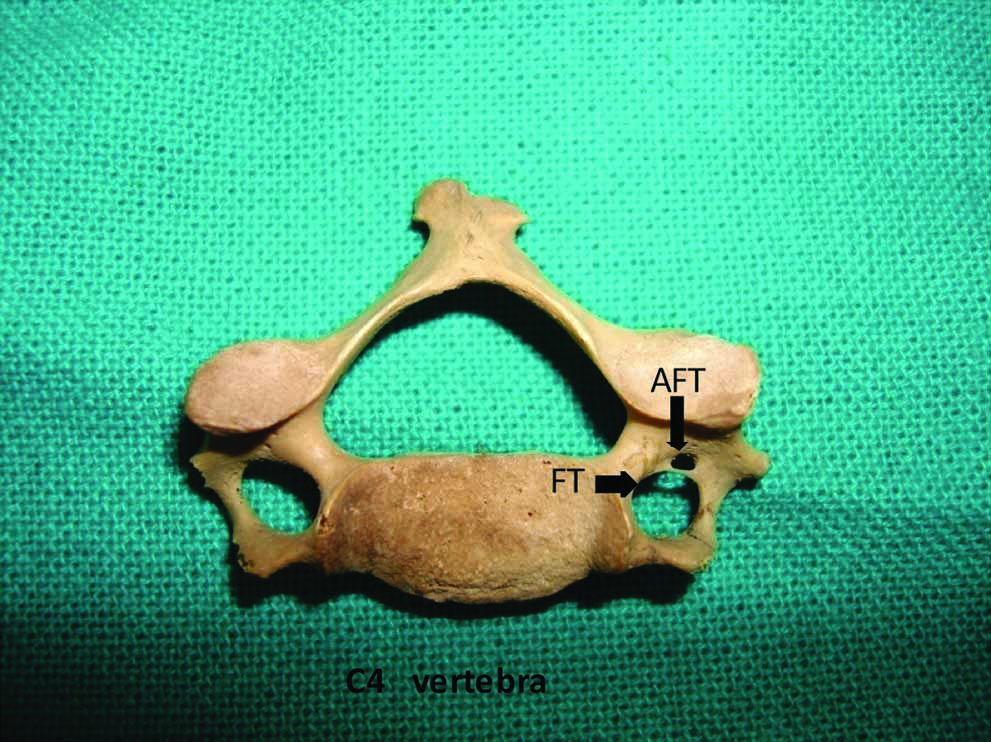
Incidence of cervical vertebrae with unilateral AFT was 15.53% (25 vertebrae out of 161) [Table/Fig-4];
C4 cervical vertebra; superior view showing Unilateral Accessory Foramen Transversarium (UAFT), Foramen Transversarium (FT).
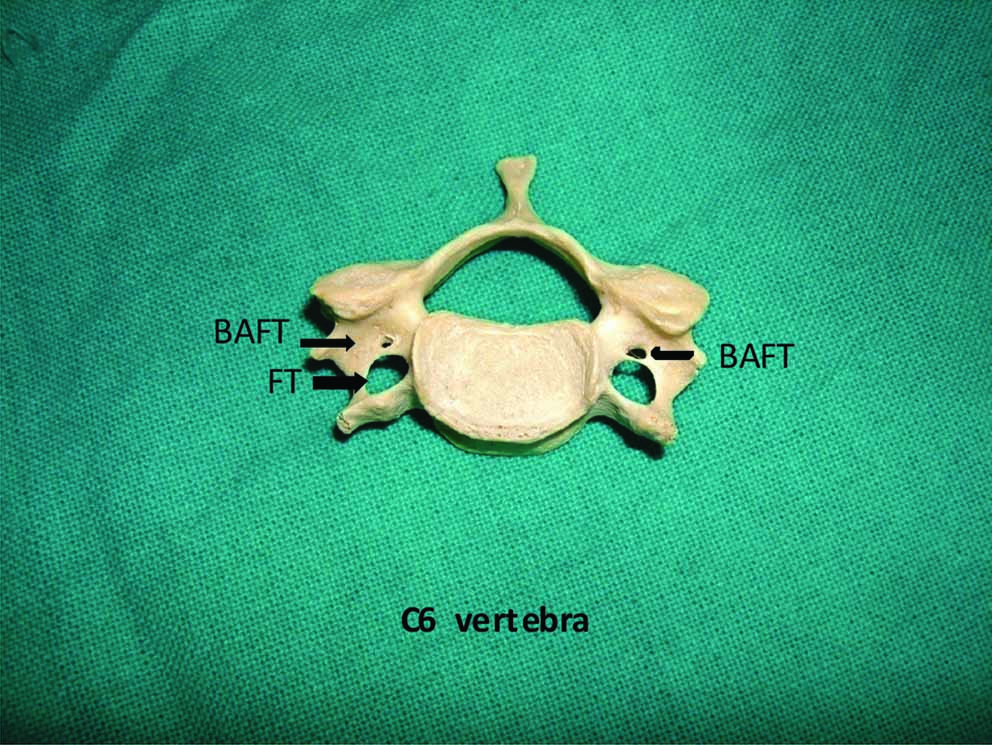
Incidence of cervical vertebrae with bilateral AFT was 10.56% (17 vertebrae out of 161) [Table/Fig-5];
Cervical vertebrae C6; superior view showing Bilateral Accessory Foramen Transversarium (BAFT), Foramen Transversarium (FT).
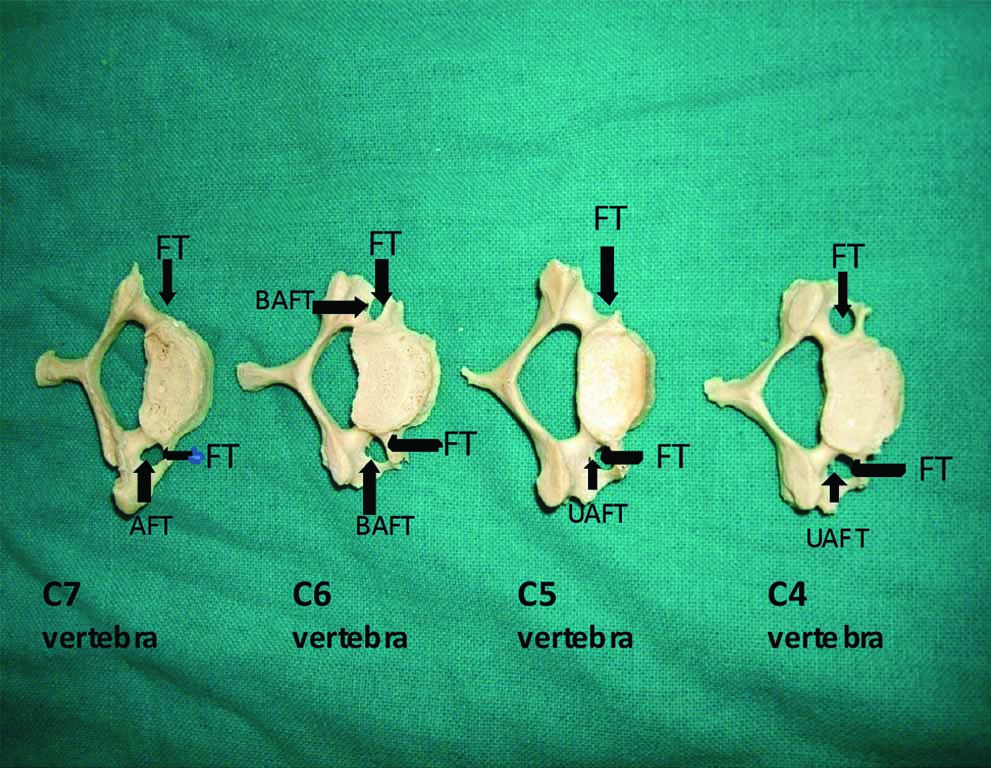
C1 and C2 cervical vertebrae showed no AFT where as only one C3 cervical vertebrae showed presence of unilateral AFT. AFT were mainly present in lower cervical vertebrae (C4-10, C5-13, C6-25, and C7-10) [Table/Fig-6];
Cervical vertebrae C4, C5, C6 and C7; superior view showing Unilateral Accessory Foramina Transversaria (UAFT) in C4, C5 and C7 cervical vertebrae; Bilateral Accessory Foramen Transversarium (BAFT) in C6 cervical vertebra
The position of AFT in relation to main FT was always posterior to main FT except in one C4 vertebrae of left side which showed presence of AFT anterior to main FT.
Size of AFT to main FT was always smaller.
Main Foramen Transversarium (FT)- Absent FT- One C7 vertebrae showed bilateral absence of FT while another C7 showed unilateral absence of FT.
Discussion
Pattern of size of main FT
According to available literature, the two vertebral arteries are unequal in size in about 75% of individuals, out of these right sided artery may be extremely narrow in 10% of individuals [8].
In the present study, left FT was larger than right FT, but no statistically significant differences were observed between the mean transverse diameters of right and left side. These results resemble a previous study conducted by Sangari SK et al., who compared them between different typical cervical vertebrae [9]. Similar findings like above observations were also reported in another study done by Taitz C et al., [6]. He showed that mean values for left FT from vertebral levels C3 to C7 were on higher side than right [6]. In few more studies carried out by Kaya S et al., and Epstein mention that left FT are larger than right FT but like Taitz C et al., these also didn’t compare them statistically [6,10,11].
Taitz C et al., reported that FT of C1 had highest mean values whereas FT of C7 showed lowest mean values. This finding is similar to our observations in the present study. [6]
In a slight variation to the above findings, another study by Ebraheim NA et al., reported that diameters of FT increase from C3 to C5 and then decrease at C6 [12].
In present study, we also compared anteroposterior and transverse diameters of cervical vertebrae from C1 to C7. We observed that statistically significant difference was present between mean transverse and anteroposterior diameters of FT of C1, C3, C4, C5 and C7 cervical vertebrae of both right and left side. On the other hand, cervical vertebrae C2 and C6 showed no statistically significant difference between mean transverse and anteroposterior diameters of FT of right as well as left side. This finding gives us idea about changing shapes of FT.
Previously, Taitz C et al., studied shapes of FT. Though, he didn’t compare them statistically but used a formula of coefficient of roundness which is similar to our findings. [6]
It is said that variation in course or diameters of vertebral artery is a factor in formation of FT, thus it can be assumed that variation in presence and course of vertebral vessels will manifest in the variations of size and number of FT and vice-versa will also hold true [6].
Vertebral artery develops from the fusion of longitudinal anastomoses linking second to sixth cervical intersegmental arteries. Most of the intersegmental arteries regress except seventh cervical intersegmental artery which forms first part of vertebral artery [13]. It is postulated that the failure of occlusion of intersegmental arteries may be responsible for duplication or fenestration of vertebral artery. A duplicate vertebral artery may help to protect patients against ischemic brain attacks and provide collateral blood circulation to basilar artery. However, fenestrated vertebral artery has been demonstrated microscopically having weak vessel wall with irregular elastic fibres [14]. Also, both double and fenestrated vertebral arteries are associated with risk of thrombus formation and embolization resulting in transient ischemic attacks [9].
Zibis A et al., suggested that variations in FT (identified in cervical spine CT) are a good indicator of vertebral artery variations. Also, variations in vertebral artery (found in ultrasonography) clearly points towards FT variations. Therefore, these incidental findings should be thoroughly investigated before planning a spine surgery [15].
Accessory Foramina Transversaria (AFT)
Taitz C et al., conducted a study on 480 cervical vertebrae and found 34 vertebrae with double FT. Among 34 vertebrae; six vertebrae had double foramina of equal size while others were with AFT of small dimensions. He also observed four vertebrae with no FT and one vertebra with triple foramen transversarium [6].
Jaroslaw W et al., reported presence of total 167 AFT in 100 vertebral column. He said that AFT were most frequently present at the level of C6 (45.6%) and were rarest at the level of C3 (2.8%). He found AFTs were always smaller in size than main FT. He also mentioned one C7 vertebrae having no AFT and one C7 vertebra with triple foramen transversarium [16].
Sangari SK et al., reported 17 typical vertebrae (24%) out of 71 having AFT. He also found that the position of AFT was always posterior to main FT and size of AFT was always smaller than main FT [9].
Murlimanju B et al., found that six cervical vertebrae (1.6%) out of 363 having AFT. He observed four cases out of 363 with absent FT and one C6 vertebra with triple foramina. AFT were more on left than right side. He found AFT was always smaller than main FT [17].
Another study by Das S et al., done on 132 cervical vertebrae documented presence of double FT only in 2 vertebrae (1 unilaterally, 1 bilaterally) [3].
In the present study, 42 cervical vertebrae (26.09%) out of 161 showed presence of AFT in their transverse processes.
In present study, unilateral presence of AFT was more prevalent than bilateral AFT, as shown by 25 vertebrae with unilateral AFT (15.53%) and 17 vertebrae with bilateral AFT (10.56%). The finding showing unilateral predominance of AFT was also observed in a study done by Murlimanju B et al., [17]. Taitz C et al., conducted a study on 480 cervical vertebrae and found 34 vertebrae with double FT. Among 34 vertebrae; six vertebrae had double foramina of equal size while others were with AFT of small dimensions. He also observed four vertebrae with no FT and one vertebra with triple foramen transversarium [6]. In our study, AFTs were most frequently present in C6 vertebrae. This finding coincides with findings of previous studies [6,16].
In a recent CT angiographic study, the author correlated the common occurrence of double transverse foramina at C5-C6 vertebrae with more clinical symptoms such as acute headache, vertigo, vomiting observed in subjects with double FT after whiplash injuries. He explained that it may be due to most pronounced bending movements occurs at the level of C5-C6 vertebrae during whiplash [18].
In the present study, AFTs were always found to be smaller than main FT. This observation is similar to previous studies conducted by Taitz C et al., Sangari SK et al., Jaroslow W et al., Murlimanju B et al., and many more [6,9,16,17].
In the present study, AFTs were observed in C3, C4, C5, C6, C7 where as they were absent in C1 and C2. AFTs were mostly present in lower cervical vertebrae C4, C5, C6, and C7. These results resembles with studies done by previous authors. Although Taitz C et al., and El Shaarawy EAA et al., found that AFTs were present in lower cervical vertebrae (C5, C6, C7), maximally in C6 (19 vertebrae) [6,19].
Murlimanju B et al., also found AFTs in C6, C7 but not in other cervical vertebrae [17].
On the other hand, Jaroslaw W et al., found AFTs in C3-C7 cervical vertebrae and Kaya S et al., who reported a single C4 vertebra showing unilateral AFT [10,16].
Study done by De Boeck M et al., documented the presence of AFTs in 17% of C1 and C2 dry cervical vertebrae [5]. But our study, and the other above mentioned studies except De Boeck M et al., showed absence of AFTs in C1 and C2 vertebrae.
It is important to point out that our study was done on intact cervical vertebral column unlike all other previous studies except studies done by Taitz C et al., Jaroslaw W et al., which gives better comparison [6,16]. Both Jaroslaw W and our study reported AFTs in C3 and C4 vertebrae while Taitz C et al., didn’t report any [6,16].
In view to compare presence of AFTs in intact vertebral column we compared our study with De Boeck M et al., who studied both dry cervical vertebrae C1 and C2 as well as CT images of cervical spines [5]. In CT images, he found one AFT in C1 vertebra and 5% frequency of C3 and 5% frequency of C4. This radiological study done by De Boeck M et al., further strengthen this understanding that as most of the studies were done on the random samples of cervical vertebrae; in order to understand, more studies should be done on intact vertebral column to estimate frequency of AFTs. Also, radiological studies like CT and MR angiography can be combined with anatomical studies for better insight in future.
Limitation
In the beginning of our study, we wanted to incorporate radiological images of cervical spines along with dry cervical vertebrae to make this a comparative study. But, we later on limited our focus only on dry cervical vertebrae as the data was already extensive. Still, we believe that morphometric data of dry cervical vertebrae can be compared with data collected taking similar parameters from radiological images of cervical spine so that a complete morphometric data is obtained for future references.
Conclusion
Anatomy of cervical spine is important for surgeons operating in this region as well as for radiologist examining radiological images of the area such as CT and MRI scans. Thus, as this study has provided a detail morphometric data showing variations in size, shape and number of FT as well as in AFT in the region of cervical spine. This would be useful in better understanding the cervical region. Moreover, the common occurrence of variations found in FT and AFT highlights the importance of detailed preoperative radiological evaluation in order to rule out any of these common anatomical variations for a better surgical outcome.
*The difference in number of foramina in C7 is due to exclusion of absent foramina.