Crossed Fused Renal Ectopia showing Pelviureteric Junction Obstruction with Single Ureter and Single Renal Artery
Rahul Dev1, Gitanjali Khorwal2, Mohit Tayal3, Vibhu Goel4, Udit Chauhan5
1 Assistant Professor, Department of Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
2 Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
3 Senior Resident, Department of Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
4 Consultant Radiologist, Aarna Diagnostic Centre, Kargi Chowk, Dehradun, Uttarakhand, India.
5 Assistant Professor, Department of Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rahul Dev, Flat No-5/1, Building No-57, AIIMS Rishikesh Residential Complex, Rishikesh-249203, Uttarakhand, India.
E-mail: rdev8283@gmail.com
Crossed fused renal ectopia is a rare anomaly remaining asymptomatic by far and detected invariably as either incidental finding or in view of pre-existing kidney disease. We report a case of crossed fused renal ectopia presenting as lumbar pain in a young female patient with no associated calculus or cystic kidney disease. It was an inferior type of renal ectopia on right side drained by a common artery and common ureter along with additional aberrant vascular supply. Multidetector computed tomography with multiplanar and three dimensional reconstruction helps in the proper delineation of renal fusion and ureteric anomaly if any, as well as mapping of aberrant vascular supply.
Aberrant vascular, Contrast enhanced computed tomography, Ectopic kidney, Fusion anomaly, Hydronephrosis, Urography
Case Report
A 20-year-old young female patient presented with dull aching recurring right lumbar pain for the last one year. The patient underwent Ultrasonography (USG) of abdomen at a different centre, which revealed empty left renal fossa. In addition, the USG showed both kidneys present on the right side, deformed in shape with a variable degree of fusion. There was presence of hydronephrosis with no obvious calculus disease. There was no clear demarcation between pelvis of either kidney. Similarly, on colour doppler individual renal arteries were not separately visualised. All laboratory parameters including renal function tests were within normal limits. The patient underwent Contrast Enhanced Computed Tomography (CECT) (after taking the due formal consent) to rule out calculus disease for right lumbar pain which might not have been excluded due to complex fusion anomaly. In addition, excretory phase imaging was added to look for any renal pelvic fusion or ureteric duplication, which could not be ascertained on USG. Non-contrast scans showed hydronephrosis with no calculus disease [Table/Fig-1]. CECT urography showed left kidney on the right side of the abdomen with the superior pole of ectopic left kidney fused to the inferior pole of orthotopic right kidney with a waist like constriction demarcating point of fusion. The pelvis of both kidneys were dilated and partially fused, associated partial pelviureteric junction obstruction and formation of common right ureter entering into the urinary bladder at right vesico-ureteric junction. The left ureter was absent. Uterus and both ovaries were present with normal appearance [Table/Fig-2,3]. The right kidney was supplied by the right renal artery originating from the aorta whereas inferior ectopically placed left kidney was supplied from ileocolic/right colic branches of superior mesenteric artery [Table/Fig-4]. The venous drainage was through the right renal vein as well as through smaller aberrant veins supplying the inferior ectopic kidney and draining into the inferior vena cava. No skeletal anomalies were visualised in dorsolumbar spine or pelvis. The patient was advised to undergo USG abdomen for evaluation of the kidneys so as to follow-up for any increase in degree of hydronephrosis, development of any calculus disease or any of its complications. The patient was also advised to undergo USG abdomen on an emergency basis if she develops any unexplained severe abdominal pain, episode of haematuria, high grade fever or unexplained and or significant weight loss. The patient came to department of radiodiagnosis and imaging recently after one year for follow-up USG scan with no significant complaints during the said duration. The USG scan showed no significant change in findings as compared to previous scan.
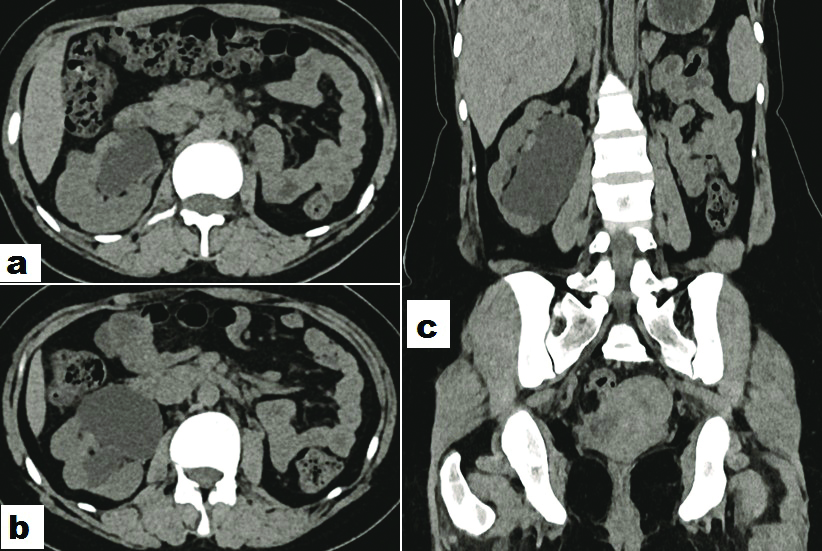
Axial (a and b) and coronal (c) noncontrast multiplanar reconstructed images shows hydronephrosis involving crossed fused ectopic kidney, however no hyperdense calculus or haemorrhage seen within the pelvicalyceal system with no area of parenchymal calcification.
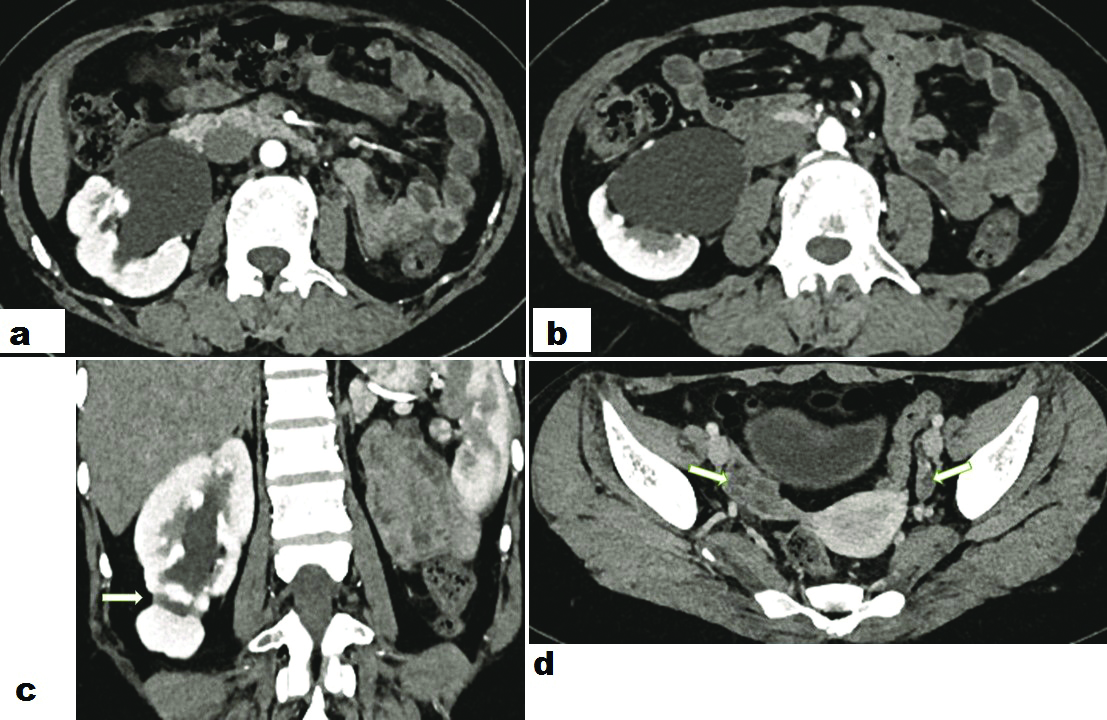
Axial contrast enhanced images show anteriorly directed renal pelvis with associated hydronephrosis (a and b). Coronal multiplanar reconstructed image shows waist (white arrow in c) demarcating point of fusion. The axial image through the pelvis shows presence of and normal appearance of the uterus and both ovaries (white arrows in d).
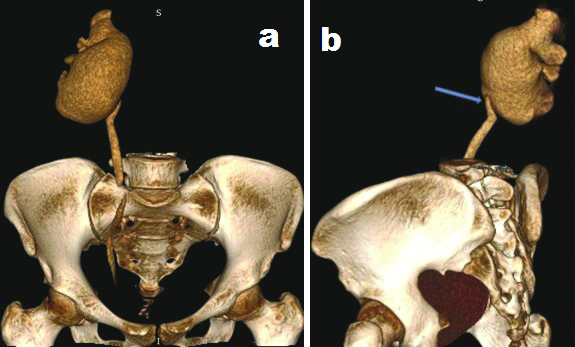
Volume rendered anterior (a) and lateral oblique (b) images show dilated renal pelvis, narrowing at pelviureteric junction (thick blue arrow in b) with visualisation of right ureter and non-visualisation of left ureter.
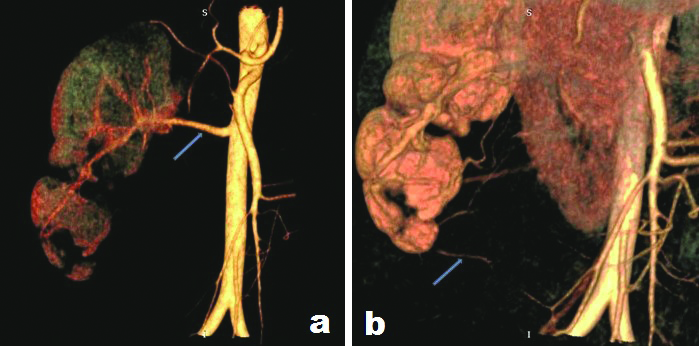
Volume rendered images depict upper pole kidney being supplied by the single right renal artery (thin blue arrow in a) and lower pole kidney supplied by a branch of superior mesenteric artery (thin blue arrow in b).
Discussion
Crossed fused renal ectopia is one of the rare anomalies of the kidney and occurs when a kidney is located and fused to the kidney on the side opposite to the side from which its ureter enters into the urinary bladder. Although it remains asymptomatic in the majority, in some cases it may be associated with hydronephrosis, calculus and reflux disease, recurrent infections, cystic renal dysplasia and congenital anomalies [1]. The kidney starts developing around the fourth week of gestation due to interaction between ureteric bud and metanephric blastema. The mesonephric duct gives rise to ureteric bud which in turn develops into the pelvicalyceal system and collecting tubules. From sixth to ninth week of gestation the kidneys ascend from native sacral region to the lumbar region adjacent to posterior abdominal wall successively receiving arterial supply from sacral and iliac vessels and finally aorta. After completion of the ascent of the kidney it undergoes rotation along its long axis so that the renal pelvis is finally anteriorly directed. Fused kidneys are usually prevented from ascending to their normal position and remain in an ectopic position. In renal fusion anomalies, the vascular supply is grossly anomalous, similar to that of ectopically located kidneys by virtue of limited cranial migration. Crossed fused renal ectopia is a rare type of renal fusion anomaly in which both the kidneys are located on either side of the midline and in the vast majority of such cases, the crossed ectopic kidney is fused with the orthotopic located kidney. This entity often remains clinically silent as supported by several case reports in cadavers [2]. At the same time cases which are symptomatic commonly present with pain, palpable lump, haematuria and or urinary tract infection. One of the first classifications of renal fusion anomalies was given by McDonald and McClellan who divided ectopic kidney into four types depending upon whether ectopia is unilateral or bilateral and associated renal fusion if any [3]. The left to right ectopia and fusion is a more common phenomenon with male preponderance. Further crossed fused ectopia was classified into six anatomical variants, namely the inferior pole fusion type, sigmoid kidney, lump kidney, disc kidney, L-shaped kidney and superior pole fusion type in decreasing order of frequency [3]. The accurate mechanism of occurrence of crossed fused renal ectopia is not fully mapped and consequently many postulates have been proposed as explanation. Among them are the genetic theory postulating familial inheritance of the anomaly in identical twins as well as siblings by highlighting the importance of sonic hedgehog gene signal, mechanical theory postulating umbilical arterial fork, preventing cranial migration of metanephros and a close approximation of the kidneys, disturbed spatial relation of nephrogenic blastema and ureteric bud as proposed by theory of abnormal rotation of the caudal end of the fetus [4,5]. The ectopic kidney derives its blood supply from ipsilateral renal vessels in majority of cases, infrequently from the contralateral side with both kidneys having aberrant vascular morphology [6,7]. Kaur N et al., reported a case of cross fused ectopia with common right ureter [8]. It is also associated with many other congenital anomalies pertaining to other organ systems [9,10]. In the absence of complications and associated additional abnormalities, the prognosis for a patient with crossed fused renal ectopia is very good. There are no specific primary treatment approaches for the management. Treatment of the associated pathologies is indicated which are most frequently renal calculi and vesicoureteral reflux. It is important to remember that mapping of aberrant vascular anatomy is vital before planning any surgical intervention.
Conclusion
Crossed fused renal ectopia is an uncommon congenital anomaly which remains asymptomatic throughout life in majority of the population, found incidentally when patients are investigated for other abdominal pathologies. In a minority of cases, it may be associated with urinary tract infections, calculus disease or associated congenital malformations affecting other organ system. We are reporting a rare case of the inferior pole crossed fused renal ectopia on the right side showing variable fusion of renal pelvis of both kidneys with a common ureter and common right renal artery. USG is the first line modality for evaluation of such condition as it readily identifies presence of hydronephrosis or calculus disease if any. USG is also used as a modality of choice for follow-up imaging for evaluation of hydronephrosis, calculus disease or its complications as well as for evaluation of any unexplained weight loss. However, in cases of complex fusion anomaly as in the present case CECT with multiplanar reconstruction provides excellent anatomical details of this anomaly. In the present case, CECT excluded any small calculi as well as infective complication and at the same time delineated anomalous vascular supply to inferior kidney as well as renal pelvic fusion and presence of single ureter.
[1]. Sharma V, Ramesh Babu CS, Gupta OP, Crossed fused renal ectopia: Multidetector computed tomography studyInt J Anat Res 2014 2(2):305-09. [Google Scholar]
[2]. Karambelkar RR, Nikumbh RD, Nikumbh DB, Shewale AD, A rare case study: crossed fused renal ectopia. Inferior ectopia type with brief review of literatureJ Anat Photon 2013 113:127-29. [Google Scholar]
[3]. McDonald JH, McClellan DS, 1957. Crossed renal ectopiaAm J Surg 1957 93:995-99.10.1016/0002-9610(57)90680-3 [Google Scholar] [CrossRef]
[4]. Shapiro E, Bauer SB, Chow JS, Anomalies of the upper urinary tract. In: Alan J Wein (Ed)Campbell-Walsh UrologyVol. 410th EdPhiladelphiaElsevier SaundersChapter 117, Pp. 3145 [Google Scholar]
[5]. Cook WA, Stephens FD, Fused kidneys: morphologic study and theory of embryogenesisBirth Defects Orig Artic Ser 1977 13(5):327-40. [Google Scholar]
[6]. Bauer SB, “Anomalies of the upper urinary tract,” in Campbell’s Urology, Walsh PC, Retik AB, Vaughan ED, Wein AJ, Eds., pp. 1898-1906 2002 8th editionPhiladelphia, Pa, USAWB Saunders [Google Scholar]
[7]. Bailey SH, Mone MC, Nelson EW, Transplantation of crossed fused ectopic kidneys into a single recipientJ Am Coll Surg 2002 194(2):147-50.10.1016/S1072-7515(01)01137-1 [Google Scholar] [CrossRef]
[8]. Kaur N, Saha S, Mriglani R, Saini P, Gupta A, Crossed fused renal ectopia with a single ureter: A rare anomalySaudi J Kidney Dis Transpl [serial online] 2013 [cited 2018 Nov 29] 24:773-76.10.4103/1319-2442.11388123816729 [Google Scholar] [CrossRef] [PubMed]
[9]. Suthar KD, Mewada BN, Crossed fused renal ectopia with vaginal agenesis-A case reportAsian J Med Res 2012 1(4):132-33. [Google Scholar]
[10]. Kulkarni R, Appaji CA, Kulkarni RN, Crossed renal ectopia associated with malrotation of intestine-A rare case reportInt J Anat Res 2013 1(2):53-56. [Google Scholar]