Sufficient volume of healthy bone at recipient site is an important requirement for long term success of osseointegrated implants. Owing to conditions such as tumour resection followed by reconstruction with grafts, trauma and severe atrophy, maxillary and mandibular ridges may become compromised [1]. Misch CE et al., has categorized available bone as Divisions A, B, C and D ranging from abundant to severely resorbed bone. Compromised and atrophied ridges, that are grouped as Division C are deficient in one or more dimensions (height <12 mm, width <2.5 mm and crown height space > 15 mm) [2]. The main goal in rehabilitation of compromised ridges is the provision of prostheses with a clinically acceptable fit [3]. The clinical challenges posed by these ridges towards the fabrication of a successful prosthesis relate to increased crown height space acting as a vertical cantilever that causes magnification of stresses thereby aggravating bone loss. The biomechanical complications posed by soft tissue proliferation around prosthetic components, altered maxillomandibular relationship, encroachment of prostheses on adjoining anatomical structures can also be detrimental to the prostheses thereby deteriorating the existing condition [2].
Implant prosthetic rehabilitation is more complex for this category of patients due to altered bone support and increased prosthetic space. Computer-Aided Design and Computer- Aided Manufacturing (CAD/CAM) technology is being successfully advocated in fabrication of implant prostheses resulting in good functional and aesthetic outcome [4]. However, a novice practitioner is challenged in selection of the right CAD/CAM prosthetic option for compromised ridges by the lack of a ready reckoner that lists all available options. An initial literature search identified several individual reports. It was unable to locate a comprehensive summary of evidence in this emerging area. Therefore, it was decided to perform a scoping review to summarise the various CAD/CAM implant prosthetic options available to rehabilitate patients with compromised ridges.
Hence, the objective of this scoping review was to enumerate the various CAD/CAM prostheses available in rehabilitation of implants in compromised maxilla and mandible.
Materials and Methods
The review was performed based on the PCC (P-patient, C- concept, C-Context) approach. The PCC question formulated was: In patients with compromised edentulous maxillary /mandibular ridge (P), what are the different types of CAD/CAM fabricated (C) implant supported prostheses (C) available?
Information Sources and Search Criteria
Initially, an electronic search of literature in English-language published between January 2005 and March 2018 was undertaken on 7th April 2018 in the following databases: MEDLINE and Embase via Ovid.
Search string used was “CAD CAM”, “Computer Aided Design Computer Aided Manufacture”, “dental implantation” OR “implant supported” OR “oral rehabilitation” OR “dental implants”, “dental prosthesis”, “denture framework”, “alveolar bone loss”, “resorbed maxilla” OR “atrophic maxilla”, “resorbed mandible” OR “atrophic mandible”, “compromised maxilla”, “compromised mandible”, “implant framework”, “maxillary neoplasms” or “maxillectomy” OR “reconstruction”, “mandibulectomy”, “bone volume” OR “bone quantity”.
A manual search was also conducted, and related articles not yet included were then added. General internet and Google scholar search was also perfomed to identify industry generated supporting materials of interest.
Study Eligibility Criteria
Studies published in English language and those which satisfied the following criteria were included: Clinical human studies including prospective and retrospective cohorts, case reports, and case series.
Patients with compromised bone such as atrophic ridges, resected jaws reconstructed with grafts, decreased bone quantity.
Studies including partially or completely edentulous patients with a minimum of four teeth missing.
Studies specifying implant supported or retained prostheses fabricated using only CAD/CAM technology.
In-vitro studies, animal studies, technical reports, biomechanical studies, and Finite Element Analysis (FEA) studies were excluded. Frameworks created solely for surgical purpose with no prosthetic solution planned were excluded. Other modes of fabrication techniques like Direct Metal Laser Sintering (DMLS), and Copy-Milling (CM) were not included. Articles which did not mention the type of prosthesis, the compromised condition and the studies done on decreased bone quality were excluded.
Study Selection
Citations retrieved in the database searches were assessed in a two-stage review process. Screening the title and abstract of eligible studies, verification of their potential relevance and full text reading were conducted independently by both the reviewers. Disagreements and conflicts during the extraction were resolved by a third reviewer. Both the reviewers had more than 10 years of experience.
Data Extraction
Extracted data included study type, participants, type of compromised condition, number of implants, ridge and site of implant placement, type of CAD/CAM prosthesis (framework or suprastructure) and the mode of retention.
Results
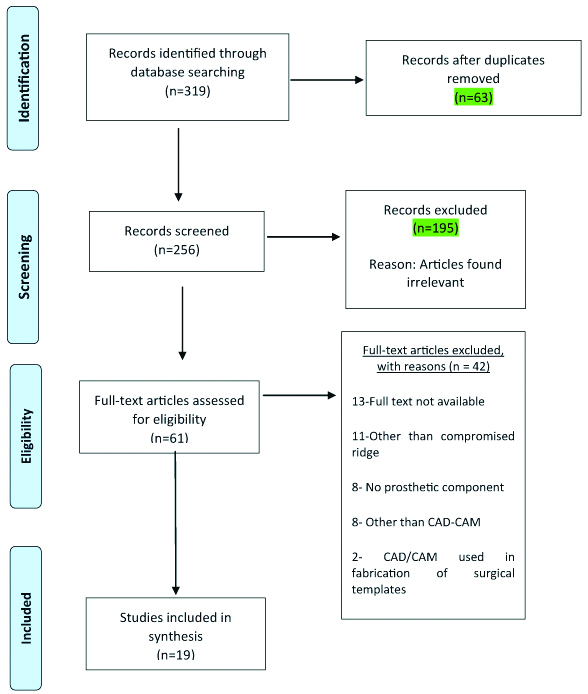
The electronic and manual searches performed in the initial stage yielded 319 records that were considered relevant. After an elaborate screening of titles and abstracts, 63 duplicates were removed. Out of the 256 studies considered for further screening, 195 articles were found irrelevant and rejected, followed by 61 articles eligible for full-text reading. Eventually, 19 articles satisfied the defined inclusion criteria, including 15 case reports that had one patient each and 4 prospective cohorts with more than 5 patients in each. Four industrial reports were included through a separate manual search.
Details on excluded studies and reasons for exclusion are depicted in the study inclusion flowchart [Table/Fig-1].
Study inclusion flowchart.
[Table/Fig-2] Describes in detail the included case reports and prospective cohort studies.
Detailed description of included studies [5-23].
| Study year | Type of study | Number of patients | Type of compromised condition | Number of implants | Ridge/region | Type of CAD/CAM prosthesis (framework/supra structure) | Manufacturer | Mode of retention | Follow-up period |
|---|
| Agustín-Panadero R [5] | Case report | 1 | Severe atrophy of maxilla | 8 | Maxilla full arch | Implant supported overdenture of grade V titanium | TSA | Screw retained | 3, 6 and 12 months |
| Agustín-Panadero R [7] | Case report | 1 | Severe atrophy of maxilla | 4 | Maxilla full arch | Co-Cr framework with ceramic supra structure | 3S | Screw retained frameworks | 12 months |
| Papaspyridakos P et al., [9] | Case report | 1 | Severe atrophy of maxilla/mandible | 5 | Maxilla/mandible full arch | Zirconia framework with feldspathic porcelain supra structure | Nobel Biocare | Screw retained | 6 months |
| Papaspyridakos P et al., [10] | Case report | 1 | Severe mandibular atrophy | 4 | Mandible full arch | Milled Titanium framework with lithium disilicate crowns as supra structure | Nobel BioCare | Screw retained framework | 6 months |
| Bentz RM et al., [8] | Case report | 1 | Severe maxillary and mandibular atrophy | Max 8Mand 6 | Maxilla/mandible full arch | Milled titanium framework veneered with acrylic resin teeth | Nobel BioCare | Screw retained | 2 years |
| Cho Y Et al., [11] | Case report | 1 | Severe atrophy of mandible | 6 | Mandible full arch | Milled zirconia framework with lithium disilicate monolithic crowns | Zirkohnzahn | Cement retained | 9 months |
| Goo CL et al., [12] | Case report | 1 | Knife edge mandibular ridge | 4 | Mandible full arch | Milled titanium bar with acrylic overdenture | Nobel BioCare | Screw retained | 2 weeks |
| Koch FP et al., [13] | Case report | 1 | Mandibular resection and reconstruction with fibula graft | 4 | Mandible full arch | Milled Dolder bar with acrylic overdenture | Astra Dentsply | screw retained | 6 months |
| Oh KC et al., [19] | Case report | 1 | Hemi mandibulectomy and reconstruction with fibula graft | 5 | Hemi mandible | milled polyetherketoneketone(PEKK)framework with PMMA resin crowns | Trione Z | Cement retained | 12 months |
| Rachmiel A et al., [18] | Case report | 1 | Hemi mandibulectomy and reconstruction with customised titanium implant | 2 | Hemi mandible | milled customised Titanium implant with maximum pores for better osseointegration and zirconia crowns | | Screw retained | 12 months |
| Schneider R et al., [17] | Case report | 1 | Hemi mandibulectomy and reconstruction with fibula graft | 6 | Hemi mandible | Milled Titanium framework with acrylic resin teeth | Thommem Medical | Screw retained | 4 years |
| Reshad M et al., [14] | Case report | 1 | Severe atrophy of mandible | 5 | Mandible full arch | Milled titanium framework with zirconia crowns and composite resin replicating gingiva | Biomet 3i | Screw retained framework Cement retained crowns | 12 months |
| Sethi A et al., [15] | Case report | 1 | Severe atrophy of mandible | 4 | Mandible full arch | Milled cobalt chromium framework with porcelain fused to metal copings | Compartis, ISUS | Screw retained | 3 months and 1 year |
| Yoon H-I et al.,[16] | Case report | 1 | Hemi mandibulectomy and reconstruction with fibula graft | 3 | Hemi mandible | Milled zirconia framework with splinted zirconia crowns | 3S | Screw retained framework Cemented crowns | 12 months |
| Al Thobity A et al., [6] | Case report | 1 | Severely deficient maxilla | 6 | Maxilla full arch | Milled titanium framework with lithium disilicate individual crowns | Nobel Biocare | Screw retained framework Cemented individual crowns | 1 year |
| Pozzi A et al., [20] | Prospective cohort | 18Males-7Females-11 | Severe atrophy of maxilla and mandible | Maxilla-36Mandibular -36 | Full archMaxilla-9Mandible-9 | Milled Titanium bar with cast Co-Cr metal framework with overlying acrylic denture. | Nobel Biocare | Screw retained | 12 months |
| Weinstein R et al., [21] | Prospective cohort | 20Males-8Females-12 | Severely atrophied mandible | 80 | Interforaminal-mandible | CAD/CAM milled acrylic prosthesis (CAD/CAM) procera system | Nobel biocare | Screw retained | 12 months |
| Agliardi EL et al., [22] | Prospective cohort | 15Males-2Females-13 | Severely atrophied maxilla | 60 | Zygomatic bone and anterior maxilla | Milled Titanium frameworks with acrylic and ceramic crowns | Nobel biocare | Screw retained framework and cemented crowns | 6 years |
| Seeman R et al., [23] | Prospective cohort | 10Males-2Females-8Females-8 | Severely atrophied mandible | 404 in each patient | Full arch mandible | CAD/CAM milled fiber-reinforced and composite resin-facetted bridge with acrylic teeth | TriniaBicon | Cement retained | 19.5 months |
Description of Included Studies
Characteristics of case reports: All the case reports considered had one patient each, who was compromised in either maxilla or mandible or both owing to severe atrophy or resection from tumours. Among the 15 case reports that were recorded, 3 reports included maxilla [5-7], 2 included both maxilla and mandible [8,9] and 10 included mandible, of which 6 were full arch [10-15] and 4 hemi-mandible [16-19]. Ridges compromised by severe atrophy and resection were reported in 11 and 4 patients respectively [13,17-19]. Based on the quantity and quality of bone, grafting or reconstruction was performed, and implants were placed accordingly. Implant prostheses were fabricated with a framework and supra structure. The material that was used commonly in most of the cases for framework fabrication was titanium. Papaspyridakos P et al., Cho Y et al., and Yoon H-I et al., reported cases where zirconia frameworks were given [9,11,16]. Agustín-Panadero R et al., and Sethi A et al., used metal frameworks made from Cobalt-Chromium (Co-Cr) [7,15].
Oh KC et al., fabricated a CAD/CAM milled framework made from Polyetherketoneketone (PEKK) for a hemi mandibulectomy case that was reconstructed with fibula graft [19]. Rachmiel A et al., fabricated a milled customised titanium implant for a hemi mandibulectomy case, with maximum pores for better osseointegration and restored with zirconia crowns [18]. Agustín-Panadero R et al., Goo CL et al., and Koch FP et al., reported cases where acrylic overdentures retained by bar attachments milled from titanium were inserted [5,12,13].
The materials for suprastructures were fabricated from different forms of ceramics (feldspathic porcelain, lithium disilicate, zirconia) and acrylic.
The cases where zirconia frameworks were used had the superstructure crowns made in any form of ceramic. For titanium frameworks, acrylic or ceramic crowns were fabricated. The PEKK framework had the suprastructure done with Polymethylmethacrylate (PMMA) resin crowns [19].
The prostheses were either screw retained, or cement retained or a combination where in, the frameworks were screw retained and the individual crowns were cemented on to the frameworks. Ten of the case reports showed the prostheses to be screw retained [5,7-10,12,13,15,17,18] and two reports were cement retained [11,19]. Al-Thobity A et al., Reshad M et al., Yoon HI et al., reported cases withframeworks that were screw retained and individual crows cemented over them [6,14,16].
Characteristics of prospective cohorts: The study by Pozzi constituted 18 individuals (7 males and 11 females) with severely atrophied ridges. Surgical placement of 36 implants was done in 9 maxillae and 9 mandibles. These were prosthetically rehabilitated with milled titanium bar and a superstructure comprising a cast Co-Cr framework with overlying acrylic denture with locator attachments. The mode of retention used were screw retained prostheses fabricated by Nobel Biocare [20].
Weinsteins’s prospective cohort study that was done on 20 patients (8 males and 12 females) with severely atrophied mandible, had implants placed in the intraforaminal region of mandible in accordance to the “All on Four protocol” and were prosthetically rehabilitated with fixed screw retained acrylic prostheses using the CAD/CAM Procera System [21].
Agliardi EL et al., performed a study on 15 patients (2 males and 13 females) with severely atrophic maxillae. Implants were placed in zygomatic bone and anterior maxilla following the “All on Four Protocol”. Prosthetic rehabilitation was done with CAD/CAM milled titanium frameworks that were screw retained to the implants and the superstructures had acrylic or ceramic crowns cemented onto the frameworks [22].
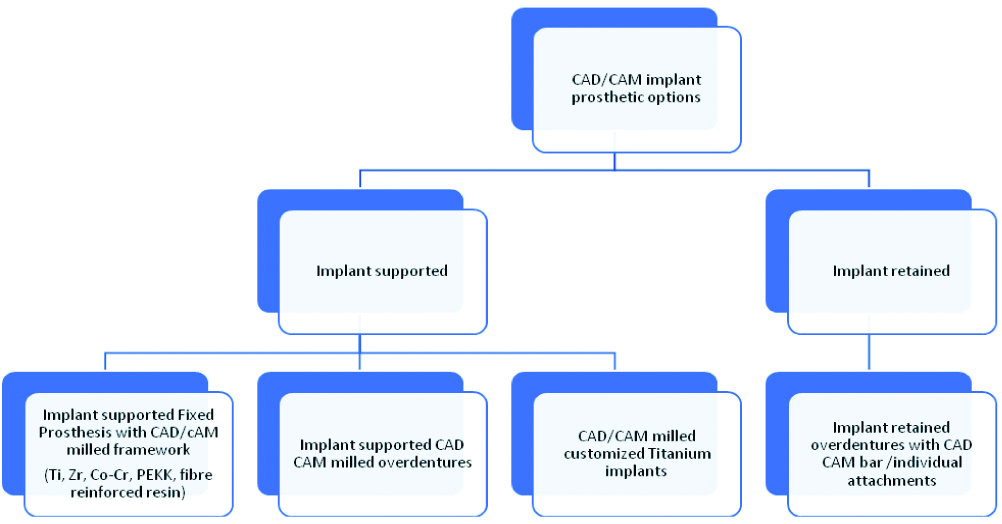
In the prospective cohort study by Seeman, that included 10 patients (2 males and 8 females) with severely atrophied mandible, 4 implants were placed in each patient and were prosthetically rehabilitated with cement retained CAD/CAM milled fiber-reinforced and composite resin-facetted bridge with acrylic teeth, manufactured by TriniaBicon [23]. [Table/Fig-3] summarises the various implant prosthetic options using CAD/CAM technology.
Implant supported/retained CAD/CAM prosthetic options.
Summary of Industrial Reports
The industrial reports discussed various CAD/CAM customised bar and framework designs by 4 manufacturers – NobelProcera (Nobel Biocare, Zurich, Switzerland) [24], CAM StructSURE- Bella Tek Bars (Biomet 3i, Florida, USA) [25], Etkon system (Straumann, Basel, Switzerland) [26] and Atlantis (DentsplyCompartis, ISUS) [27]. [Table/Fig-4] elaborates various implant retained/supported CAD/CAM bar designs for removable and fixed prosthesis by the manufacturers.
CAD/CAM bar designs by manufacturer [24-27].
| Nobel Procera [24] | Biomet 3i (CAM Struc SURE) [25] | STRAUMANN (ETKON system) [26] | ATLANTIS (Dentsply Compartis ISUS) [27] |
|---|
| Removable1. Free Form Milled Bar with Locator attachments2. Dolder Bar with gold riders3. Hader Bar with nylon clips and housings4. Milled Bar with ball attachments5. Round bar6. Mixed bar – milled bar with Dolder extensions7. Paris BarFixed 1. Fixed bar Montreal type without metallic lingual2. Fixed bar Montréal type with metallic lingual3. Wrap around bar4. Hybrid bar5. Procera Implant bridge6. Malo’s bridge | Removable1. Dolder egg shape bar2. Dolder U shape bar3. Hader bar4. Primary Bar5. Combination Hader and Dolder barsFixed1. Hybrid prostheses2. Wrap around bar3. Freeform bar4. Montreal bar | Removable1. Dolder® Bar U-Shape2. Dolder® Bar Egg-Shape 3. Ackermann-Bar® 1.9 mm4. MP-Clip® Bar 1.8 mm5. Milled Bar, available threads for Locator6. round bar 1.8 mm diameterFixed(Cares Screw-Retained Bridges and Bars) | RemovableATLANTIS” BarAtlantis 2 in 1FixedAtlantis Hybrid |
Discussion
This scoping review enumerates various CAD/CAM prosthetic options to rehabilitate compromised ridge with implants. Increased crown height space, changes in anatomic contours and altered maxillomandibular relation affects the prognosis of rehabilitation with removable or fixed prosthesis in case of compromised ridges. Therefore, these patients are the best suited for implant supported or retained prosthesis. CAD/CAM in fabrication of implant prosthesis offers better clinical fit, fewer fabrication steps, faster turn around, and elimination of distortion compared to conventional casting techniques.
CAD/CAM Prosthetic Options
1. Implant retained overdentures with CAD CAM bar attachments: In compromised clinical conditions where an implant supported fixed prosthesis cannot compensate for severe bone and soft tissue loss, implant retained overdenture can satisfy both aesthetic and prosthetic retention needs. Goo CL et al., reported the use of CAD/CAM milled Titanium bar overdenture with cast metal framework to reinforce the strength of prosthesis in knife edged mandibular ridge. It proved advantageous by resisting lateral load and improving stability [12]. In a fibula reconstructed mandible reported by Koch FP et al., CAD/CAM milled Titanium Dolder overdenture bar defined the form and position of fibula. It also acted as an external fixator stabilizing the molded fibula thereby positioning the prosthesis in occlusal harmony with the upper jaw. The drawback posed by this mode of rehabilitation is that, the entire procedure from harvesting fibula flap to insertion of overdenture are performed at the same time resulting in higher chances of morbidity [13].
In patients with severely resorbed ridges, a fixed prosthesis can be challenging due to the undue overlap of the prosthetic flange onto the residual ridge, both horizontally and vertically, making hygiene difficult. Rehabilitation of such conditions with an overdenture supported by a CAD/CAM milled titanium bar evades encroachment on soft tissues and also reduces the denture base extension. In a prospective cohort study by Pozzi, patients with an altered skeletal maxillomandibular relationship and bone resorption were prosthetically rehabilitated with implant retained bar overdentures. The design included a CAD/CAM milled titanium bar with cast cobalt-chromium metal framework and acrylic overdenture. The rigid parallel-walled bars lessened the rotational movements similar to fixed prosthesis, thereby minimising wear of the attachment system and veneering material. One-year review showed 100% prosthetic success and survival rate in both ridges, with good patient acceptability. Though the prosthesis showed many advantages, the study posed the limitation of not having a control group [20].
2. Implant supported CAD/CAM overdenture: In patients where implant supported fixed prosthesis cannot be advocated due to proximity to anatomical landmarks thus impeding the placement of implants in the desired position for a fixed prosthesis or due to problems of aesthetics and speech, attributing to a lack of lip support, this type of prosthesis can be indicated. A case report by Agustín-Panadero R et al., with severely resorbed maxilla and severe Class III ridge relationship was reported. The prosthetic rehabilitation was done with implant supported overdenture with horizontal insertion manufactured using CAD/CAM technology. The prosthesis provided a better fit between anatomic structures compensating for the negative intermaxillary discrepancy. The main factors that warranted the use of horizontal dentures to fixed prosthesis were provision of adequate lip support, compensation for intermaxillary discrepancy and good hygiene [5].
3. Implant supported fixed prosthesis: Removable dentures supported/retained by implants have proven advantageous by enhancing buccal/labial fullness with the presence of prostheses flanges. But in patients with mandibular resection, this type of prosthesis can cause inconvenience due to decreased keratinized mucosa. In such cases, fixed prostheses supported by implants can be effective by providing better comfort, biting efficacy and stability [19].
CAD CAM Milled Framework Designs
a. CAD/CAM milled titanium framework: A prospective study by Weinstein reported rehabilitation of patients with severe atrophy of posterior mandible using CAD/CAM Procera System with screw retained Titanium milled bar and acrylic suprastructure. One year success rate of the prosthesis was 100% and the quality of life assessed satisfactory aesthetics by 66.7%, phonetics 77.8% and mastication 88.9%. This study had a major limitation of a very short follow up period of 1 year. To assess the efficacy, a long term evaluation is mandated [21].
Implant-supported fixed restoration is a reliable mode of treatment for patients with insufficient bone volume in mandible. The application of CAD/CAM has extended the scope for this treatment option. A milled titanium bar retaining individual all-ceramic zirconia crowns, veneered with porcelain and gingival composite, has been advocated as an acceptable prosthetic option in such compromised conditions. Reshad M et al., reported the use of this prosthesis in a patient with a minimal mandibular residual height. A 12-month follow up showed good patient compliance in terms of function and aesthetics. It possessed the advantages of easy repair and retrievability. The prosthetic design comprised of all-ceramic restorations luted onto a rigid metal substructure with a high rigidity (titanium framework), enabled prevention of crack initiation and propagation. The limitations of this prosthesis exhibited were, increased possibilities of fracture of all ceramic restorations, staining at the junction between composite and all ceramic, difficulty in retievability and more time consumption in luting with resin cement [14].
In extremely resorbed ridges where adequate support cannot be rendered by the palate, stability for an upper denture will be a difficult task. Presence of flabby tissues can also aggravate patient inconvenience and hence rehabilitation with an implant-supported prosthesis poses a challenge. In such situations, the prosthesis extends towards the palate, compromising speech and hygiene. The positioning of the prosthetic screw will also be different from the ideal location (cingulum for anterior teeth and the central fossa for posterior dentition). A prospective cohort study by Agliardi EL et al., reported on complete-arch prostheses supported by zygoma implants after a period of 6 years of loading using the All on 4 Hybrid protocol. The patients were prosthetically rehabilitated with (CAD/CAM) Procera titanium prostheses with acrylic or ceramic teeth (Procera Implant Bridge). The prosthesis success rate was 100%. Patient contentment in terms of aesthetics, function and speech was also high. The main limitation of this study was the limited number of patients taken into consideration [22].
In severely deficient maxilla caused by traumatic injury, rehabilitation with a fixed prosthesis using a conventional endosseous implant protocol might result in significant bone grafting. Al Thobity A et al., published a report wherein a patient with severely deficient maxilla caused by a gunshot injury was surgically rehabilitated with zygomatic and pterygomaxillary implants. The prosthetic rehabilitation was done with CAD/CAM milled titanium framework and individually cemented IPS e-max crowns. This provided the patient with a satisfactory aesthetic and functional fixed prosthesis that also eliminated the need of bone grafting. It also enabled the possibility of repair, if an individual crown had to be replaced [6].
A case was reported by Bentz with atrophied ridges and class III ridge relation. The prosthetic design for both the arches comprised of a Computer Numeric Controlled (CNC)-milled titanium framework (NobelProcera Implant Bridge) veneered with thermocure acrylic resin and denture teeth. These frameworks for edentulous arches had better precision, good passive-fit and a stable and predictable reconstruction [8].
Papaspyridakos P illustrated a digital workflow for the rehabilitation of extremely atrophic edentulous mandible with full-arch implant-supported fixed prosthesis that comprised a screw-retained full arch titanium framework with luted individual lithium-disilicate crowns. In addition to limited appointments, it also enhanced patient acceptance and comfort and served as a good alternative in rehabilitation of compromised ridges [10].
Patients with mandibular resection and reconstruction with microvascular fibula free flap are of concern in prosthetic rehabilitation due to insufficient vestibular depth. Often debulking and/or vestibuloplastyis performed to provide a thinner and firm base for the prosthesis. Provision of CAD/CAM partial fixed dental prosthesis has been successful in such situations. Schneider reported a case of resection and reconstruction that was prosthetically rehabilitated with a CAD/CAM Titanium framework and acrylic resin prosthetic teeth. The prosthesis proved effective by decreasing the prognathic appearance and 4 years follow up showed good outcome in terms of function and aesthetics [17]. It was advantageous by providing good retention, material support and adequate access for oral hygiene which are important factors to be considered in compromised ridges.
b. CAD/CAM milled zirconia framework: Zirconia is widely used as a core material for manufacturing frameworks for implant-supported fixed partial dentures owing to their superiority in aesthetics and good flexural strength [9].
Zirconia has the disadvantage of long term degradation, aging, veneer porcelain chipping and stress concentration inside a framework that may induce cracking of the veneer porcelain [28]. To lower the inaccuracies in veneering ceramics, monolithic zirconia restorations or pressing the veneering porcelain to the zirconia framework have been introduced [29].
Cho Y et al., discussed the use of CAD/CAM fabricated lithium disilicate monolithic heat pressed ceramic crowns with holes for abutment screw access bonded onto a zirconia framework, with the framework cemented onto the implants with provisional cement, to restore a severely atrophied edentulous mandible. This prosthetic design reduced the incidence of fracture of the layered porcelain, facilitated removal when desired and easy corrections of occlusal disharmonies. It has shown promising results in aesthetics, strength and structural integrity. But the limitations it possessed were in terms of cost and the risk of failure in the bond between zirconia framework and the veneering gingival porcelain [11].
Papaspyridakos reported the rehabilitation of a patient with severely atrophic mandible, with screw retained CAD/CAM milled zirconia framework veneered with feldspathic porcelain. The prosthesis showed good results in terms of patient comfort, appearance and biocompatibility [9]. Although not many long term clinical studies have been reported on this type of prosthesis with zirconia framework, there are several in-vitro studies showing the stress concentration inside the framework thus, causing fracture of the veneering porcelain, which can pose as a major drawback with this prosthesis.
Zirconia frameworks have shown positive effect on stress reduction in peri implant bone tissue. CAD/CAM in fabrication of zirconia frameworks has increased the accuracy and passiveness of fit. Yoon H-I et al., discussed a case of resected and reconstructed mandible, prosthetically rehabilitated with CAD/CAM fabricated zirconia framework veneered with porcelain. It showed satisfactory aesthetic and functional performance over 1 year [16]. Owing to the short follow-up period, limitations could not be delineated; rather it was stated, good soft and hard tissue management, and adequate material selection could enhance prosthetic success.
c. CAD/CAM milled Cobalt-Chromium (Co-Cr) framework: Implant prosthetic rehabilitation of compromised ridges with screw retained CAD/CAM milled chrome–cobalt framework and veneered porcelain has shown promising results. Sethi A et al., reported a case with severely atrophied mandible [15] and Agustín-Panadero R, rehabilitated a case of epidermolysis bullosa with deficient maxilla [7]. The fabrication of these prostheses using CAD/CAM technology has enabled construction of accurately fitting restorations for screw retention and significantly increasing patients’ quality of life.
d. CAD/CAM milled PEKK framework: Polyetheretherketone (PEKK), a material belonging to the class of thermoplastic polymers, is increasingly used in dentistry owing to its good mechanical and biological properties [30].
Oh KC et al., reported on prosthetic rehabilitation of a hemi-mandibulectomy patient, reconstructed with fibula graft. The prosthetic design consisted of a CAD/CAM fabricated PEKK framework with polymethylmethacrylate (PMMA) crowns cemented onto it. It was luted on the abutments with a resin cement. The prosthesis exhibited satisfactory results without any problems over 12 months [19]. Since long term data for this framework are not available, continuous monitoring is mandated to decipher the efficiency and success of this prosthesis.
e. CAD/CAM milled fiber reinforced resin framework: Fiber-reinforced resin is a material lighter than zirconium or Chromium-Cobalt (Cr-Co) and with mechanical properties comparable to that of zirconia and chromium-cobalt. In a prospective cohort study by Seeman, four short implants were placed in resorbed jaws and were rehabilitated with TRINIA scaffold, a fiber-reinforced resin framework with acrylic denture teeth cemented onto it. This, being metal free proved effective in reducing laboratory procedures. It was efficient in withstanding masticatory load without any fracture or chipping [23]. The drawback of this technique was the difficulty in cleaning the prosthesis and incidental detachment after final cementation. The main limitation of this study was that it was confined to atrophic jaws opposing dentures and not natural dentition.
CAD/CAM milled Customised Titanium Implant
This is a patient specific implant system, reported by Rachmiel A et al., for rehabilitation of a mandible with a large defect involving ramus, body and the angle. This customised titanium implant, contained a crib with pores for better osseointegration of the autogenous bone graft. Dental rehabilitation employed zirconia crowns on multiunit abutments, and placement of screw-retained crowns. One-year follow-up showed good function and appearance [18]. This mode of rehabilitation exhibited accurate occlusion, symmetry of the face and mandible, with proper mandibular movements.
Limitation
The results of the present review must be interpreted with caution because of its limitations. The quality of the included studies varied greatly. The main limitation of the review was that there were no randomised control trials available during the period the articles were included, for quality assessment. The electronic database search showed 42 studies which were excluded after in depth screening for various reasons. The main reasons for exclusion were that the studies did not specify the rehabilitation of compromised ridges, and the technology used for fabrication did not pertain to CAD/CAM. As these studies could not contribute to the review, we may have missed relevant results. Most of the studies had limited follow-up period and did not mention any specific outcome calibration criteria. Most of the case reports also did not mention the disadvantages of the prostheses that were fabricated for rehabilitation of the compromised conditions.
Conclusion
Prosthetic rehabilitation of compromised ridge with implant supported prosthesis using CAD/CAM technology shortens the total rehabilitation/reconstruction time. CAD/CAM fabrication of bars and frameworks has resulted in elimination of distortion, better fit, fewer fabrication steps, and faster turn-around when compared to conventional casting techniques. Implant-supported fixed prosthesis with CAD /CAM milled framework is a reliable treatment option in atrophic ridges offering high level of patient satisfaction in terms of aesthetics, function and phonetics. In clinical conditions where fixed prosthesis cannot compensate the severe bone resorption, soft tissue loss and increased crown height space, implant supported/ retained overdentures with bar attachments satisfy aesthetics, hygiene maintenance and prosthetic retention needs. Although the use of CAD/CAM in dentistry is dated back to 1970s, its employment in fabrication of implant supported prosthesis for compromised ridges is not very old. With more patients being rehabilitated by this technology, this scoping review will enable the clinician in selecting the right prosthesis for compromised ridges.