Burkholderia Infections in Diabetic Patients Emerging as a Challenge for Physicians: A Case Series
Shubhransu Patro1, Sudhansu Sekhar Panda2, Debashish Mishra3, Sonapuram Keerthi4
1 Professor, Department of General Medicine, KIMS, Bhubaneswar, Odisha, India.
2 Professor, Department of General Medicine, KIMS, Bhubaneswar, Odisha, India.
3 Assistant Professor, Department of Orthopaedics, KIMS, Bhubaneswar, Odisha, India.
4 Postgraduate Resident, Department of General Medicine, KIMS, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sonapuram Keerthi, C302, Balaram Anant Complex, Damana, Bhubaneswar, Odisha, India.
E-mail: keerthi.sonapuram505@gmail.com
The genus Burkholderia comprises more than 40 species. Medically important members of this genus are Burkholderia cepacia (B.cepacia), Burkholderia pseudomallei (B.pseudomallei) and Burkholderia mallei (B.mallei). Burkholderia cepacia complex (Bcc) can cause Cepacia syndrome which includes necrotising pneumonia, respiratory failure and bacteremia in Cystic Fibrosis (CF) patients and can be fatal. B.cepacia can be potentially pathogenic in individuals with impaired host defences and can cause pneumonia, bronchiectasis, pyopneumothorax and cavitatory lesions. The clinical manifestations of Melioidosis range from localised infection to overwhelming sepsis and death with Pneumonia being the most common presentation. The most significant risk factor for Melioidosis is diabetes. Musculoskeletal Melioidosis is not common in India even though sporadic cases have been reported mostly involving soft tissues. In the present two cases of Melioidosis in diabetics who presented with septic arthritis treated with surgical debridement followed by antibiotics and two cases of Cepacia syndrome in diabetics whose hospital course was complicated by pneumothorax and Acute Respiratory Distress Syndrome (ARDS). These reports raise the concern regarding the potential severity of Burkholderia infections and prompts early diagnosis by physicians to prevent morbidity and mortality.
Cepacia syndrome, Cystic fibrosis, Melioidosis, Pyopneumothorax
Case Report
Case 1
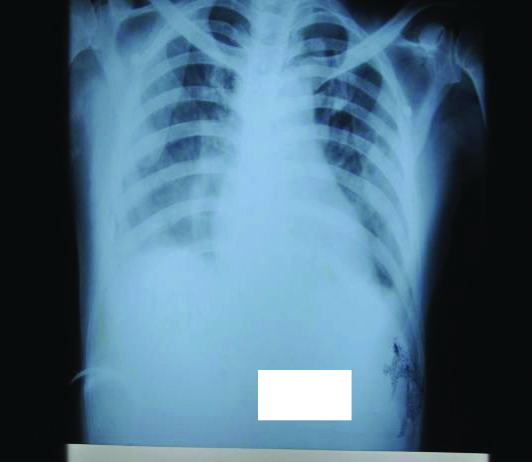
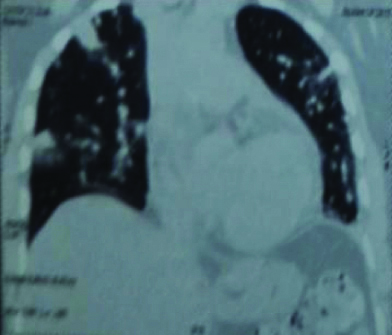
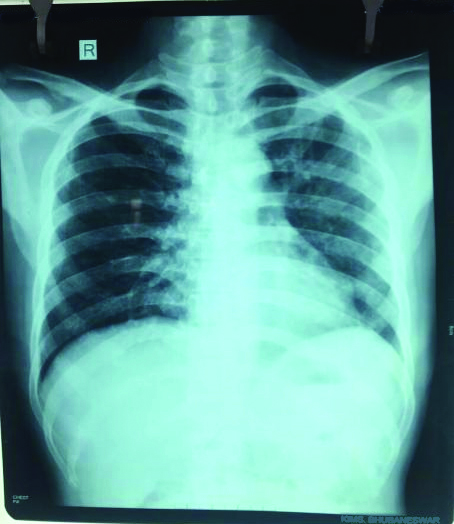
A 52-year-old diabetic male patient came to Medicine Out-Patient Department (OPD) with chief complaints of fever since last 45 days and swelling of left knee joint [Table/Fig-1] since last three days. Before admission to the hospital, empirical Antitubercular Therapy (ATT) was started outside after the Chest X-Ray (CXR) showed features of bilateral bronchopneumonia [Table/Fig-2] and Computerised Tomography (CT) scan of thorax showed nodules [Table/Fig-3].
Knee joint before treatment.

CT Thorax with pulmonary nodules.
Patient was started on amoxicillin-clavulanic acid along with regular insulin and ATT was discontinued. Samples of urine, blood, sputum and pus from aspirated knee joint were sent for culture for identification of causative organism. As the condition of the patient deteriorated (dyspnoea and fall in oxygen saturation); he was immediately shifted to Intensive Care Unit (ICU) and antibiotic was escalated to Piperacillin-Tazobactam suspecting septicaemia. In the meantime, arthrotomy of the knee joint was done [Table/Fig-4]. B.pseudomallei was isolated from blood, sputum and aspirated pus from involved joint using automated methods (BacT Alert and VITEK-2). Based on sensitivity pattern, the suspicion was almost accurate as the patient was from a locality where rice farming is mostly done, the area faces heavy rainfall as well as he was diabetic. After being confirmed as case of Melioidosis immediate treatment with systemic ceftazidime and imipenem was started. Bronchopneumonia resolved [Table/Fig-5]. After two weeks of parenteral antibiotic therapy, patient was switched over to oral co-trimoxazole for twelve more weeks with regular follow-up.
Knee joint after treatment.

Case 2
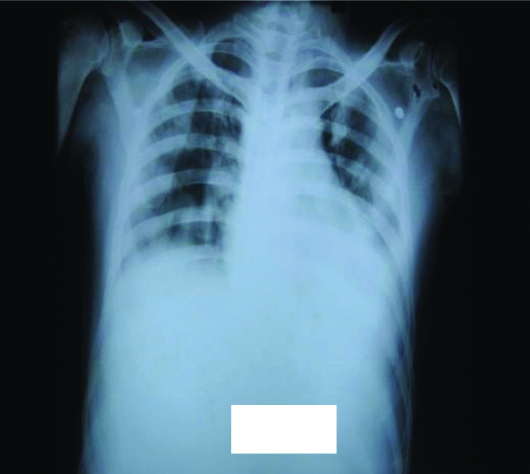
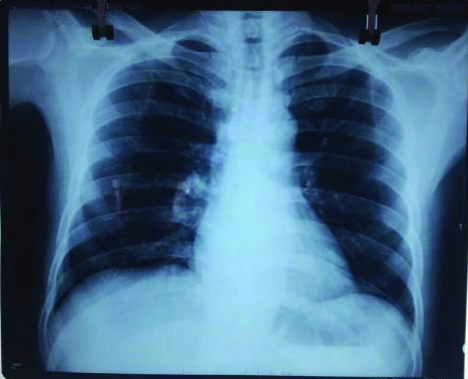
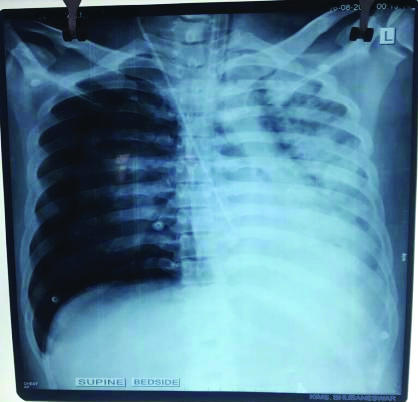
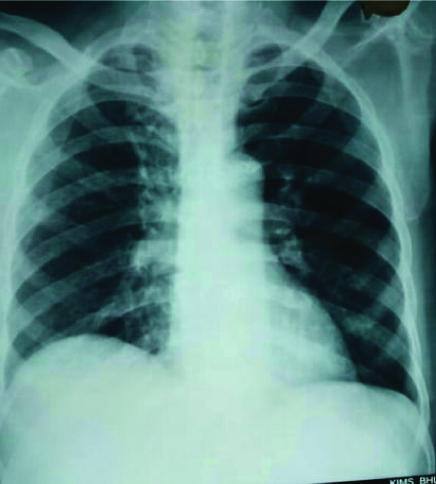
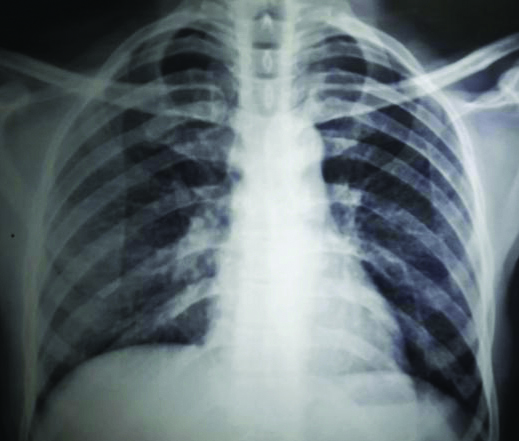
A 41-year-old male patient presented in Medicine OPD with history of fever for seven days duration associated with headache and pain in left groin. All routine investigations were done. Chest X-Ray Postero-Anterior View (CXR-PA) was normal [Table/Fig-6]. He was newly diagnosed with diabetes. Later abruptly, patient developed shortness of breath and sudden onset of hypotension following which patient became tachypnoeic and saturation in pulse oximetry showed 79% at room air. Hence the patient was shifted to ICU. Arterial Blood Gas (ABG) analysis showed severe hypoxia and patient was intubated and was kept on vasopressor support. CXR revealed pneumothorax on right side and consolidation on left side [Table/Fig-7]. Procalcitonin was 33.3 ng/mL which indicated severe septicaemia. Repeated blood cultures revealed B.cepacia using automated methods (BacT Alert and VITEK-2). According to sensitivity pattern, meropenem was started. Blood sugar was controlled. Patient was extubated after ARDS improved [Table/Fig-8]. Finally patient recovered from the septic shock and ARDS due to Cepacia syndrome and was discharged after 20 days of hospitalisation with oral cotrimoxazole.
Normal CXR-PA at admission.
CXR showing Pneumothorax, consolidation.
CXR showing resolution at discharge.
Case 3
A 68-year-old diabetic male patient presented to Orthopaedics OPD with chief complaints of fever and swelling of left knee joint for 40 days duration [Table/Fig-9]. He was treated as a case of Tubercular osteomyelitis and ATT was started prior to hospitalisation to our hospital. On examination there was diffuse swelling over left knee joint. Patient was diagnosed as a case of chronic osteomyelitis and along with all routine investigations; pus was aspirated from knee joint and sent for culture which showed B.pseudomallei by using automated methods (BacT Alert and VITEK-2). ATT was stopped as there was no response. Surgical debridement was done [Table/Fig-10]. CXR-PA is normal [Table/Fig-11]. Subsequent blood and pus cultures showed B.cepacia by isolation through automated methods (BacT Alert and VITEK-2). Hence, patient was diagnosed with Burkholderia sepsis and was started on intravenous ceftazidime according to sensitivity report for two weeks. Gradually patient recovered symptomatically and was discharged with oral doxycycline with regular follow-up.
Knee joint before treatment.

Knee joint after treatment.

Case 4
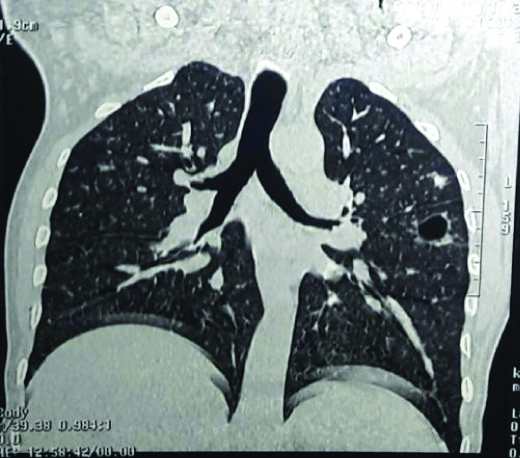
A 45-year-old diabetic male patient was admitted to medicine OPD with chief complaints of fever and pain in the right thigh for 15 days duration. Fever was persistent and on chest examination bilateral rhonchi were present. Blood picture showed neutrophilic leucocytosis and CXR-PA showed features of bronchitis [Table/Fig-12]. Patient was started on piperacillin-tazobactum. X-ray of right hip joint showed no abnormality hence Magnetic Resonance Imaging (MRI) of right thigh was done which showed osteomyelitis with abscess. High-Resolution Computerised Tomography (HRCT) scan of Thorax showed chronic infective pathology with a cavitatory lesion [Table/Fig-13]. Blood culture was done using automated methods (BacT Alert and VITEK-2) and B.cepacia was isolated. Patient was diagnosed as case of Cepacia syndrome and according to sensitivity report, patient was started on intravenous meropenem. Patient responded to treatment and became afebrile. Patient was discharged with oral cotrimoxazole and advised for regular follow-up.
HRCT Thorax with cavitatory lesion.
Discussion
Burkholderia genus comprises of gram-negative bacteria that have in common an inability to ferment lactose. B.cepacia is oppurtunistic bacillus that inhabits moist environments in rhizosphere [1-5]. It possesses multiple virulence factors and colonising factors that are capable of binding to lung mucus which explains the predilection of B.cepacia for lungs in CF [6]. B.cepacia secretes elastase and like Pseudomonas aeuroginosa, it possesses injectable toxin secretion system. Besides infecting the lungs in CF, B.cepacia appears as an airway coloniser during broad spectrum antibiotic therapy and is a cause of Ventilator Associated Pneumonia (VAP), catheter associated infections and wound infections. The organism is known to colonise the lungs of CF patients occasionally causing chronic pulmonary infection [1-5,7]. B.cepacia can be isolated in blood cultures and is intrinsically resistant to many antibiotics [2,4,5,7]. Carbapenems, ceftazidime, piperacillin-tazobactum and cotrimoxazole are effective agents against Bcc [2,5]. Bcc infection causes Cepacia syndrome which is fatal combination of necrotising pneumonia, rapid respiratory failure and septicaemia [8]. Cases of severe Bcc lung infection have been reported and include pneumonia, bronchiectasis, pyopneumothorax and cavitatory lesions [8]. B. pseudomallei, a soil saprophyte is the cause of Melioidosis with clinical manifestations ranging from localized infection to overwhelming sepsis and death. Melioidosis is endemic in Southeast Asia and Northern Australia, where it accounts for 20% of all community acquired septicaemias and causes death in 40% of treated patients in Thailand [9,10]. Even among people who are exposed to soil and surface waters in endemic areas, active infection mainly occurs in people who have underlying predisposing conditions like diabetes mellitus, renal disease, alcoholism, cirrhosis, chronic lung disease, thalassemia, malnutrition or immunosuppression due to disease or drug therapy [10]. B. pseudomallei can cause Melioidosis in diabetics due to functional neutrophil defects which are important in pathogenesis. B. pseudomallei is mostly sensitive to ceftazidime, imipenem (intensive phase), cotrimoxazole, chloramphenicol doxycycline and amoxycillin-clavulanic acid (maintenance phase) [9,10]. Documented reports of Melioidosis from India have been few and sporadic. The majority of reports of Melioidosis from India have been documented from CMC, Vellore [11]. Sporadic cases have also been reported from Maharashtra, Kerala, Karnataka and Pondicherry [12-14]. Melioidosis patients are often more severely ill after heavy monsoonal rainfall which results in a shift towards inhalation as the mode of infection with B.pseudomallei, which leads to more severe illness [15].
Conclusion
Bcc is a hospital acquired infection and potentially pathogenic in individuals with impaired host defences. B.cepacia may cause sudden onset of ARDS with requirement of ventilator support. High index of suspicion in all cases of septicaemia with conditions such as diabetes will be useful in detecting many more cases of Burkholderia infections like Melioidosis. These infections are difficult to treat and patients need long-term antibiotic therapy for complete cure. Recurrences are common even after strictly controlled treatment. Hence prompt treatment is required and the underlying causes like diabetes to be corrected. Physicians need to be careful as Burkholderia infections are dreadful.
[1]. Lynch JP, Burkholderia cepacia complex: impact on the cystic fibrosis lung lesionSemin Respir Crit Care Med 2009 30(5):596-610.10.1055/s-0029-123891819760547 [Google Scholar] [CrossRef] [PubMed]
[2]. Dizbay M, Tunccan OG, Sezer BE, Aktas F, Arman D, Nosocomial Burkholderia cepacia infections in a Turkish university hospital: a five-year surveillanceJ Infect Dev Ctries 2009 3(4):273-77.10.3855/jidc.12419759490 [Google Scholar] [CrossRef] [PubMed]
[3]. Coutinho HD, Burkholderia cepacia complex: virulence characteristics, importance and relationship with cystic fibrosisIndian J Med Sci 2007 61(7):422-29.10.4103/0019-5359.3319417611350 [Google Scholar] [CrossRef] [PubMed]
[4]. McClean S, Callaghan M, Burkholderia cepacia complex: epithelial cell-pathogen confrontations and potential for therapeutic interventionJ Med Microbiol 2009 58(1):110.1099/jmm.0.47788-019074648 [Google Scholar] [CrossRef] [PubMed]
[5]. Araque-Calderon Y, Miranda-Contreras L, Rodriguez-Lemoine V, Palacios-Pru EL, Antibiotic resistance patterns and SDS-PAGE protein profiles of Burkholderia cepacia complex isolates from nosocomial and environmental sources in VenezuelaMed Sci Monit 2008 14:49-55. [Google Scholar]
[6]. Leitão JH, Sousa SA, Ferreira AS, Ramos CG, Silva IN, Moreira LM, Pathogenicity, virulence factors, and strategies to fight against Burkholderia cepacia complex pathogens and related speciesAppl Microbiol Biotechnol 2010 87(1):31-40.10.1007/s00253-010-2528-020390415 [Google Scholar] [CrossRef] [PubMed]
[7]. Leitão JH, Sousa SA, Cunha MV, Salgado MJ, Melo-Cristino J, Barreto MC, Variation of the antimicrobial susceptibility profiles of Burkholderia cepacia complex clonal isolates obtained from chronically infected cystic fibrosis patients: a five-year survey in the major Portuguese treatment centerEur J Clin Microbiol Infect Dis 2008 27(11):1101-11.10.1007/s10096-008-0552-018600352 [Google Scholar] [CrossRef] [PubMed]
[8]. Hauser N, Orsini J, Cepacia syndrome in a non-cystic fibrosis patientCase Reports in Infectious Diseases 2015 2015:53762710.1155/2015/53762726357579 [Google Scholar] [CrossRef] [PubMed]
[9]. White NJ, MelioidosisLancet 2003 361:1715-22.10.1016/S0140-6736(03)13374-0 [Google Scholar] [CrossRef]
[10]. Cheng AC, Currie BJ, Melioidosis: Epidemiology, pathophysiology and managementClin Microbiol Rev 2005 18:383-416.10.1128/CMR.18.2.383-416.200515831829 [Google Scholar] [CrossRef] [PubMed]
[11]. Jesudason MV, Anbarasu A, John TJ, Septicaemic melioidosis in a tertiary care hospital in south IndiaIndian J Med Res 2003 117:119-21. [Google Scholar]
[12]. Kanungo R, Padhan P, Bhattacharya S, Srimannarayana J, Jayanthi S, Swaminathan RP, Melioidosis: A report from Pondicherry, South IndiaJ Assoc Physicians India 2002 50:1438-39. [Google Scholar]
[13]. Rao PS, Dhawan R, Shivananda PG, Burkholderia pseudomallei infectionsTrop Doct 2002 32:174-75.10.1177/00494755020320032112139165 [Google Scholar] [CrossRef] [PubMed]
[14]. Vidyalakshmi K, Shrikala B, Bharathi B, Suchitra U, Melioidosis: an underdiagnosed entity in Western coastal India: A clinico-microbiological analysisIndian J Med Microbiol 2007 25:245-48.10.4103/0255-0857.3476717901643 [Google Scholar] [CrossRef] [PubMed]
[15]. Currie BJ, Jacups SP, Intensity of Rainfall and Severity of MelioidosisAustralia: Emerging Infectious Diseases 2003 9(12)[www.cdc.gov/eid]10.3201/eid0912.02075014720392 [Google Scholar] [CrossRef] [PubMed]