Anaplastic Carcinoma Occurring in a Longstanding Multinodular Goitre Diagnosed by FNAC: A Rare Case
Devi Beena1
1 Assistant Professor, Department of Pathology, Azeezia Institute of Medical Science and Research, Kollam, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devi Beena, Azeezia Institute of Medical Science and Research, Meeyannoor, Kollam, Kerala, India.
E-mail: devibeena1987@gmail.com
Anaplastic Thyroid Carcinoma (ATC) remains one of the most virulent of all cancers in humans with a survival rate of only 1%. The widespread use of Fine Needle Aspiration Cytology (FNAC) has significantly changed the approach to thyroid nodules and has made it possible to identify such aggressive thyroid neoplasm from aspirated cellular material. ATC can arise from pre-existing well-differentiated thyroid carcinoma. This case is presented due to the rarity of anaplastic carcinoma occurring in Multi-Nodular Goiter (MNG) in an early age group which was diagnosed by FNAC.
Cytology, Neoplasm, Thyroid
Case Report
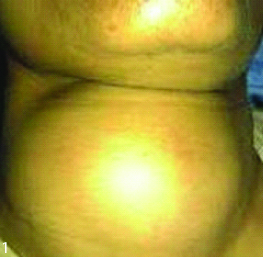
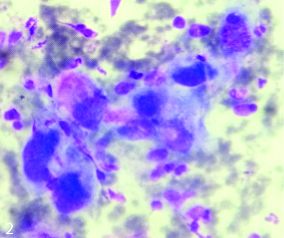
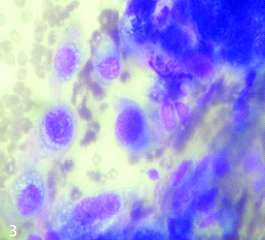
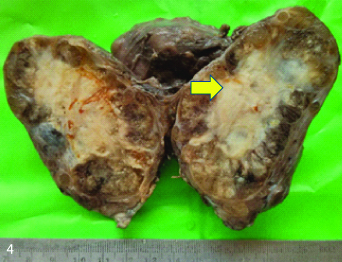
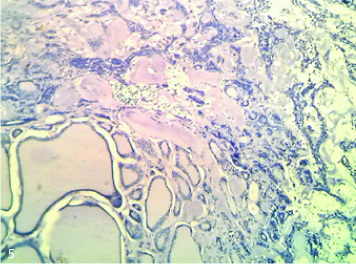
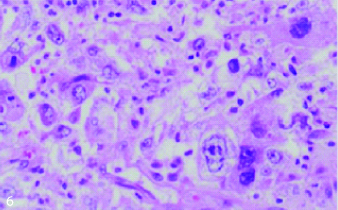
A 45-year-old female presented with a large midline swelling in front of the neck for past 20 years, with complaint of mild dysphagia and sudden increase in size. There was no history of change in voice and breathlessness. She had been diagnosed with multi-nodular goiter at an outside center. Local examination showed diffusely enlarged thyroid measures 5×4 cm [Table/Fig-1] which was firm to hard in consistency, mobile, irregular margin with smooth surface. No palpable cervical lymph nodes were noted. Laboratory investigations revealed that the patient was euthyroid; TSH levels were 4 mU/L. Ultrasound thyroid showed enlargement of both the lobes with multiple hypoechoic lesions and diagnosed as Multi-nodular goitre with hypoechoic lesions. CT scan and thyroid scintigraphy had not been done. Provisional diagnosis of Multinodular goitre was made to rule out thyroid neoplasm. Fine Needle Aspiration Cytology was done from multiple sites which showed scant cellularity comprising of highly pleomorphic cells arranged on singles and clusters. The atypical cells have scanty to moderate cytoplasm [Table/Fig-2], enlarged nucleus showing pleomorphism with coarse chromatin [Table/Fig-3] along with giant cells. Focal areas showed feature of colloid nodule. The cytological diagnosis was given as anaplastic carcinoma of thyroid in a background of nodular goitre. Total thyroidectomy was done and showed a growth of 5×3 cm on cut surface [Table/Fig-4]. Histopathological examination revealed pleomorphic cells with multinucleated giant cells. Scattered mitotic figures were also seen. Thus, the diagnosis of anaplastic carcinoma with multinodular goitre was confirmed [Table/Fig-5,6].
Diffusely enlarged thyroid measures 5×4 cm.
Atypical cells have scanty to moderate cytoplasm (40X).
Enlarged nucleus showing pleomorphism with coarse chromatin (40X).
A pale white growth of 5×3 cm.
Anaplastic carcinoma with multinodular goitre (10X).
Pleomorphic cells with occasional giant cells (40X).
Discussion
ATC is a highly malignant neoplasm that generally pursues a rapidly fatal course [1]. ATC usually presents in 60s and 70s and has female preponderance [2]. The pathogenesis of ATC is not completely understood. Several studies have shown that some ATC’s may be derived from B-type Raf Kinase (BRAF)-mutated papillary thyroid cancer, targeted expression of BRAF in thyroid cells of transgenic mice results in papillary thyroid cancers that undergo differentiation [3]. The origin of ATC in our patient is unclear. Aetiological factors including iodine deficiency, radiation exposure, pre-existing thyroid disease, longstanding goitre is a well known risk factor for ATC [2]. Our patient had history of goitre since 20 years. The patient usually comes with mass which is rapidly growing along with an extra thyroid extension which causes hoarseness, dysphagia and dyspnoea. Diagnosis can be made with the help of cytology, histology, imaging and Immunohistochemistry (IHC) study. The FNAC is reported to be 90% accurate in diagnosing ATC [4]. According to Sharma C, who studied the accuracy of FNAC in detecting thyroid carcinomas in 724 cases, stated that the accuracy of FNAC was 97% [5]. A study done by Wagan PA et al., stated that incidence of malignancy in non-toxic multinodular goitre is around 10.58% and was predominantly papillary carcinoma (7%), however the anaplastic carcinoma is still rare [6]. According to Marcelino M et al., hyperthyroidism is described in some cases of ATC, the concomitant existence of non-toxic multinodular goitre and ATC has not been documented in literature [7]. Our patient had a diffuse swelling which on first aspirate showed frank colloid material. In view of Ultrasonography (USG) report, multiple aspirates were taken from multiple sites which helped in arriving the accurate diagnosis. The presence of osteoclastic giant cells does not have impact on the aggressive nature of this tumour and the prognosis remains the same. The point of importance here is to consider the following differential diagnoses, especially if giant cells are in abundance. The list includes subacute or granulomatous thyroiditis and papillary carcinoma with giant cells. The presence of a dirty background and inflammatory cells can be observed in both granulomatous thyroiditis and anaplastic carcinoma. The giant cells are usually very large in subacute thryroiditis. In the presence of rapidly growing and obstructing goitre, and advanced age, it is essential to consider malignancy and immediately confirm the diagnosis so appropriate therapy may be instituted [5]. Recently, a combination of irradiation and chemotherapy has shown encouraging preliminary result.
Conclusion
Occurrence of thyroid carcinoma in multi-nodular goitre is almost negligible. But if it occurs, tends to be aggressive and potentially fatal. The indexed case shares the relevance of multiple site aspiration in cases of diffusely enlarged thyroid swelling in diagnosing malignant tumours arising in a MNG. It is important to diagnose ATC early and differentiating them.
Informed consent: Informed consent was obtained from the patient.
[1]. Alwani M, Rathod GB, Diagnosis of anaplastic thyroid carcinoma on fine needle aspiration cytology- A rare case reportIAIM 2015 2(3):183-87. [Google Scholar]
[2]. Nagare MR, Joshi SR, Karwande AV, Pathak SS, Tekwani DT, Jaison J, Anaplastic thyroid carcinoma: a rare caseAnnals of applied Bio-Sciences 2015 211(2):6-9. [Google Scholar]
[3]. Quiros RM, Ding HG, Gattuso P, Prinz RA, Xu X, Evidence that one subset of anaplastic thyroid carcinomas are derived from papillary carcinomas due to BRAF and p53 mutationsCancer 2005 103:2261-68.10.1002/cncr.2107315880523 [Google Scholar] [CrossRef] [PubMed]
[4]. Negro R, Valcavi R, Toulis KA, Incidental thyroid cancer in toxic and nontoxic goiter: Is TSH associated with malignancy rate? Results of a meta-analysisEndocrPract 2013 19:212-18.10.4158/EP12234.OR23186976 [Google Scholar] [CrossRef] [PubMed]
[5]. Sharma C, Diagnostic accuracy of fine needle aspiration cytology of thyroid and evaluation of discordant casesJ Egypt NatlCanc Inst 2015 27(3):147-53.10.1016/j.jnci.2015.06.00126185872 [Google Scholar] [CrossRef] [PubMed]
[6]. Adorable-Wagan P, Martinez A, Chua-Agcaoili M, Alcazaren EAS, A case of toxic multi-nodular goiter with anaplastic carcinomaJournal of the ASEAN Federation of endocrine societies 2012 27(1)10.15605/jafes.027.01.19 [Google Scholar] [CrossRef]
[7]. Marcelino M, Marques P, Lopes L, Leite V, Castro JJ, Anaplastic carcinoma and Toxic multinodular goiter: An unusual presentationEur Thyroid J 2014 3:278-82.10.1159/00036789325759806 [Google Scholar] [CrossRef] [PubMed]