Nephrolithiasis is a common health problem that affects 1 out of 10 individuals during their lifetime with an increasing rate of detection in recent decades [1]. In the United States, the lifetime risk of renal stone formation is approximately 12% in males and 5% in females with recurrence rate up to 50% over 5-10 years if left untreated [2]. The epidemiology of nephrolithiasis is related to diet, dehydration, metabolic syndrome (obesity, hypertension and diabetes mellitus), cardiovascular diseases and chronic kidney diseases [3].
Medical imaging plays a substantial role in diagnosis, pre-treatment planning and follow-up of nephrolithiasis. Many imaging methods are useful for diagnosis of nephrolithiasis, including conventional radiography of the kidney, ureter and bladder, intravenous urography, ultrasonography, computed tomography and magnetic resonance imaging. Each technique has its uses and limitations [4]. In the present study, authors used ultrasonography, that is widely available and safe even for children and pregnant women. The European Association of Urology (EAU) recommends ultrasonography as the first imaging method for kidney stones [5]. The detection rate of renal stones by ultrasonography increases with increased stone size [6]. Ultrasonography has 78.9% sensitivity and 83.7% specificity for detection of nephrolith [7]. Concerning size determination of renal stones, stone-specific-algorithm (S-mode) ultrasonography has similar accuracy to CT, with an approximately 1-mm bias from CT-determined size [8]. Because the stone shadow does not vary according to stone depth, measuring the width of the stone shadow is more accurate than measuring the stone itself on ultrasonography images, with only an approximately 1 mm sizing error [9]. There is a significant association between the sensitivity of ultrasonography for detection of renal stones and size of the stone. Nephrolithiasis is the most common discovered cause of hydronephrosis [10]. Both location and size of nephrolithiasis are essential factors for planning clinical management. Due to lack of previous studies covering this topic, this study was designed to clarify the relationship between location and size of nephrolith inside the pelvicalyceal system by comparing the size of nephrolith in different areas inside the kidney. This study has a highly significant value for urologists in selecting the most suitable surgical procedure according to the location and size of nephrolith.
Materials and Methods
Patients: This study was a retrospective study of ultrasound reports of 284 patients who underwent renal imaging by ultrasonography and were diagnosed with nephrolithiasis. All patients were examined from January 2016 to October 2017 in Amran Hospital in Yemen. Ultrasonography examinations of all patients were performed by a specialist with 10 years’ experience in general ultrasound imaging. Data were collected from the preserve reports in the ultrasound unit. Data included the laterality of stones, location of stones in the kidney and stone size. In cases with multiple stones, only the largest stone included in this analysis; Exclusion criteria were the lack of a renal stone diagnosis and the lack of information on the size of stones. Nephrolith was classified according to location in the kidney as follows; Lower calyx, middle calyx, upper calyx, renal pelvis, and PUJ. Size of nephrolithiasis was classified into three categories: 2-10 mm, 11-20 mm and 21-30 mm stones.
Procedure: A Medison, Sono ex-model six colour Doppler machine used for the examinations. A 3.5 MHz curved transducer was used. Patients were scanned by the same highly experienced radiologist following the protocol of ultrasound imaging of the kidneys [11].
Ethics: Institutional Ethical Approval was taken. Patients confidentiality was protected during data collection.
Statistical Analysis
The collected data were analysed using the “Statistical Package for Social Sciences (SPSS), version 16.0”. Statistical analyses including analysis of variance (ANOVA) were performed. Results were reported as frequencies and percentages in categorical data and as means and standard deviations in continuous data.
Results
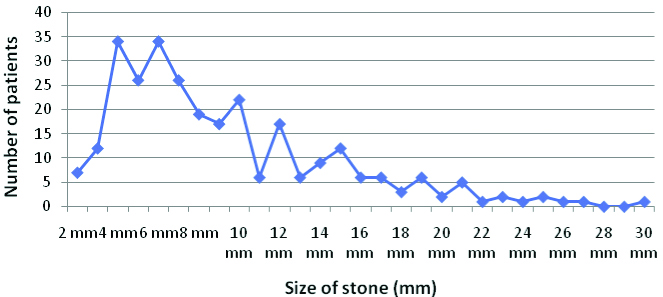
Among 284 patients; 270 (95.1%) were adults, and 194 (68.3%) were males. A total of 284 stone were analysed. Stones were present in the right kidney in 148 (52.1%) and in the left kidney in 136 (47.9%). The majority of stones were 4 mm and 6 mm (12% each), followed by 5 mm and 7 mm (9% each) [Table/Fig-1].
Small size renal stones were predominant. There was a double peaking of stone size at 4 mm and 6 mm.
Small stones predominantly located in the middle, upper and lower calyces. Large stones predominantly located in the PUJ, and renal pelvis [Table/Fig-2]. Most stones were located in the middle and lower calyces (35.9% and 32% respectively).
Relationship between size and intra-renal site of nephrolith. The table revealed a strong relationship between size and site of the stones inside the kidney (p<0.001); Small size stones predominantly located in the middle, upper and lower calyces; Increasing size of stones predominate them to be located in the PUJ and renal pelvis; PUJ: pelviureteric junction
| Size of stones | Site of the largest stone | Total number |
|---|
| Lower calyx | Middle calyx | Upper calyx | Pelvis | PUJ |
|---|
| 02-10 mm | 68 | 85 | 40 | 2 | 2 | 197 (69.3%) |
| 11-20 mm | 22 | 17 | 16 | 8 | 10 | 73 (25.7%) |
| 21-30 mm | 1 | 0 | 0 | 6 | 7 | 14 (5%) |
| Total | 91 (32%) | 102 (35.9%) | 56 (19.7%) | 16 (5.6%) | 19 (6.7%) | 284 (100%) |
There was considerable variation in the size of stones inside the pelviureteric junction and inside the renal pelvis but the variation decreased inside the renal calyces. The least variation in stone size was in the middle calyx (SD=3.76025) [Table/Fig-3].
Mean size of the largest stone according to location inside the kidney.
| Site of the largest stone | Number of stones | Mean | SD |
|---|
| Lower calyx | 91 | 7.9231 | 4.00342 |
| Middle calyx | 102 | 7.3824 | 3.76025 |
| Upper calyx | 56 | 9.2321 | 4.36928 |
| Renal pelvis | 16 | 18.5625 | 5.44021 |
| PUJ | 19 | 17.3158 | 6.41225 |
| Total | 284 | 9.2148 | 5.39726 |
Analysis of variance shows a significant difference between the size of the stones at different sites (p=0.001); There was considerable variation in the size of stones in the renal pelvis and in the pelvi-ureteric junction but the variation decreased in the renal calyces; SD, Standard deviation; PUJ: Pelviureteric junction
In post-hoc analysis; There was a true relationship between stone location and size (p<0.001) in the kidney. Stones in the upper calyx were significantly smaller in size than stones in the renal pelvis (p<0.001) and PUJ (p<0.001). Stones in the middle calyx were significantly smaller in size than stones in the pelvis (p<0.001) and the PUJ (p<0.001). Stones in the lower calyx were significantly smaller in size than those in the pelvis (p<0.001) and PUJ (p<0.001). No significant difference in size was found between stones in the PUJ and renal pelvis (p=1.00) [Table/Fig-4].
Post-hoc analysis of the relationship between size and location of stones inside the kidney.
| (I) Largest | (J) Largest | Mean Difference (I-J) | p-value | 95% confidence interval |
|---|
| Lower calyx | Middle calyx | 0.54072 | 1.000 | -1.2045 - 2.2859 |
| Upper calyx | -1.30907- | 0.726 | -3.3647 - 0.7465 |
| Pelvis | -10.63942* | <0.001 | -13.9204 - -7.3584 |
| PUJ | -9.39271* | <0.001 | -12.4455 - -6.3400 |
| Middle calyx | Lower calyx | -0.54072- | 1.000 | -2.2859 - 1.2045 |
| Upper calyx | -1.84979- | 0.098 | -3.8627 - 0.1631 |
| Pelvis | -11.18015* | <0.001 | -14.4346 - -7.9257 |
| PUJ | -9.93344* | <0.001 | -12.9576 - -6.9093 |
| Upper calyx | Lower calyx | 1.30907 | 0.726 | -0.7465 - 3.3647 |
| Middle calyx | 1.84979 | 0.098 | -0.1631 - 3.8627 |
| Pelvis | -9.33036* | <0.001 | -12.7612 - -5.8995 |
| PUJ | -8.08365* | <0.001 | -11.2970 - -4.8703 |
| Renal pelvis | Lower calyx | 10.63942* | <0.001 | 7.3584 - 13.9204 |
| Middle calyx | 11.18015* | <0.001 | 7.9257 - 14.4346 |
| Upper calyx | 9.33036* | <0.001 | 5.8995 - 12.7612 |
| PUJ | 1.24671 | 1.000 | -2.8600 - 5.3534 |
| PUJ | Lower calyx | 9.39271* | <0.001 | 6.3400 - 12.4455 |
| Middle calyx | 9.93344* | <0.001 | 6.9093 - 12.9576 |
| Upper calyx | 8.08365* | <0.001 | 4.8703 - 11.2970 |
| Pelvis | -1.24671- | 1.000 | -5.3534 - 2.8600 |
Stones in the upper calyces are significantly less in size compared to stones in the renal pelvis (p<0.001) and in PUJ (p<0.001). Stones in the middle calyces are significantly less in size compared to stones in the pelvis (p<0.001) and in PUJ (p<0.001). Stone in the lower calyces are significantly less in size compared to stones in the pelvis (p<0.001) and in PUJ (p<0.001);
No significant difference in size of stones in the renal pelvis and PUJ
No significant relationship was found between the size of the largest stone and the number of stones (p=0.914).
Discussion
Nephrolithiasis is a widespread health problem that can be present at any location in the pelvicalyceal system of the kidney. The present results demonstrate a significant relationship between the size and location of nephrolith in the kidneys. These two factors are essential in selection of treatment modalities and success of extracorporeal shock wave lithotripsy as reported by Tarawneh E et al., [12].
In this study, authors found a statistically significant difference in sex distribution of patients with renal stones (68.3% males vs. 31.7% females). This result is similar to the results of Amir A et al., who reported that nephrolithiasis was more common in male patients (79%) [13]. This predominance is explained by Chand RB et al., who reported that the larger body muscle mass of males cause increase excretion of calcium and waste products [14].
The stones were in the middle calyx in 35.9%, lower calyx in 32%, upper calyx in 19.7%, renal pelvis in 5.6% and PUJ in 6.7% of patients. These results are not compatible with those of the study by El-Assmy A et al., who found that nephrolith was located in the renal pelvis in 42.1% of children, and in the middle, lower and upper calyces in 19.3%, 17.5% and 7% respectively [15].
The largest size stones were predominantly located in the PUJ and the renal pelvis. These results are similar to those of a previous study by Xue W et al., who reported that 73% of large (>20 mm) stones were located in the renal pelvis [16]. The present results are also similar to the findings of Palmero JL et al., who reported that renal stones >20 mm were found in the renal pelvis in 41.5% of cases and in the lower calyx in 36.8% [17]. This result is explained by Randall’s theory of stone formation in the renal pelvis and papillary ducts [18].
The mean sizes of stones in the upper, lower and middle calyces were 9.23, 7.92 and 7.38 mm respectively. The results are consistent with those from a previous study by Khalil MM, who reported that the mean size of stones in the upper, lower and middle pole were 7.5, 6.89 and 5.68 mm respectively [19].
Regarding the number of stones per patients, 50.7% of the patients had a single stone, 29.2% had two stones, 11.6% had three stones, 5.3% had four stones, 2.8% had five stones, and 0.4% had seven stones. The results are consistent with the results of the study by Najeeb Q et al., who reported that 46% of patients had a single stone, 44% had two stones, and 10% had three stones [20].
This study data will aid researchers investigating the effect of nephrolith location on stone size. Furthermore, a new theory concerning the effect of gravity on the location of nephrolith was proposed and is an avenue for further exploration in future studies.
Limitation
This study is limited in that the assessment of location and size of renal calculi was performed using ultrasonography, even though this technique does not provide completely accurate measurement for the size of nephrolith. CT, which could be used for more accurate calculation of nephrolith size, was not available.
Conclusion
In conclusion, there was a significant relationship between the location and size of nephrolith in the kidney. Stones located in the renal pelvis and in the PUJ tend to be larger than stones in the calyces. This can be beneficial for urologists when selecting the method of surgical intervention.
Analysis of variance shows a significant difference between the size of the stones at different sites (p=0.001); There was considerable variation in the size of stones in the renal pelvis and in the pelvi-ureteric junction but the variation decreased in the renal calyces; SD, Standard deviation; PUJ: Pelviureteric junction
Stones in the upper calyces are significantly less in size compared to stones in the renal pelvis (p<0.001) and in PUJ (p<0.001). Stones in the middle calyces are significantly less in size compared to stones in the pelvis (p<0.001) and in PUJ (p<0.001). Stone in the lower calyces are significantly less in size compared to stones in the pelvis (p<0.001) and in PUJ (p<0.001);
No significant difference in size of stones in the renal pelvis and PUJ