Evaluation of the Vertical Bone Height of the Palate using CBCT for Placing Micro Implants- A Pilot Study
Sunita Sugumaran1, Ravindra Kumar Jain2, Aravind Kumar3, Sruthi Sinnadurai4, Mary Shelonimissier5
1 Postgraduate Student, Department of Orthodontics, Saveetha Institute of Medical and Technical Science, Chennai, Tamil Nadu, India.
2 Reader, Department of Orthodontics, Saveetha Institute of Medical and Technical Science, Chennai, Tamil Nadu, India.
3 Head, Department of Orthodontics, Saveetha Institute of Medical and Technical Science, Chennai, Tamil Nadu, India.
4 Postgraduate Student, Department of Orthodontics, Saveetha Institute of Medical and Technical Science, Chennai, Tamil Nadu, India.
5 Postgraduate Student, Department of Orthodontics, Saveetha Institute of Medical and Technical Science, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sunita Sugumaran, PH Highroad, Chennai, Tamil Nadu, India.
E-mail: sunita_eco@yahoo.co.in
Introduction
Determining an ideal anatomical location for mini-implant placement is very crucial for successful use of mini-implants in an orthodontic setup. Some of the factors that should be considered while selecting an ideal site for implant placement are soft tissue morphology, interradicular distance, sinus morphology, nerve location, buccolingual bone depth, and cortical thickness. In maxilla, implants are commonly placed in the buccal bone in the anterior and posterior inter radicular regions but in certain instances there is a need to place implants on the palatal side. Median and paramedian sites are recommended for placement of mini-implants in the hard palate. It is important that the measurement of the available vertical bone height is carried out to select the ideal location for placing a mini-implant since this will directly influence stability, and thus success.
Aim
This study aims to evaluate the Vertical Bone Height (VBH) of the palate using a CBCT (Cone Beam Computed Tomography) at different coronal sections postero-anteriorly so as to determine the ideal location for implant placement.
Materials and Methods
This is a cross-sectional study carried out in the department of Orthodontics, Kyungpook national university dental hospital, Daegu from February 2018 to march 2018. CBCT records of 12 patients referred to the department of orthodontics were selected. Sample consisted of 6 adults above 18 years (3 females and 3 males), and 6 children below the age of 18 years (3 females and 3 males). The images were analysed using InVivoDental (Anatomage Inc., San Jose, CA, USA), a volumetric imaging software. The CBCT analysis involves evaluation of series of coronal sections starting from the most posterior section of the palate extending up to the anterior section. In each section, the VBH of the palate was measured at a distance of 5 mm and 10 mm lateral to the midpalate suture on the right and left side.
Results
In adults: the greatest bone height is seen in area mesial to the 1st premolar with a mean of 14.77 mm at a distance of 5 mm from the midline and mean of 17.53 mm at a distance of 10 mm from the midline. In children: the greatest bone height is seen in area mesial to the 1st deciduous molar with a mean of 14.04 mm at a distance of 5 mm from the midline and mean of 16.7 mm at a distance of 10 mm from the midline. The mean Palatal height is higher at 10 mm lateral to midline when compared to 5 mm lateral to midline at every coronal section. The mean palatal height is more in males than in females. No significant difference is seen between the palatal height on the right and the left side.
Conclusion
The palate presents a site of choice for the insertion of miniscrews for orthodontic purposes as it acts as a safe haven for both novice and experienced orthodontists. The thickest part of the palate is the antero-lateral part of the palate. Further multicentric studies with larger sample size in different age ranges are required for better understanding of efficiency and success of palatal implants.
Cone beam computed tomography, Diagnostic images, Micro implant, Palatal height, Vertical bone height
Introduction
A successful orthodontic treatment involves the application of low continuous force on a group of teeth using another teeth/group of teeth as anchor units. Ideally, it is required for the anchor unit to be stable. However, this is not the usual scenario and orthodontists are often faced with the problem of anchor loss. One-way to overcome this would be the usage of skeletal anchorage by the means of Temporary Anchorage Devices (TADs). This would prevent the orthodontist from taxing a tooth or a group of teeth for anchorage requirements. TADs or Mini-implants have gained popularity in the orthodontic fraternity due to its versatility, ease of use, minimal invasiveness, effective biomechanics, ability to avoid surgery, effect on treatment duration and lack of need of patient’s cooperation [1]. Mini-implants are placed to provide anchorage to bring about various orthodontic tooth movements like distalisation of tooth/teeth, mesialisation, intrusion, extrusion, rotation correction, up righting tipped teeth, correction of deep bite, open bite, gummy smile, sagittal skeletal corrections, and also correction of borderline surgical cases [2-5].
Success of the mini-implant depends on many factors and among them these three are very important-Implant placement site, Micro implant design, Surgical technique [6]. The focus of this study is on the implant placement site. Determination of ideal anatomical location for mini-implant placement has been intended by several studies [7,8]. For a mini-implant to be successful, a minimum of 50% of the threaded surface should be embedded in the cortical bone. TADs can be placed in maxilla and mandible at various site, however in maxilla, the site that satisfies most of the requirements is the hard palate. Recently, Palatal skeletal anchorage has been used extensively by orthodontists across the world [9-14]. Mini-implants placed in the palate have showed 90%-95.7% success rate [15] Palatal mini-implants can sustain sufficient orthodontic/orthopaedic loads [16,17].
One of the best location choices historically for a palatal implant was the mid-palatal suture since it boasts a very high bone quantity and quality. However, the exact age at which the midpalate suture completes its ossification is extremely variable [18,19], also a study on dogs has shown that there is a potential inhibition of transverse maxillary growth when implants were placed in the median region of the mid-palate suture [20]. Thus, a logical alternative location is the use of paramedian mini-implants. One of complications of paramedian placement in the palate is perforation into the nasal cavity. Lateral cephalograms that are taken routinely for treatment planning do not offer acceptable screening of palatal depth in the paramedian sites. The success of the mini-implants placed in the paramedian sites highly depends on the quality and density of the bone at the receptor site which can be imaged only by a cone beam CT or CT technology. Since CT involves higher radiation exposure, CBCT is considered the imaging technique of choice.
This study aims to evaluate the vertical bone height available in different coronal sections of the palate postero-anteriorly using a CBCT to determine the ideal location for mini-implant placement.
Materials and Methods
This is a cross-sectional study carried out in the department of Orthodontics, Kyungpook national university dental hospital, Daegu from February 2018 to march 2018. This study was approved by Kyungpook national university dental college. Cone beam computed tomographic records of 12 patients visiting the Department of Orthodontics were randomly selected for the study. This study included records of 6 adults above 18 years (3 females and 3 males), and 6 children below the age of 18 years (3 females and 3 males). Cases with craniofacial malformations, syndromic patients, evidence of trauma, orthognathic surgery, patients with medical and systemic conditions were excluded. The CBCT dicom files were analysed using InVivoDental (Anatomage Inc., San Jose, CA, USA), a volumetric imaging software. The analysis was done in various coronal sections starting from the most posterior section of the palate extending up to the anterior sections.
In adults the coronal sections of the following sites were analysed [Table/Fig-1a-d]:
Coronal sections viewed in InVivo software in adults. a) Mesial to second molar. b) Mesial to first molar. c) Mesial to second premolar. d) Mesial to first premolar.
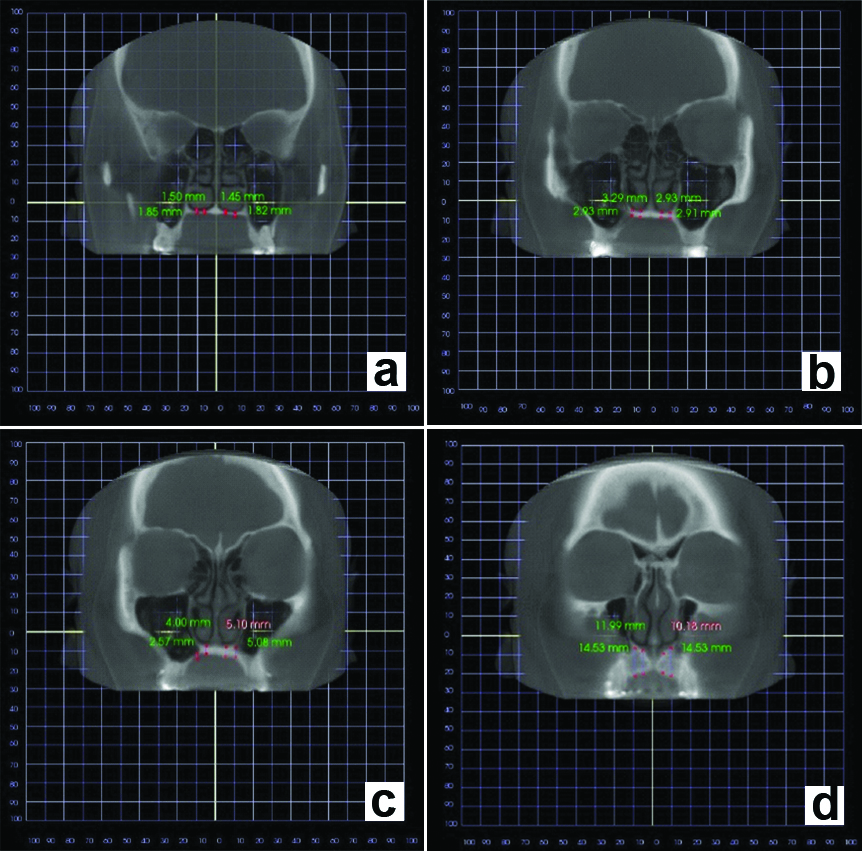
Mesial to the 2nd molar
Mesial to the 1st molar
Mesial to the 2nd premolar
Mesial to the 1st premolar
The various coronal sections in children were as follows [Table/Fig-2a-c]:
Coronal sections used in InVivo software in children. a) Mesial to first permanent molar. b) Mesial to second deciduous molar. c) Mesial to first deciduous molar.
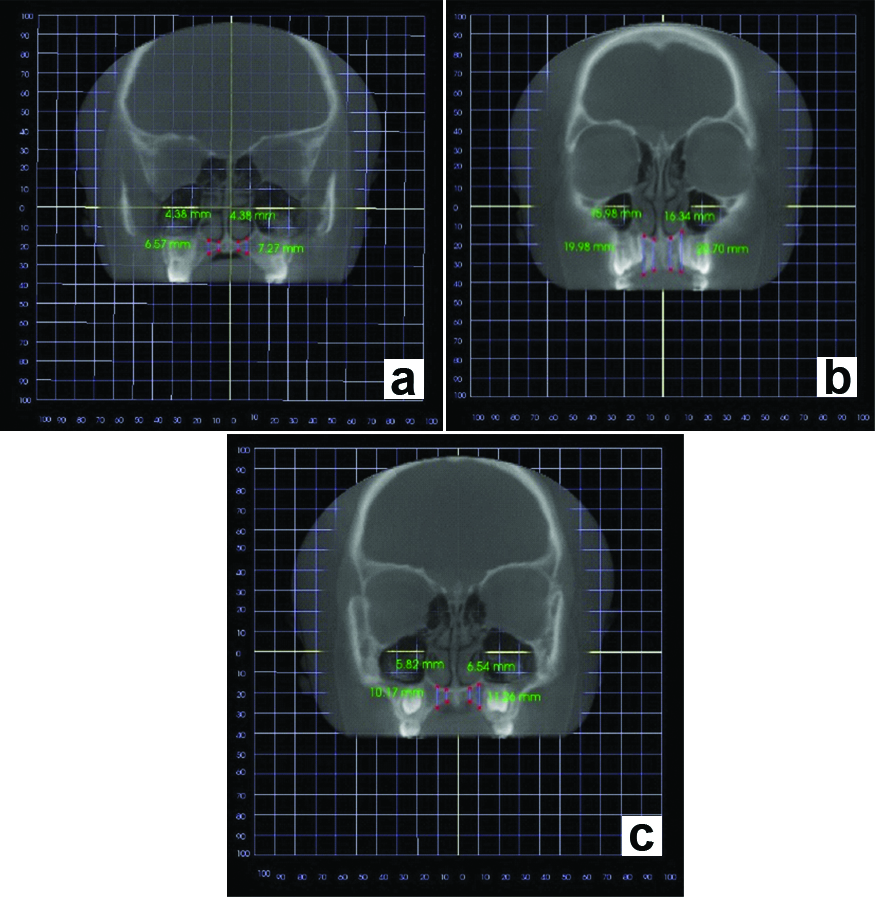
Mesial to the 1st molar
Mesial to the 2nd deciduous molar
Mesial to the 1st deciduous molar.
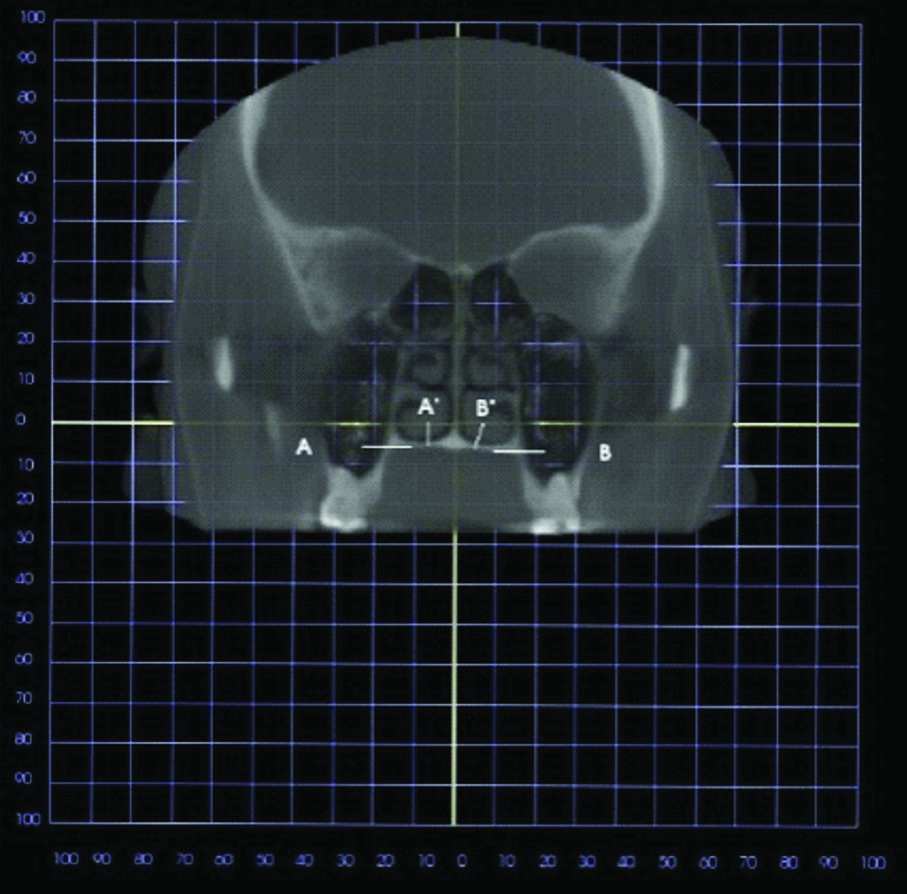
In each section, the VBH of the palate was measured at a distance of 5 mm and 10 mm lateral to the midpalate suture on the right and left side [Table/Fig-3]. To test the intra-examiner reliability, eight randomly selected scans were re-measured one week later by the same investigator. The palatal height measurement was carried out in the eight randomly selected patients, and was carried out by three different operators. The results were compared using analysis of variance and did not show statistically significant differences.
A 5 mm and 10 mm measurements from the median suture. a. 10 mm lateral to the midline suture (right); a’. 5 mm lateral to the midline suture (right); b. 10 mm lateral to the midline suture (left); b’. 5 mm lateral to the midline suture (left).
Statistical Analysis
For each measurement of the coronal section, the mean and standard deviation were calculated. Difference between female and male patients was evaluated by comparing the mean values, and between the measurements of the right and the left side of each section was evaluated using analysis of variance.
Results
From [Table/Fig-4], it can be concluded that the greatest bone height is seen in area mesial to the 1st premolar in adults and similarly, in children the greatest bone height is seen mesial to the 1st deciduous molar [Table/Fig-5]. This is also the site for succeeding 1st premolar. Thus, from this study, it is noted that the palatal height is highest in area mesial to the 1st premolar. In this study, it is evident that for a given individual the palatal height is more at 10 mm lateral to the midline rather than 5 mm lateral to the midline. Such observation is similar in both adults as well as children.
Mean and standard deviation in adult patients.
| MESIAL TO 2nd MOLAR | MESIAL TO 1st MOLAR | MESIAL TO 2nd PREMOLAR | MESIAL TO 1st PREMOLAR |
|---|
| 5 mm | 10 mm | 5 mm | 10 mm | 5 mm | 10 mm | 5 mm | 10 mm |
|---|
| Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left |
|---|
| Mean | 4.183333 | 4.021667 | 5.02 | 5.043333 | 4.25 | 4.195 | 5.405 | 5.648333 | 7.376667 | 7.57 | 9.33 | 9.693333 | 14.59 | 14.96333 | 17.74167 | 17.32 |
| Std. Dev | 1.661429 | 1.351879 | 2.782524 | 3.265705 | 0.787096 | 0.749046 | 1.442439 | 1.559531 | 2.254619 | 1.76327 | 3.976989 | 2.661831 | 2.771317 | 3.711014 | 3.095864 | 2.58723 |
Mean and standard deviation in children.
| MESIAL TO THE 1st MOLAR | MESIAL TO 2nd DECIDUOUS MOLAR | MESIAL TO 1st DECIDUOUS MOLAR |
|---|
| 5 mm | 10 mm | 5 mm | 10 mm | 5 mm | 10 mm |
|---|
| Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | Right | Left |
|---|
| Mean | 4.266667 | 4.246667 | 4.985 | 5.451667 | 6.361667 | 6.856667 | 9.328333 | 9.813333 | 13.92333 | 14.165 | 16.33333 | 17.07333 |
| Std. Dev | 0.861317 | 1.313159 | 1.278808 | 1.883777 | 2.005327 | 2.017986 | 2.559378 | 3.405899 | 2.126609 | 2.364434 | 2.896886 | 2.80074 |
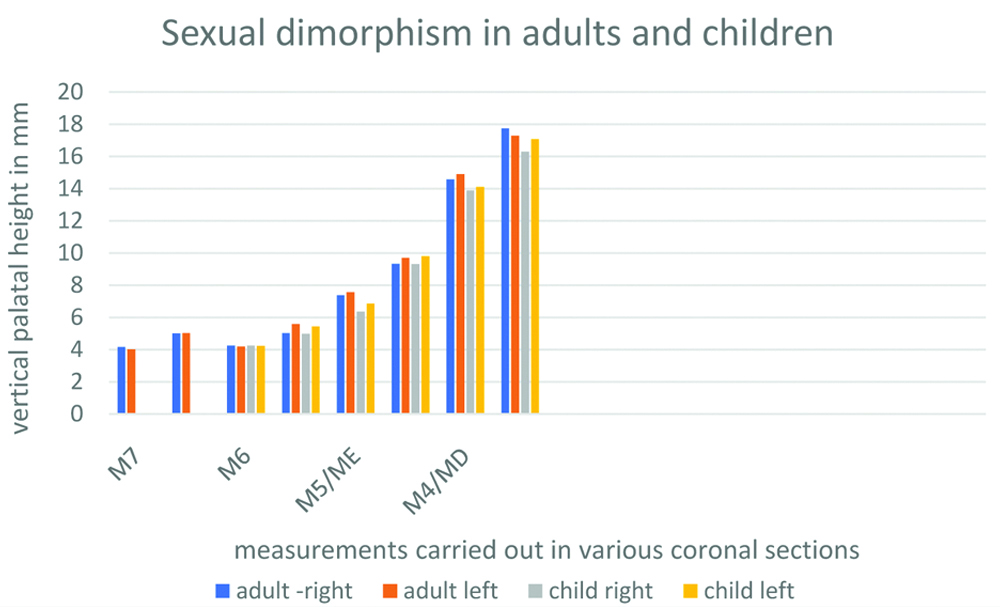
It is also noted that at any given anatomical position, the mean palatal height is higher in males (mean). This sexual dimorphism is similar in both adults as well as children [Table/Fig-6].
Sexual dimorphism in adults and children.
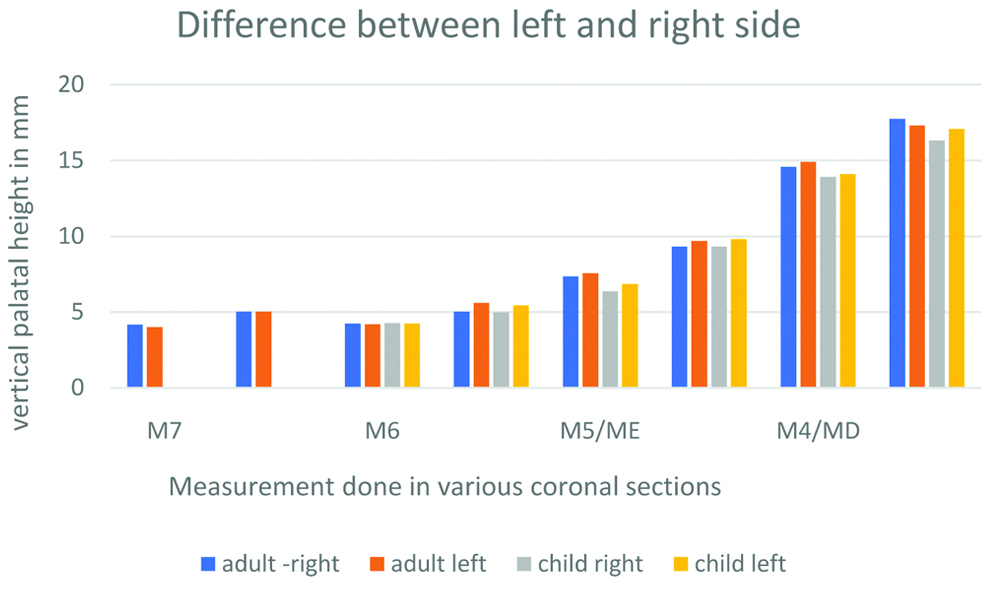
On comparison of mean palatal heights between right and left side in adults and children, it is seen that there is no statistical difference between measurements on either side at any given coronal section. Results were similar for adults and children. The mean values were evaluated [Table/Fig-7].
Vertical bone height difference between the right and the left side in adults and children.
Difference between female and male patients was evaluated by comparing the mean values and between the measurements of the right and the left side of each section was evaluated using analysis of variance.
Discussion
The choice between a median and paramedian palatal mini-implant insertion has been subjected to controversy and debate for several years. In the past, studies have shown that there is no difference between the two patterns regarding retention and stability [21,22]. Advantages of a median mini-implant placement are that there is a reduced risk of injury to the upper incisor roots and more anterior placement of the implant is possible. But at the same time, it has to be noted that there is a high risk of penetration into the incisive canals, which would lead to persistent paraesthesia and eventually implant failure due to lack of adequate bone support. Midpalate mini-implants have also raised issues of inhibition of transverse maxillary growth [23] by damaging the ossifying sutures. A huge variation in the ossification of mid palatal suture questioned the justification of use of the mid palatal implants. In order to overcome this challenge, it would be a safe route to use a paramedian implant. Paramedian implants have all the advantage of the median implant and also doesn’t damage the suture. However, one should keep in mind that the more lateral we move from the midline, the closer we are to the roots of the adjacent teeth. This can be avoided by careful radiographic examination of the insertion site. A lateral cephalogram can be used for measuring VBH in mid palatal implants but one study has reported that the VBH measured with a lateral ceph is 2 mm less than the actual dimension [24,25], hence CBCT is the imaging of choice for acquiring accurate dimension of the VBH of the palate and is the only choice for, measuring the VBH for paramedian placement.
Paramedian implants is currently under the radar by several orthodontists with one of the pioneers being Bernhart T et al., [26,27]. However, there are only a few studies evaluating the success rates of these implants. In a study conducted by Bernhart T et al., [26,27], the success rate was found to be 85.7%, while a study conducted by Zuger J et al., showed success rate of 95.2% [28]. Thus, paramedian implants can be considered a sound alternative to the median implants.
In this study, the vertical bone heights available at 5 mm and 10 mm increments lateral from the midline in the 4 coronal sections of 3 adult patients were measured. Also, vertical bone heights available at 5 mm and 10 mm increments lateral from the midline in 3 coronal sections in patients below 18 years of age were measured. The results suggest that the VBH in the palate is highest at 10 mm from the midline and mesial to the 1st premolar in adults and mesial to 1st deciduous molar in children. At any given section, the mean palatal height is higher in males than females in both adults and females. There is no significant difference between palatal heights on right and left side of the palate in both adults as well as children.
This study justifies the results from previous related studies. Marquezan M et al., concluded from their study that 4 mm posterior to the incisive foramen, in median or paramedian area adjacent to suture are the most suitable areas for micro implant placement in the palate [29]. Winsauer H et al., concluded from their study that the ideal site for implant placement is about 3 mm posterior direction to the incisive foramen and 6 mm lateral to the midpalate suture [30], justifying the results of the current study. Winsauer H et al., also suggests a footprint-like area in the anterior region on the hard palate to be more reliable for safe anchorage. On the other hand, Wilmes B et al., suggested “T zone”, the area immediately posterior to the palatal rugae, to be an ideal location for placement of mini-implants in the palate [31]. The average height of the palate decreases from the anterior to posterior and from the median to the lateral region, thereby indicating the anterior median region of the palate as the ideal site for insertion of mini-implants as concluded by the current study. In the current study, it is seen that males show higher mean VBH when compared to females at any point on the coronal section, justifying the results from the previous studies by Kang S et al., and Moon SH et al [32,33].
Limitation
Since it involved records of patients from another college, the sample size was limited. Study was performed on a different ethnic group. Clinical study is required to substantiate the results.
Conclusion
Vertical Bone height is highest in the anterior part of the palate. The paramedian site shows higher bone height with lower complications when compared to the mid-palatal implant. Thus, paramedian sites can be considered as an alternative, when placing an implant on the palatal surface for orthodontic treatment. However, due to small sample size and ethnic variations, further studies with higher sample size and different ethnic group is required.
[1]. Papadopoulos MA, Tarawneh F, The use of miniscrew implants for temporary skeletal anchorage in orthodontics: a comprehensive reviewOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 103:e6-15.10.1016/j.tripleo.2006.11.02217317235 [Google Scholar] [CrossRef] [PubMed]
[2]. Nienkemper M, Wilmes B, Pauls A, Yamaguchi S, Ludwig B, Drescher D, Treatment efficiency of miniimplant-borne distalization depending on age and second molar eruptionJ Orofac Orthop 2014 75:118-32.10.1007/s00056-013-0199-z24577015 [Google Scholar] [CrossRef] [PubMed]
[3]. Wilmes B, Nienkemper M, Nanda R, Lübberink G, Drescher D, Palatally anchored maxillary molar mesialization using the mesialsliderJ Clin Orthod 2013 47:172-79. [Google Scholar]
[4]. Park HS, Jang BK, Kyung HM, Maxillary molar intrusion with micro-implant anchorage (MIA)Australian Orthodontic Journal 2005 21(2):129-35. [Google Scholar]
[5]. Wilmes B, Drescher D, Vertical periodontal ligament distraction-A new method for aligning ankylosed and displaced caninesJ Orofac Orthop 2009 70:213-23.10.1007/s00056-009-8811-y19484414 [Google Scholar] [CrossRef] [PubMed]
[6]. Wilmes B, Drescher D, Impact of insertion depth and predrilling diameter on primary stability of orthodontic miniimplantsAngle Orthod 2009 79:609-14.10.2319/071708-373.119537867 [Google Scholar] [CrossRef] [PubMed]
[7]. Poggio MP, Incorvati C, Velo S, Carano A, “Safe Zones”: A guide for miniscrew positioning in the maxillary and mandibular archAngle Orthod 2006 76:191-97. [Google Scholar]
[8]. Deguchi T, Nasu M, Quantitative evaluation of cortical bone thickness with computed tomographic scanning for orthodontic implantsAm J Orthod Dentofacial Orthop 2006 129(6):721e7-12.10.1016/j.ajodo.2006.02.02616769488 [Google Scholar] [CrossRef] [PubMed]
[9]. Lee JS, Kim DH, Park YC, Kyung SH, Kim TK, The efficient use of midpalatal miniscrew implantsAngle Orthod 2004 74(5):711-14. [Google Scholar]
[10]. Melsen B, Mini-Implants: Where Are We?J Clin Orthod 2005 39(9):539-47.quiz 531-32 [Google Scholar]
[11]. Carano A, Velo S, Leone P, Siciliani G, Clinical implication of the miniscrew anchorage systemJ Clin Orthod 2005 39(1):9-24.quiz 29-30 [Google Scholar]
[12]. Park HS, A Miniscrew-assisted transpalatal arch for use in lingual orthodonticsJ Clin Orthod 2006 40(1):12-16. [Google Scholar]
[13]. Kircelli BH, Pektas Z, Kircelli C, Maxillary molar distalization with a bone-anchored pendulum applianceAngle Orthod 2006 76(4):650-59. [Google Scholar]
[14]. Kinzinger G, Wehrbein H, Byloff FK, Yildizhan F, Diedrich P, Innovative anchorage alternatives for molar distalization-an overviewJ Orofac Orthop 2005 66(5):397-413.10.1007/s00056-005-0512-616231115 [Google Scholar] [CrossRef] [PubMed]
[15]. Männchen R, Schätzle M, Success rate of palatal orthodontic implants: a prospective longitudinal studyClin Oral Impl Res 2008 19:665-69.10.1111/j.1600-0501.2007.01512.x18492083 [Google Scholar] [CrossRef] [PubMed]
[16]. Kyung SH, Hong SG, Park YC, Distalization of maxillary molars with a midpalatal miniscrewJ Clin Orthod 2003 37(1):22-26. [Google Scholar]
[17]. Misch CE, Contemporary Implant Dentistry 1999 2nd edMosby, StLouis:11310.1097/00008505-199901000-00013 [Google Scholar] [CrossRef]
[18]. Melsen B, Palatal growth studied on human autopsy material A histologic microradiographic studyAmerican Journal of Orthodontics 1975 68:42-54.10.1016/0002-9416(75)90158-X [Google Scholar] [CrossRef]
[19]. Schlegel KA, Srour S, Neukam FW, Fenner M, Felszeghy E, Which region of the median palate is a suitable location of temporary orthodontic anchorage devices? A histomorphometric study on human cadavers aged 15-20 yearsClinical Oral Implants Research 2009 20:306-12.10.1111/j.1600-0501.2008.01647.x19397643 [Google Scholar] [CrossRef] [PubMed]
[20]. Asscherickx K, Hanssens JL, Wehrbein H, Sabzevar MM, Orthodontic anchorage implants inserted in the median palatal suture and normal transverse maxillary growth in growing dogs: A biometric and radiographic studyAngle Orthod 2005 75:826-31. [Google Scholar]
[21]. Nienkemper M, Pauls A, Ludwig B, Drescher D, Stability of paramedian inserted palatal mini-implants at the initial healing period: A controlled clinical studyClin Oral Implants Res 2015 26:870-75.10.1111/clr.12321243730224 [Google Scholar] [CrossRef] [PubMed]
[22]. Nienkemper M, Wilmes B, Pauls A, Drescher D, Mini-implant stability at the initial healing period: A clinical pilot studyAngle Orthod 2014 84:127-33.10.2319/040813-271.123883287 [Google Scholar] [CrossRef] [PubMed]
[23]. Knaup B, Yildizhan F, Wehrbein H, Age-related changes in the midpalatal suture. A histomorphometric studyJournal of Orofacial Orthopedics 2004 65:467-74.10.1007/s00056-004-0415-y15570405 [Google Scholar] [CrossRef] [PubMed]
[24]. Schlegel KA, Kinner F, Schlegel KD, The anatomic basis for palatal implants in orthodonticsThe International journal of Adult Orthodontics and Orthognathic Surgery 2002 17:133-39. [Google Scholar]
[25]. Wehrbein H, Merz BR, Diedrich P, Palatal bone support for orthodontic implant-a clinical and radiological studyEur J Orthod 1999 21:65-70.10.1093/ejo/21.1.6510191579 [Google Scholar] [CrossRef] [PubMed]
[26]. Bernhart T, Vollgruber A, Gahleitner A, Dörtbudak O, Haas R, Alternative to the median region of the palate for placement of an orthodontic implantClinical Oral Implants Research 2000 11:595-601.10.1034/j.1600-0501.2000.011006595.x11168253 [Google Scholar] [CrossRef] [PubMed]
[27]. Bernhart T, Freudenthaler J, Dörtbudak O, Bantleon HP, Watzek G, Short epithetic implants for orthodontic anchorage in the paramedian region of the palate. A clinical studyClinical Oral Implants Research 2001 12:624-31.10.1034/j.1600-0501.2001.120611.x11737107 [Google Scholar] [CrossRef] [PubMed]
[28]. Züger J, Pandis N, Wallkamm B, Grossen J, Katsaros C, Success rate of paramedian palatal implants in adolescent and adult orthodontic patients: a retrospective cohort studyEuropean Journal of Orthodontics 2014 36(1):22-25.10.1093/ejo/cjt00323525601 [Google Scholar] [CrossRef] [PubMed]
[29]. Marquezan M, Nojima LI, Freitas AO, Baratieri C, Alves Júnior M, Nojima Mda C, Tomographic mapping of the hard palate and overlying mucosaBrazilian Oral Research 2012 26(1):36-42.10.1590/S1806-8324201200010000722344336 [Google Scholar] [CrossRef] [PubMed]
[30]. Winsauer H, Vlachojannis C, Bumann A, Vlachojannis J, Chrubasik S, Paramedian vertical palatal bone height for miniimplant insertion: a systematic reviewEur J Orthod 2014 36(5):541-49.10.1093/ejo/cjs06823221896 [Google Scholar] [CrossRef] [PubMed]
[31]. Wilmes B, Ludwig B, Vasudavan S, Nienkemper M, Drescher D, The Tzone: median vs. paramedian insertion of palatal mini-implantsJ Clin Orthod 2016 50:543-51. [Google Scholar]
[32]. Kang S, Lee SJ, Ahn SJ, Heo MS, Kim TW, Bone thickness of the palate for orthodontic mini-implant anchorage in adultsAmerican Journal of Orthodontics and Dentofacial Orthopedics 2007 131:S74-S81.10.1016/j.ajodo.2005.09.02917448390 [Google Scholar] [CrossRef] [PubMed]
[33]. Moon SH, Park SH, Lim WH, Chun YS, Palatal bone density in adult subjects: implications for mini-implant placementThe Angle Orthodontist 2010 80:137-44.10.2319/011909-40.119852653 [Google Scholar] [CrossRef] [PubMed]