Penile gangrene is extremely rare. It spreads very rapidly to surrounding structure and have high mortality rate. Its aetiology can be infectious, traumatic or vasculogenic. Precipitating factors can be elicited with careful history and examination. Its management depends upon clinical presentation, which includes serial debridement, partial or total penectomy and treatment of underlying pathology. Here, we are reporting three cases of penile gangrene presented in emergency, one of which was managed by total penectomy, and other two by active debridement with supra-pubic catheter.
Introduction
Fournier Gangrene (FG) is a rapidly progressive life threatening soft tissue synergistic infection of genitalia, perineum, perianal region and anterior abdominal wall. Fournier’s gangrene is the necrotising soft tissue infection which mainly involves scrotum but, penile involvement is rarest presentation. Fournier gangrene generally occurs in old age, malnourished patient, chronic alcoholic, diabetic and immuno-compromised patient. Its management depends on the early recognition of disease. There are different treatment modalities of fournier gangrene, which includes broad spectrum antibiotics, aggressive debridement and penile amputation depending on the condition at the time of presentation. We shared our experience on the presentation and management of three cases of isolated fournier’s gangrene of penis to draw attention to this rare condition.
Case Presentation
Case-1
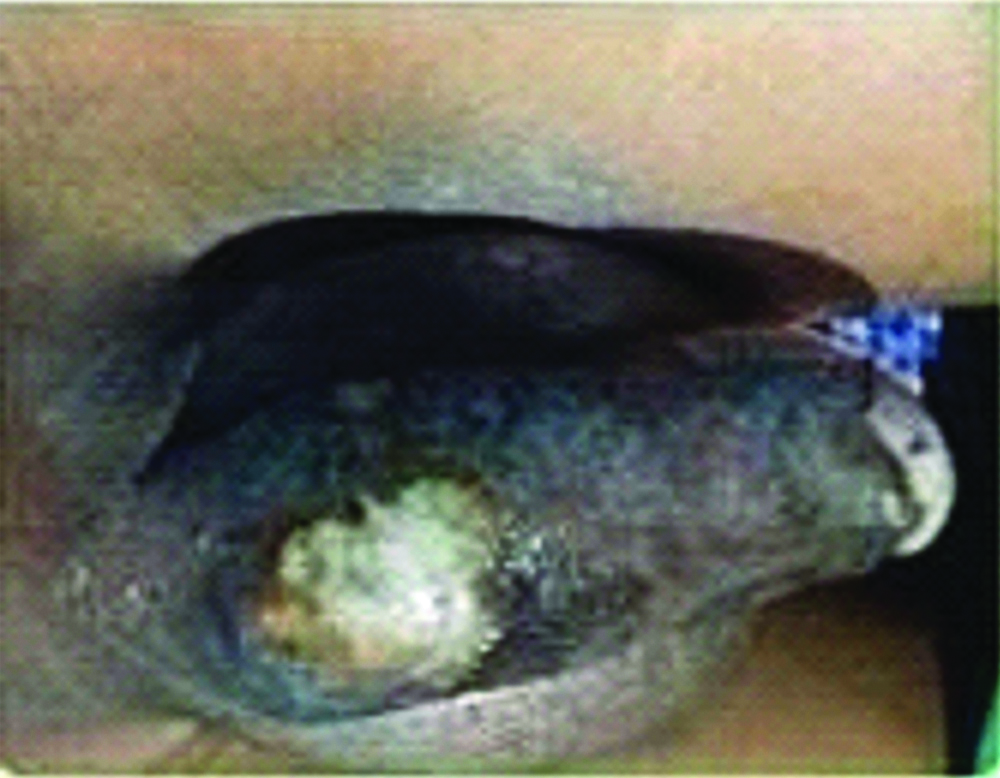
A 61-year-old male presented in emergency with complaints of pain, discolouration of penile skin, ulceration and foul smelling discharge for 10 days with history of trauma, 15 days back. He was a known case of coronary artery disease since four years; cardiac stent was put two years back. Patient had no other comorbid conditions. He was a chronic smoker (one pack of tobacco per day). Patient was afebrile with pulse 110/min, BP-120/70 mm of Hg, respiratory rate (RR)-18/min. Examination of external genitalia revealed the gangrene of the glans and shaft of penis. Also, there was ulcer with foul smelling discharge present at the base of penis [Table/Fig-1]. There was no inguinal lymphadenopathy. Testes and spermatic cord were normal. Laboratory investigations revealed-Hb-11 g/ dL, Haematocrit-41%, WBC-20,000/mm3, Blood urea-21 mg/dL, Serum Creatinine-1.2 mg/dL, Na/K-136/5.1 mEq/L, RBS-106 mg/dL. Urine examination revealed numerous pus cells. FGSI (Fournier’s gangrene severity index) was four, the score is calculated based on nine parameters, which ranges from 0 to 4 [1]. Broad spectrum antibiotics (intravenous amoxicillin and clavulanic acid combination 1.2 gm 8 hourly and injection clindamycin 600 mg 12 hourly) was started. Patient underwent surgery and total penectomy with supra- pubic catheterization [Table/Fig-2]. The postoperative period was uneventful and patient was discharged on 5th postoperative day. Histopathology of amputated penis revealed gangrene. The patient was followed up after 1 month, patient was doing fine and voiding through suprapubic catheter.
Penile gangrene with purulent discharge from the base of penis.

After total Penectomy of patient.

Case-2
A 46-year-old male presented in emergency with complaint of blackish discoloration of penile skin since 15 days. He was a known case of Diabetes Mellitus (DM) type-2 since three years, on oral hypoglycaemic medication. Diabetes was uncontrolled at the time of presentation (RBS-196 mg/dL). He was a chronic smoker (one pack of tobacco cigarettes per day). Patient was afebrile, pulse-100 beats/min, BP-120/70 mm of Hg, respiratory rate-20 breaths/min. Examination of external genitalia showed blackish discolouration of penile skin with no discharge and ulceration [Table/Fig-3,4]. There was no inguinal lymphadenopathy. The scrotum, testes, spermatic cords were normal. Laboratory investigations revealed Hb-9 g/dL, Haematocrit-38%, WBC-19000/dL, Blood urea-25 mg/dL, serum creatinine-0.6 mg/dL, Na/K-150/4.0 mEq/L, RBS-196 mg/dL. FGSI was 2. Patient was put on higher intravenous antibiotics (intravenous amoxicillin and clavulanic acid combination 1.2 gm 8 hourly and injection clindamycin 600 mg 12 hourly). Patient was taken up for emergency surgery, debridement and excision of gangrenous tissue was done [Table/Fig-5]. SPC was performed to divert urine from surgical site. Patient was discharged on postoperative day 4 with the advice of wound care, dressing and antibiotics. On follow-up, wound bed was healthy and was covered with split skin graft after 3 months.
Penile gangrene on the dorsum.
Penile gangrene on the ventral side.

Post surgical debridement of penile gangrene.

Case-3
A 55-year-old male presented in emergency with complaint of blackish discolouration of penile skin since 10 days. He had no comorbidity and was non-smoker, non-alcoholic. The Patient was afebrile, pulse-98 beats/min, BP-110/70 mm of Hg, RR-14 breaths/ min. Examination of external genitalia showed blackish discolouration of skin of penis and gangrenous patch present on the shaft. There was no inguinal lymphadenopathy. The scrotum, testes, spermatic cords were normal. Digital rectal examination was normal. Laboratory investigation revealed- Hb-12 g/dL, Haematocrit-36%, WBC-17000/mm3, Blood urea-30 mg/dL, Serum creatinine-1.6 mg/dL, Na/K-133/3.5 mEq/L, RBS-130 mg/dL, serum bicarbonate-38 meq/L. Urine microscopy and culture showed no abnormalities, FGSI was two. Patient was put on broad spectrum antibiotics (intravenous amoxicillin and clavulanic acid combination 1.2 gm 8 hourly and injection clindamycin 600 mg 12 hourly) and taken for emergency surgical debridement [Table/Fig-6]. Following serial debridement and dressing, the wound was healthy and patient was discharged with advice.
Post debridement appearance of FG of penis.

Discussion
Fournier’s gangrene is necrotising fasciitis of the perineal and genitourinary region which appears more frequently in males [2-4]. It is mostly seen at an advanced age, most frequently seen between age of 40-60 years [1,5]. Necrotising fasciitis is a bacterial infection commonly referred as the “flesh eating disease”. This disease usually involves the scrotum (30%), perineum (50%), or ant abdominal wall (20%) [6]. Isolated penile gangrene is rare due to the rich collateral circulation of penis (branches of internal pudendal artery named dorsal, cavernosal, and bulbourethral artery). Penile fournier’s gangrene is also known as penile necrotizing fasciitis or wet gangrene of penis [3]. It was first described by Baurienne in 1764 [7], as an idiopathic soft tissue necrosis leading to gangrene, but disease was named after Fournier JA (French venereologist) in 1883, who presented a case of perineal gangrene in young man [8]. The mortality and morbidity ranges from 10-20% [9] and up to 60% respectively. It spread rapidly along the shaft and may affect abdominal wall. According to the literature, risk factors of penile gangrene includes: renal insufficiency, diabetes mellitus, thromboembolic, coagulopathy, previous operation, ligation of penile circulation, peripheral vascular disease and kaposi’s sarcoma [10,11]. DM is the most common comorbidity associated with FG [1,5]. Other factors like UTI, urethritis, immunodeficiency state and lymphoproliferative disease, may also contribute [5,12].
Fournier’s gangrene represents polymicrobial infection (both aerobic and anaerobic organism are present) [2-4]. Escherichia coli and Bacteroides species are the predominant aerobe and anaerobes respectively. Others are Proteus, staphylococcus, Enterococcus, aerobic and anaerobic streptococcus, pseudomonas, klebsiella and clostridium strains [12]. Laor E et al., reported E.coli and streptococcus species are most commonly isolated organism and stated that staphylococcus and enterococcus were more frequently isolated when compared to bacteroides [1]. Its treatment includes immediate hospitalisation, broad spectrum antibiotics, and timely surgical debridement. If disease progresses, by necrosis of skin, crepitus or induration of the shaft then partial or total penectomy can be done depending upon necrosis [2-4,13].
In 1995 Laor E et al., developed fournier’s gangrene severity index (FGSI), to assess severity of disease, which is most widely accepted index [1]. There are nine parameters, which are graded on 0-4 scale (Heart rate, temperature, respiratory rate, serum Na and K level, serum creatinine, serum bicarbonate, haematocrit and leucocyte count). FGSI score greater than 9 had 75% probability of mortality [1].
In a series of isolated fournier’s gangrene of penis published in 2016, four cases were reported in a period of seven years (2006-2013), all of whom were managed with intravenous antibiotics and debridement [13]. Akbulut F et al., reported a similar case of Fournier’s gangrene involving the glans in a 77-year-old diabetic gentleman with a five day history of pain, discolouration which was managed by partial penectomy [3]. About a year later Temiz et al., reported isolated penile Fournier’s gangrene in a 62-year-old gentleman requiring subtotal penectomy where they performed closure with a dartos fascial flap enclosing urethra and a penile skin flap covering spongiosis [14]. The same year De S et al., published a case of fournier’s gangrene necessitating total penectomy [15]. In our cases, we had to do total penectomy with suprapubic catheterization in one patient, and rest two underwent surgical debridement with suprapubic catheterization.
Conclusion
Isolated Fournier’s gangrene of penis is rare and irreversible process. Early recognition, correction of underlying disease, co-morbidity, broad-spectrum antibiotic, and aggressive debridement can prevent wound liquefaction, preserve more penile length and improve quality of life.
Patients consent: Obtained
[1]. Laor E, Palmer LS, Tolia BM, Reid RE, Winter HI, Outcome prediction in patients with Fournier’s gangreneJ Urol 1995 154:89-92.10.1016/S0022-5347(01)67236-7 [Google Scholar] [CrossRef]
[2]. Rizos S, Filippou DK, Condilis N, Filippou G, Trigka A, Skandalakis P, Fournier’s gangrene: Immediate diagnosis and multimodality treatment is the cornerstone for successful outcomeAnn Ital Chir 2005 76(6):563-67. [Google Scholar]
[3]. Akbulut F, Kucuktopu O, Sonmezay E, Simsek A, Ozgor F, Gurbuz ZG, Partial penectomy after debridement of a Fournier’s gangrene progressing with an isolated penile necrosisUlus Travma Acil Cerrahi Derg 2014 20(5):385-88.10.5505/tjtes.2014.9363625541853 [Google Scholar] [CrossRef] [PubMed]
[4]. Yucel M, Ozpek A, Basak F, Kilic A, Unal E, Yüksekdağ S, Fournier’s gangrene: a retrospective analysis of 25 patientsUlus Travma Acil Cerrahi Derg 2017 23(5):400-04.10.5505/tjtes.2017.0167829052826 [Google Scholar] [CrossRef] [PubMed]
[5]. Doluoglu OG, Karagoz MA, Kilinc MF, Karakan T, Yuceturk CN, Sarici H, Overview of different scoring systems in fournier’s Gangrene and assessment of prognostic factorsTurk J Urol 2016 42(3):190-96.doi;10.5152/tud.2016.1419410.5152/tud.2016.1419427635295 [Google Scholar] [CrossRef] [PubMed]
[6]. Singam P, Wei KT, Ruffey A, Lee J, Chou TG, Fournier’s Gangrene: A case of Neglected symptoms with Devastating physical lossMalays J Med Sci 2012 19(3):81-84. [Google Scholar]
[7]. Nathan B, Fournier’s gangrene: a historical vignetteCan J Surg 1998 41(1):72 [Google Scholar]
[8]. Fournier JA, Gangrene foudroyante de la VergeSemaine Medicine 1883 :3345-48. [Google Scholar]
[9]. Eke N, Fournier gangrene: A review of 1726 casesBr J Surg 2000 87(6):718-28.10.1046/j.1365-2168.2000.01497.x10848848 [Google Scholar] [CrossRef] [PubMed]
[10]. Harris CF, Mydlo JH, Ischemia & gangrene of the penisJ Urol 2003 169(5):179510.1097/01.ju.0000057796.64080.3a12686840 [Google Scholar] [CrossRef] [PubMed]
[11]. Vijayan P, Gangrene of penis in a diabetic male with multiple amputations and follow upIndian J Urol 2009 25(1):123-25.10.4103/0970-1591.4555019468442 [Google Scholar] [CrossRef] [PubMed]
[12]. Eke N, Raphael JE, Fournier’s gangrene. In: Vitin A, editorGangrene-Current concept and management options. Rijeka: in Tech 2011 :37-48.10.5772/24293 [Google Scholar] [CrossRef]
[13]. Obi A, Isolated Fournier’s gangrene of penisNiger J clin Pract 2016 19(3):426-30.10.4103/1119-3077.17929727022814 [Google Scholar] [CrossRef] [PubMed]
[14]. Temiz MZ, Yuruk E, Aykan S, Tuken M, Kandirali E, Isolated penile Fournier’s gangrene presenting with glans penis involvementJ coll physicians Surg Pak 2015 25:S140-41. [Google Scholar]
[15]. De S, Belsante MJ, Tausch TJ, Simhan J, A case of fournier’s gangrene necessitating total penectomyCan J Urol 2015 22(6):8108-11. [Google Scholar]