A Unique Case of Mandibular Bony Extension in the Vicinity of Superior Pharyngeal Constrictor
Leyla Berna Çağirankaya1
1 Associate Professor, Department of Dentomaxillofacial Radiology, Hacettepe University, Faculty of Dentistry, Sihhiye, Ankara, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Leyla Berna Çagğırankaya, Associate Professor, Department of Dentomaxiollofacial Radiology, Hacettepe University, Faculty of Dentistry, Sihhiye-06100, Ankara, Turkey.
E-mail: lbartvinli@yahoo.com
Mandible, Muscles of pharynx, Mylohyoidridge
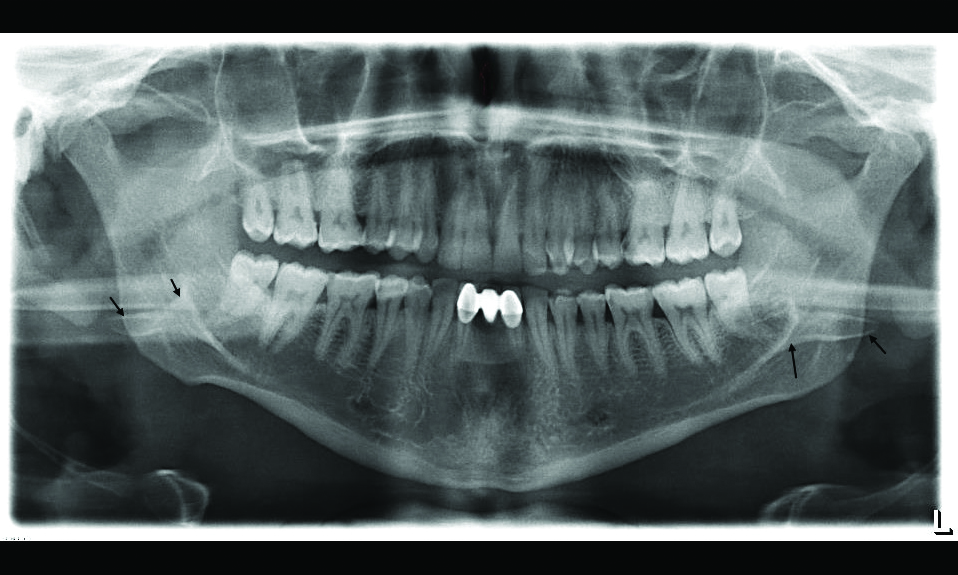
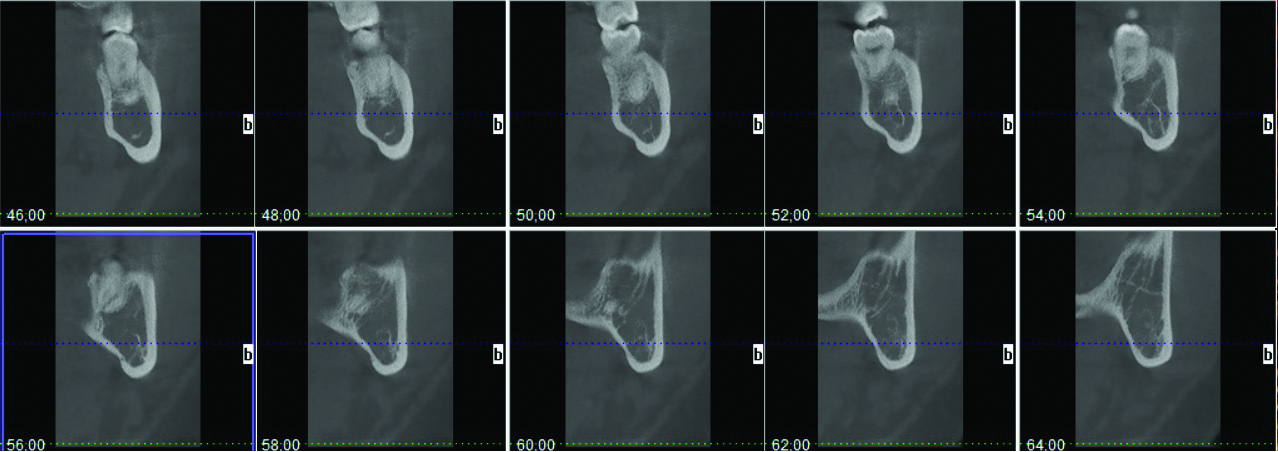
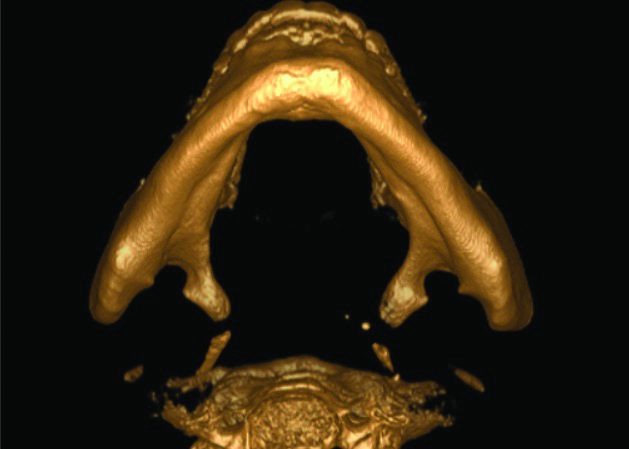
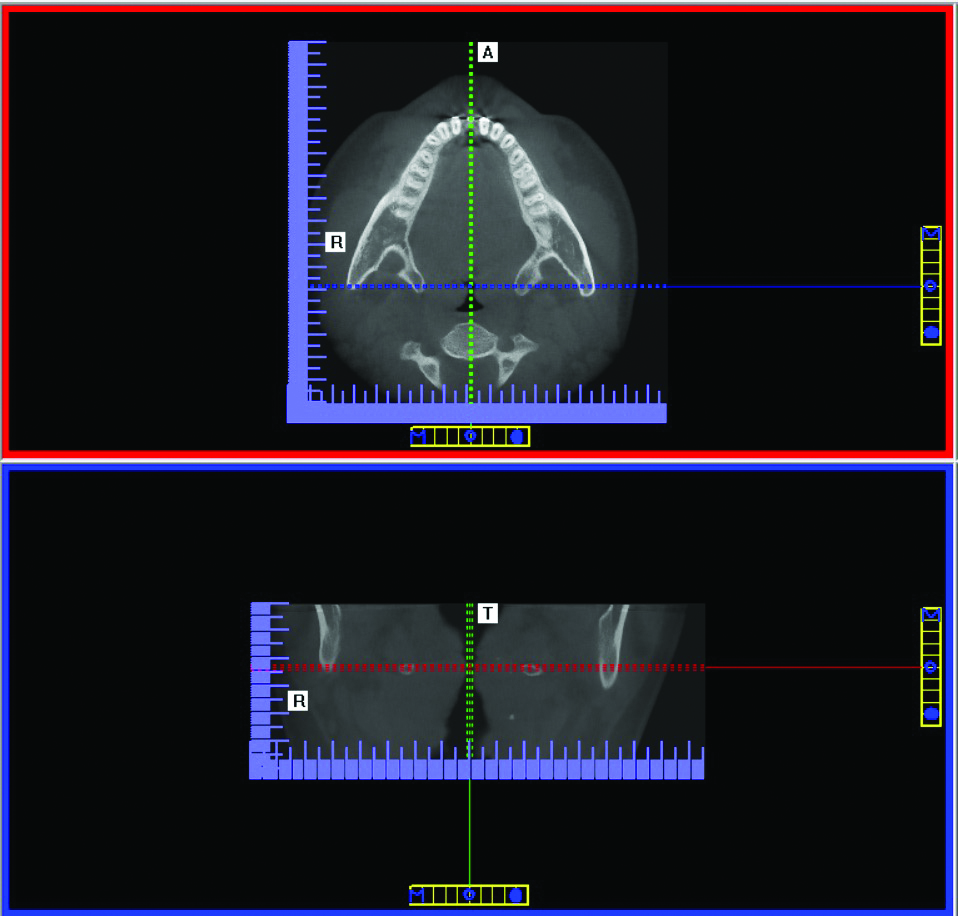
A 28-year-old male attended a dental faculty for a routine dental examination. During clinical examination, the patient with normal facial appearance reported no current systemic diseases. When the digital panoramic X-ray was examined, bilateral symmetrical bone structures related to the distal end of mylohyoid ridge was observed [Table/Fig-1]. Detailed radiographic examination was done with Cone Beam Computed Tomography (CBCT) (iCAT_Next Generation, Imaging Sciences International, Hatfield, PA, USA). CBCT examination confirmed medially extending bony structures arising from the end of the mylohyoid ridge [Table/Fig-2]. Bony structures were identical in both figure and location [Table/Fig-3]. Furthermore, CBCT revealed reduction in the oropharyngeal airway dimension in the vicinity of the structure [Table/Fig-4]. However, the patient has not reported any complaint.
Panoramic radiograph of the patient. Arrows point to the aberrant structures related with the distal end of mylohyoid ridges. Radiopaque bands above them corresponds to the ghost images of the structures.
Cross-sectional images delinate that structures have bony architecture and arise from the end of the mylohyoid ridge.
A 3D CBCT view demonstrates identical structures on both side of the mandible. Shape and localisation of aberrant bone are rather compatible with superior pharyngeal constrictor.
Axial and sagital views indicate reduction in the oropharnygeal airway dimension in the vicinity of the structures.
Discussion
Fibres of the superior pharyngeal constrictors arise partly from the posterior end of the mylohyoid line and curve back into the median pharyngeal raphe [1]. In the present case, although relevant soft tissues could not be analysed due to the limitation of CBCT [2], these bony extensions were rather compatible with superior pharyngeal constrictor in shape and localisation. Therefore, they were speculated to be related to the muscles of pharynx.
There are reported cases of prominent bony extensions of mandible at the muscle attachment areas [3,4]. However, to the best of author’s knowledge, this case is a unique instance in the vicinity of pharyngeal muscles.
The differential diagnosis of the case includes replication of mandibular segments which is an example of diprosopus (craniofacial duplication). Craniofacial duplication is a rare craniofacial anomaly. While true diprosopus refers to the complete duplication of facial structures with two faces on a single head, partial craniofacial duplication describes a broad spectrum of deformities and malformations. Duplication of the jaws may present as isolated parts, with or without involvement of the dentition, such as mandibular condyle, ascending ramus, palate, or alveolar arch duplications [5]. In the present case, extensions were rather compatible with superior pharyngeal constrictor in shape and localisation. Therefore, they were considered as associated with pharyngeal muscles.
Panoramic radiographs have many useful applications in dentistry but require diligence on the part of the observer to examine the image throughly [6]. A systematic approach to the interpretation of this image would reveal many occult conditions. However, in similar cases where panoramic radiography is not sufficient, CBCT would be beneficial. Yet, it must be emphasised that; although CBCT applications provide obvious benefits in the assessment of dentomaxillofacial region with lower effective radiation doses than medical CT, it should be used only in correct indications considering the necessity and potential hazards of the examination [2].
[1]. Williams PL, Dyson M, SplanchnologyIn: Gray’s Anatomy 1989 Churchill Livingstone, UK:1245-1450. [Google Scholar]
[2]. Kamburoğlu K, Use of dentomaxillofacial cone beam computed tomography in dentistryWorld J Radiol 2015 7(6):128-30.10.4329/wjr.v7.i6.12826120381 [Google Scholar] [CrossRef] [PubMed]
[3]. Pauna MR, Babiuc I, Farcaşiu AT, Prosthodontic management of an extreme atrophy of the mandible correlated with a prominent genial tubercleRom J Morphol Embryol 2015 56(2 Suppl):876-70. [Google Scholar]
[4]. Jindal G, Jindal S, Sharma P, Singla A, Rare enlargement of genial tubercles and its management: a case reportJCDR 2015 9(11):23-24.10.7860/JCDR/2015/16237.682726673984 [Google Scholar] [CrossRef] [PubMed]
[5]. Costa MA, Borzabadi-Farahani Ali, Lara-Sanchez PA, Schweitzer D, Jacobson L, Clarke N, Partial craniofacial duplication: a review of the literature and a case reportJournal of Cranio-Maxillo-Facial Surgery 2014 42:290-94.10.1016/j.jcms.2013.05.01623969147 [Google Scholar] [CrossRef] [PubMed]
[6]. Perschbacher S, Interpretation of panoramic radiographsAust Dent J 2012 57(1 Suppl):40-45.10.1111/j.1834-7819.2011.01655.x22376096 [Google Scholar] [CrossRef] [PubMed]