Management of Occlusion in a Completely Edentulous Patient with Abnormal Jaw Relation
VT Abdurahiman1, M Shammas2, M Quassem3, Sanju John Jolly4
1 Associate Professor, Department of Prosthodontics, Ibn Sina National College, Jeddah, Saudi Arabia.
2 Associate Professor, Department of Prosthodontics, Ibn Sina National College, Jeddah, Saudi Arabia.
3 Assistant Professor, Department of Prosthodontics, Ibn Sina National College, Jeddah, Saudi Arabia.
4 Specialist Prosthodontist, Department of Prosthodontics, Ministry of Health, Najran, Saudi Arabia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abdurahiman VT, Tushara, PO Vakkad, Paravanna via, Malappuram DT, Kerala-676502, India.
E-mail: drsajidh@hotmail.com
Complete edentulous patients are not an uncommon finding in day to day prosthodontic clinical practice. Retention and stability are important key factors in successful treatment of a complete denture patient. A practitioner must always plan his treatment depending on various situations encountered in the patient’s mouth. Maxillomandibular relation, which involve deviation from normal situations occurs with considerable frequency and are often quite challenging to the dentist in offering a good treatment plan. The importance of teeth arrangement with a stable occlusion in maintaining the stability of a denture is well documented. This presentation highlights a case with small maxillary arch and a wide mandibular arch which was managed successfully by a cross arch arrangement of artificial teeth.
Cross arch arrangement, Occlusal scheme, Orthognathic, Prognathic, Retention, Stability, Teeth arrangement
Case Report
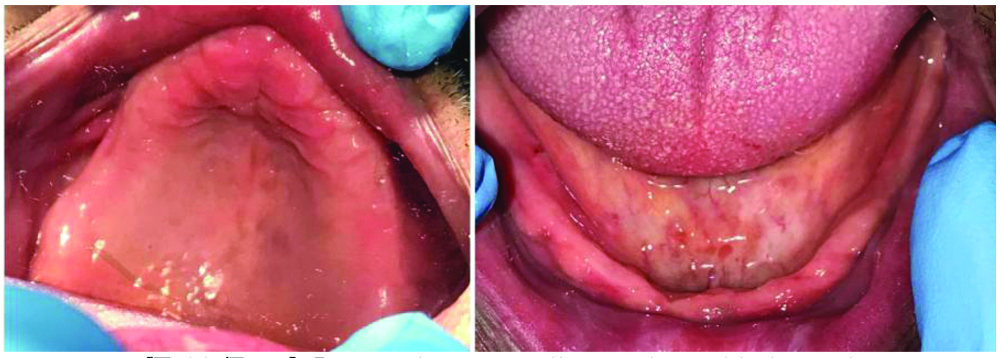
A 65-year-old male reported with a chief complaint to replace his missing teeth. Extra oral examination showed that his facial profile was straight. His skin and TMJ examination were normal. On intraoral examination, mucosa and other areas were found normal except in ridge relation. It revealed a mandibular prognathic ridge relation to the maxilla. The mandibular arch was wider than the maxillary arch [Table/Fig-1]. No abnormalities were found in his Orthopantomogram (OPG). No other abnormalities were detected elsewhere in the oral cavity. A diagnosis of upper and lower completely edentulous arches with a mandibular prognathic ridge relation was made.
Intraoral view maxillary and mandibular arch.
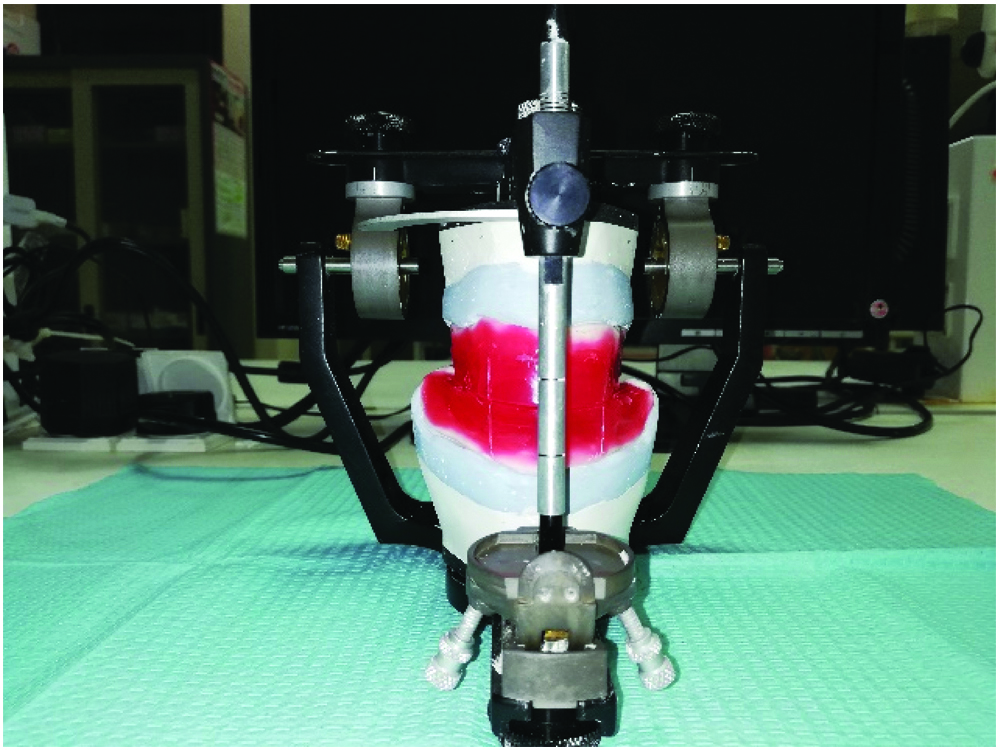
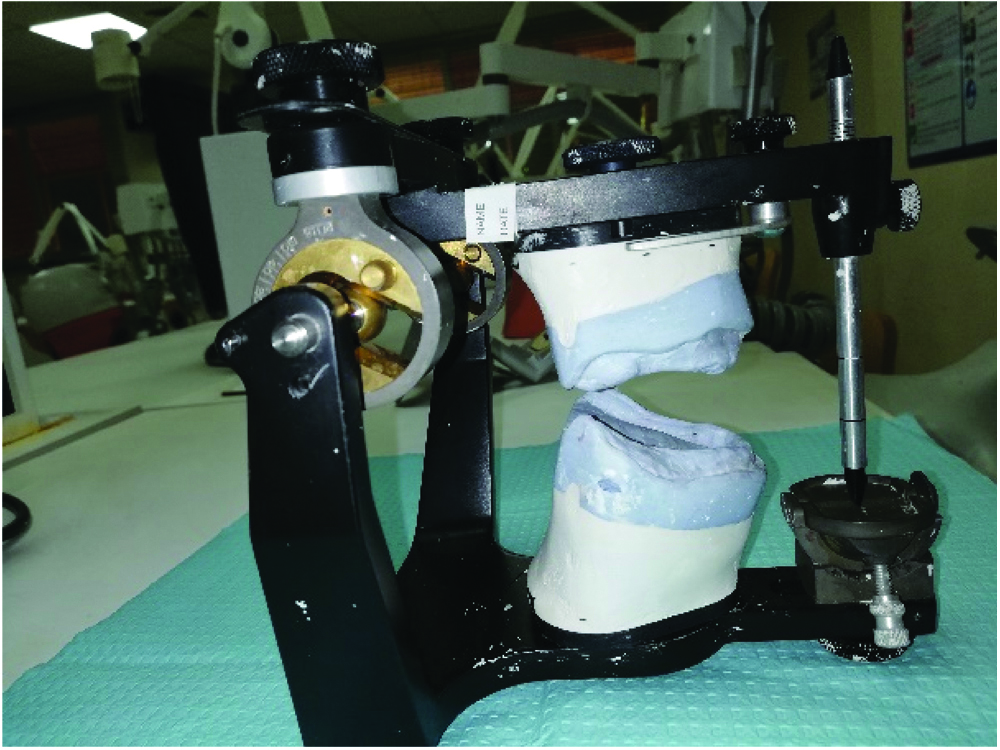
The patient was explained about the procedure and a written consent was obtained before the start of the procedure. Maxillary and mandibular primary impressions were made using alginate (Cavex CA37, Netherlands) and diagnostic casts were made. Acrylic (PMMA) custom trays were fabricated using these diagnostic casts. The custom trays were border molded using greenstick compound (DPI Pinnacle tracing sticks, India) and final impressions were made using an impression paste (Cavex Outline, Netherlands). The final casts were obtained from these impressions. Temporary record bases with wax rims were made on these master casts. Maxillomandibular relations were made using these record bases. Following this procedure the casts were articulated [Table/Fig-2] using the face bow and centric relation records onto a semi adjustable articulator (Hanau Wide-Vue, Whip mix). The record bases were then removed out of the articulator and the inter-ridge relations were evaluated visually [Table/Fig-3]. In the anterior region, the mandibular dental arch revealed a prognathic relation to the maxillary arch while in the posterior area; the lower ridge was more buccal in relation to the upper ridge. Tooth arrangement was done by following the normal principles in arrangement for mandibular prognathic cases. The anterior teeth were arranged in an edge to edge relation whereas a proper teeth arrangement was not possible in the posterior segment by the technician, as it was going too much into a cross bite relation [Table/Fig-4]. The technician was then instructed to remove one bicuspid from the upper arch and rearrange the posterior teeth in a cross arch set up (Interchange); that is to use the upper posterior teeth of each side onto the lower arch of the opposite side and vice versa. This led to a good and stable occlusion [Table/Fig-5]. The try-in was done and patient’s approval was taken [Table/Fig-6]. The dentures were processed [Table/Fig-7] and was inserted [Table/Fig-8]. The patient was comfortable and the routine post insertion instructions were given. A post insertion checkup was done after 24 hours, 72 hours, one week and one month. The patient was satisfied with his denture and no post insertion complaints were reported.
Articulated occlusion rims.
Articulated cast showing mandibular prognathic ridge relation.
Right and left side view of the arrangement showing inability to achieve a good stable occlusion due to wider mandibular arch.

Cross arch arrangement of teeth to achieve a stable occlusion.

Intra oral view of the trial denture.

Final processed dentures showing the cross arch arrangement of posterior teeth.

Right, left and frontal view of the inserted denture.

Discussion
Over the past few years, the frequency of edentulism has drastically declined [1,2]. But when compared with high-income population the trend of edentulism is still more in low and middle-income populations [2]. Therefore, a dentist can always have a completely edentulous patient in his day to day clinical practice. There are many situations where we get a completely edentulous patient with abnormal jaw relations. Mandibular prognathic case with a wide posterior arch is quite challenging to both the dentist and technician. The main trouble that would come across in such cases is the difficulty in arranging the artificial teeth. It is well known that, a good occlusion is one of the criteria in obtaining a stable denture [3]. LaVere AM et al., stated the biomechanical importance in placement of posterior teeth for prognathic patients [4].
This report highlights a case of mandibular prognathism with wide posterior arch, which was managed by cross arch setting method. Cross arch arrangement [5,6] is the technique, where the upper posterior and lower posterior teeth are interchanged with each other onto the opposite sides (contralateral sides). By doing so, the posterior teeth are arranged to a more favourable position (neutral zone) and thereby the chewing forces are directed more to the centre of the remaining residual alveolar ridge. These may be indicated to obtain a stable occlusion especially if the deviation of the arch is more in lateral magnitude. The limitations of this type of arrangement could be a possible cheek bite due to the loss of buccal overlap from the upper teeth. However, there was no problem in this case as we followed-up the case for two years. Another limitation could be a difficulty in arrangement if the arch is too wide than expected.
There are review reports [7-9] on arrangement of teeth and occlusal schemes in complete denture cases but literature on case reports on this type of arrangement in a complete denture patient is scarce. Tambe A et al., reported this type of arrangement in a case of Oral Sub Mucous Fibrosis (OSMF) [6]. Readers should also know that this type of arrangement can also be used in cases where there are no pathologies. There are many ways to treat a mandibular prognathic situation. Various technique [4,5,10] involves cross bite arrangement, removal of one bicuspid to adjust the space etc. However in this case, a posterior cross arch arrangement with removal of one bicuspid from upper arch was suitable for better management of occlusion.
Lopes JF et al., have recently published literature on orthognathic surgeries for correcting skeletal deformities in a completely edentulous patient with an open bite [11]. Such type of approach should be considered only if the deformities are severe and cannot be managed prosthodontically. Dai N et al., have reported using digital technologies while Kumar L et al., have used innovative functional chew in method to develop occlusion in complete denture cases [12,13]. However, using these technologies for a prognathic mandible with a wide posterior arch needs further documentations.
The method how the occlusion was managed for this patient has an importance here rather than the method how the complete denture was fabricated. The arrangement of artificial teeth is considered to be an art based upon the biomechanical factors [10]. Occlusion should be developed to function efficiently with the least trauma to supporting tissues whether in normal or abnormal jaw relations. Regardless of what technologies used to fabricate a denture or develop an occlusion, the basic fundamentals of teeth arrangement remains the same. Reports [14] till date haven’t revealed any superior form of tooth arrangement in a particular patient. Therefore, it is always important to know the various situations that may require a dentist to deviate from the normal principles of tooth arrangement.
Conclusion
This article highlights the rehabilitation of a completely edentulous mandibular prognathic patient with wide arch. The case was treated using a cross arch arrangement of artificial teeth. The patient was evaluated for satisfaction on retention and stability of denture and was found to be satisfied. The success of a complete denture not only lies in one factor, but also in many factors like retention, stability, support, aesthetics etc. Understanding the correlation between the factors and procedures done is mandatory by the dentist to construct a removable prosthesis. Therefore, a practitioner should always correlate the anatomy with the biomechanical factors involved in the success of a denture.
[1]. Peltzer K, Hewlett S, Yawson A, Moynihan P, Preet R, Wu F, Prevalence of loss of all teeth (Edentulism) and associated factors in older adults in China, Ghana, India, Mexico, Russia and South AfricaInt J Environ Res Public Health 2014 11(11):11308-24.10.3390/ijerph11111130825361046 [Google Scholar] [CrossRef] [PubMed]
[2]. Tyrovolas S, Koyanagi A, Panagiotakos D, Haro J, Kassebaum N, Chrepa V, Population prevalence of edentulism and its association with depression and self-rated healthSci Rep 2016 6:3708310.1038/srep3708327853193 [Google Scholar] [CrossRef] [PubMed]
[3]. Jacobson T, Krol A, A contemporary review of the factors involved in complete dentures. Part II: StabilityJ Prosthet Dent 1983 49(2):165-72.10.1016/0022-3913(83)90494-8 [Google Scholar] [CrossRef]
[4]. LaVere AM, Freda AL, Artificial tooth arrangement for prognathic patientsJ Prosthet Dent 1972 28(6):650-54.10.1016/0022-3913(72)90117-5 [Google Scholar] [CrossRef]
[5]. Goyal B, Bhargava K, Arrangement of artificial teeth in abnormal jaw relations: Mandibular protrusion and wider lower archJ Prosthet Dent 1974 32(4):458-61.10.1016/0022-3913(74)90359-X [Google Scholar] [CrossRef]
[6]. Tambe A, Patil S, Bhat S, Badadare M, Cross-arch arrangement in complete denture prosthesis to manage an edentulous patient with oral submucous fibrosis and abnormal jaw relationBMJ Case Rep 2014 2014:bcr201320306510.1136/bcr-2013-20306525239981 [Google Scholar] [CrossRef] [PubMed]
[7]. Farias-Neto A, Carreiro AF, Complete denture occlusion: an evidence-based approachJ Prosthodont 2013 22(2):94-97.10.1111/j.1532-849X.2012.00927.x22984917 [Google Scholar] [CrossRef] [PubMed]
[8]. Engelmeier RL, Phoenix RD, The development of lingualized occlusionJ Prosthodont 2017 Apr 19 doi: 10.1111/jopr.1262410.1111/jopr.1262428422342 [Google Scholar] [CrossRef] [PubMed]
[9]. Abduo J, Occlusal schemes for complete dentures: a systematic reviewInt J Prosthodont 2013 26(1):26-33.10.11607/ijp.316823342330 [Google Scholar] [CrossRef] [PubMed]
[10]. Zarb G, Hobkirk J, Eckert S, Jacob R, Prosthodontic treatment for edentulous patients: Complete denture and implant supported prostheses. 13ed.3251 2013 Riverport LaneElsevier Mosby [Google Scholar]
[11]. Lopes JF, Pinto JH, Lopes MM, Mazottini R, Soares S, Interrelationship between implant and orthognathic surgery for the rehabilitation of edentulous cleft palate patients: a case reportJ Appl Oral Sci 2015 23(2):224-29.10.1590/1678-77572014037126018315 [Google Scholar] [CrossRef] [PubMed]
[12]. Dai N, Yu X, Fan Q, Yuan F, Liu L, Sun Y, Complete denture tooth arrangement technology driven by a reconfigurable rulePLoS One 2018 13(6):e019825210.1371/journal.pone.019825229912886 [Google Scholar] [CrossRef] [PubMed]
[13]. Kumar L, Mattoo KA, Innovating functional chew in method to establish balanced occlusion in complete denture-a case reportAnn Int Med Den Res 2017 3(6):DE35-DE37.10.21276/aimdr.2017.3.6.DE9 [Google Scholar] [CrossRef]
[14]. Rangarajan V, Gajapathi B, Yogesh P, Ibrahim M, Kumar R, Karthik P, Concepts of occlusion in prosthodontics: A literature review, part IJ Indian Prosthodont Soc 2015 15(3):200-05.10.4103/0972-4052.16517226929513 [Google Scholar] [CrossRef] [PubMed]