Calcium silicate-based cements have been available for many years. These biomaterials have been used in various endodontic treatments and provide a tight barrier against the migration of microorganisms and stimulate tissue healing without causing inflammation. However, they show properties like biocompatibility, negligible neurotoxicity and cytotoxicity, bactericidal and fungicidal properties [1]. Postoperative discolouration of the calcium silicate-based cements has been commonly noticed.
Intrinsic tooth discolouration related to endodontic treatment results due to decomposition of necrotic pulp tissue, haemorrhage into the pulp chamber, endodontic medications and filling materials [2,3].
However, there are various drawbacks with the usage of MTA, mainly its potential for tooth discolouration, expensive, difficulty in handling properties mainly long setting time (140 minutes) [12] and difficulty in removal at the time of retreatment.
To overcome the short comings of White MTA, newer calcium silicate-based bioceramics EndoSequence Root Repair Material (ERRM) (Brasseler, Savannah, GA) has been introduced. It is an insoluble, radiopaque and aluminium-free material which requires the presence of water to set and harden. ERRM is premixed cement that is available as a paste, condensable putty composed of nanosphere particles. ERRM is composed of calcium silicates, zirconium oxide (ZrO2), tantalum oxide and calcium phosphate. In EndoSequence, the bismuth oxide is replaced by zirconium oxide. It has high radiopacity and alkaline pH that enables to have ideal working time (more than 30 minutes) and strength (70-90 MPa).
ENDOCEM-Zr (MARUCHI, Wonju, Korea) is a white, fast-setting, pozzolan-based MTA, with minimal discolouration and calcification. It mainly consists of oxides of calcium, silicon aluminum, magnesium and iron along with radio-opacifiers. Its physical properties comprise of improved aesthetics; excellent sealing property and biocompatibility; minimal discolouration, reduced calcification, augmented for partial pulpotomy of anterior teeth. They are proven to be substantially equivalent to ENDOCEM MTA. ENDOCEM sets quickly without the addition of a chemical accelerator because it contains small particle pozzolan cement. The difference between ENDOCEM MTA and ENDOCEM-Zr is that, radio-opacifier bismuth oxide (ENDOCEM MTA) is replaced by zirconium oxide (ENDOCEM-Zr). ENDOCEM-Zr has similar physical and biocompatible properties and demonstrates comparable performance specifications to ENDOCEM MTA. ENDOCEM did not affect the contacting dentin surface when compared to different types of MTA which causes discolouration with time [13].
Although manufacturers claim that this product does not cause discolouration either in-vivo or ex-vivo, study was mainly aimed to determine the discolouration among ERRM and Endocem-Zr as these two combinations have not been previously studied in a same study, although it is proven that newer root end filling material have shown minimal discolouration with time. Other studies showed that significant coronal tooth discolouration was caused by Triple Antibiotic paste, Grey and White MTA but not by recent root end filling materials like that of Biodentine, Endosequence Root Repair Material and Endosequence Fast setting [14].
There are two colour matching methods in dentistry: visual (conventional) and instrumental. However, visual shade matching is unreliable, inconsistent and considered highly subjective. Despite visual assessment the most commonly used in clinical practice, is based on subjective measurements using a visual colour scale to compare shades [15]. Most often used instruments are: tristimulus colorimeters, spectroradiometers, digital cameras and spectrophotometers [16]. The colour measurements in the present study were carried out using an X-Rite i1 Pro Spectrophotometer. It is a scientific standardised equipment which gives information about reflectance curve as a function of wavelengths in entire visible range and thus numerically specifies the perceived colour of an object. This can also avoid long experimental time period in detecting colour changes that are not even clinically observable by human eye. Therefore, standard CIELAB colour system was used to express the magnitude of colour and relative colour changes of all the specimens [17,18].
For this reason, it was decided to use spectrophotometric analysis for evaluating tooth discolouration in this study similar to previous studies [19-21]. A spectrophotometer can detect colour without the interference of any uncontrolled factors [18]. Visual spectrometry is the most widely used method of determining colour; it meets international standards, and it is compliant with ISO standards [22,23]. Spectrophotometer is the most reliable instrument in both, in-vitro and in-vivo circumstances [24]. It is also a colour measurement instrument with both reliability and accuracy values greater than 90% [3] and hence more reliable in contrary there are studies which gives no statistical significant difference between Vita shade key and spectrophotometric method [25]. In instrumental shade analysis, the objective is to attain the smallest delta E value possible which specifies the most accurate shade match. The delta E value provides the quantification of the shade variance between the selected shade and the one to be matched which means that it does not specify whether one shade is darker or lighter than another. Brightness is a significant element of colour and must be prioritised during shade selection.
In a study by Van der Burgt TP et al., skilled visual inspectors analysed the colour difference between samples [3]. It was a subjective technique of colour analysis which was susceptible to error primarily owing to the individual and environmental influences. In the present study, spectrophotometer was used to measure the colour at the different intervals as it is more accurate than conventional means. Spectrophotometric analysis is cost effective and less time consuming when compared to stereomicroscope and hence used in this particular study. Novelty of the study dictates the use of recent material which is available in market and testing its evaluation for discolouration in the aesthetic zone by using a simple device like that of spectrophotometer which is accurate, reliable.
The study was conducted keeping in mind that MTA showed discolouration with time but the newer materials showed minimal discolouration, although the rate of changes among these three experimental groups has not been previously studied. The purpose of this in-vitro study is to assess and compare coronal tooth discolouration by ProRoot MTA, ENDOCEM-Zr and EndoSequence Root Repair Material after three months follow-up.
Materials and Methods
An in-vitro study was conducted for a period of three months (August-October, 2017). A sample size of 40 intact extracted permanent central incisor teeth were taken for study. The study was conducted at Manipal Institute of Technology (MIT) after ethical clearance was obtained from scientific review board from Kasturba Hospital, Manipal under Institutional Ethical Committee (reg No. ECR/146/Inst/KA/2013/RR-16) IEC:646/2015.
Inclusion Criteria included teeth with straight roots and closed apex. Natural extracted maxillary central incisors with minimal inclination in horizontal and vertical plane in order to minimise incisal abrasion and incisal angle cracks.
Exclusion criteria included teeth with caries, fracture, resorption, cervical wear and discolouration. The external surface of all specimens were then cleaned ultrasonically and polished with a rubber cup and pumice for calculus and extrinsic stain removal. In time bound study sample size was determined based on convenient sampling method, a sample size of 10 was determined for each group. Forty human extracted central incisors teeth were collected and divided into three experimental groups and one control group with a sample size of 10 each in all the groups.
Experimental Group: divided into three groups:
Group 1: ProRoot MTA (n=10 groups)
Group 2: Endocem-Zr (n=10 groups)
Group 3: EndoSequence Root Repair material (n=10 group)
Control Group (n=10 group): No filling material
The teeth were sectioned horizontally 2 mm apical to the cementoenamel junction (diamond disk, kerr dental). The coronal pulp was chemo mechanically removed using barbed broach (Mani, Tokyo, Japan) and with size 20 K-file (Dentsply Maillefer, Tulsa, Okla), and irrigated with 2.5% sodium hypochlorite (NaOCl) (10 mL) (Dkm Enterprise, Gujurat) via retrograde access. Using a cylindrical diamond bur (Mani, Tokyo, Japan), (8 mm head length and 1.4 mm head size), a cavity was prepared that extended 4 mm from cementoenamel junction. The cavities were flushed with 10 mL sodium hypochlorite (2.5%) followed by 5 mL saline. Cavities in group 1 were filled with ProRoot White MTA (Dentsply, Tulsa, OK), whereas cavities in group 2 were filled with ENDOCEM-Zr (MARUCHI, WONJU, KOREA) and group 3 filled with EndoSequence Root Repair Material (Putty) (Brasseler, Savannah, GA).
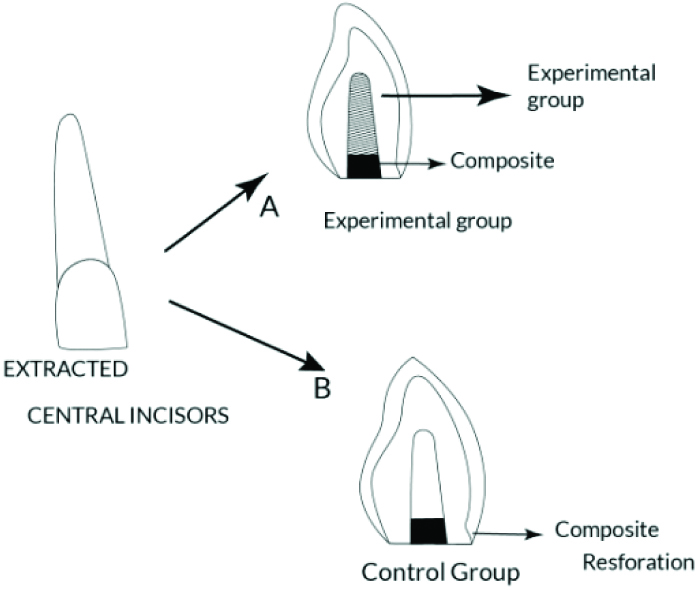
The materials were manipulated according to manufacturer’s instruction and then used to retrofill the teeth to the level of the cementoenamel junction in the pulp chamber. After the early setting phase, the lower area was sealed with light-cured hybrid composite resin (Ionosit-Baseliner; DMG, Hamburg, Germany). In the control group, the pulp tissue was removed from the teeth, which were then only sealed with composite resin [Table/Fig-1]. All samples were kept at room temperature at 100% relative humidity in artificial saliva under natural light. Tiny squares measuring 1.5×1.5 mm were prepared at the mid-buccal surface of all teeth by a fissure bur (Dentsply, Maillefer, Ballaigues, Switzerland) to be used as a reference for repeated measurements.
Shows diagrammatic representation of the procedure.
Measuring Tooth Colour Change
A spectrophotometer is made up of a spectrometer and a photometer. Spectrometer produces light of any wavelength whereas the function of photometer is to measure the intensity of light. The liquid or a sample is placed between spectrometer and photometer at the time of measurement. The photometer measures the amount of light that permits through the sample which is measured as voltage signal.
Colour assessments were done immediately for the experimental group and the control group after the placement of material in the cavity (baseline) and at one week (T1), one month (T2) and three months (T3). Colour values were recorded by a single operator using a spectrophotometer (X-Rite I1 Pro, Germany) [Table/Fig-2] having a standard illuminant with a white background to measure the colour of each specimen in a standardised condition according to the CIELAB [26].
Spectrophotometre: X-Rite I1 Pro, Germany.

Measurements were taken by positioning the spectrophotometer 2 mm from the samples under constant laboratory light conditions. The instrument was calibrated according to the manufacturer’s recommendations before recording the measurements for each group. Each sample was measured spectrophotometrically at 4 timepoints: At baseline and at one week, one month, three months after restoration. The colour measurements were reported by using the CIE L*a*b* System [26] [Commission International de I’EclairageL*a*b*].
L is the lightness (from 0 {black} to 100 {white});
a indicates red-green axis in the chromaticity parameter;
b indicates yellow blue axis in the chromaticity parameter.
ΔE describes the colour difference between the initial time
points (After placement) and each subsequent time point.
Measurements
To position the tip of the colorimeter in the same location on each specimen, a mould was prepared. The colorimeter was calibrated on white calibration plate according to the manufacturer’s instruction. The colour of the middle third of the teeth was assessed three times and the mean value was considered as the final measurement at the baseline examination. The teeth were then kept in an incubator 37°C in artificial saliva for three months, whereas artificial saliva was replenished each week. After this period, colour discolouration assessment was made using the colorimeter in the manner described for baseline readings.
ΔE={(ΔL*)2+(Δa*)2+(Δb*)2}1/2The human eye cannot perceive colour difference between two specimens (ΔE) values less than 1. ΔE values between 1 and 3.3 represent a clinically acceptable range [18]. ΔE values of 3.3 and higher are reported to be unacceptable for human eyes in clinical conditions [27].
Statistical Analysis
Statistical analysis was performed using SPSS software (SPSS version 15.0, SPSS, Chicago, IL, USA). Bonferroni Post-hoc tests were used to compare the rates of ΔE among the groups. One-way Anova and repeated measures analysis of variance was carried out to determine the significant difference in the discolouration among the four groups namely, ProRoot MTA, ENDOCEM-Zr, ERRM and Control group across the three time points: baseline, 30 days and 90 days.
Results
The results [Table/Fig-3,4,5 and 6] indicated that there is no statistically significant difference between the four groups. [Table/Fig-3] shows no statistical significant difference between baseline readings and various groups (p-value: 0.424). However, a statistically significant difference between control and ERRM at 30 days (p-value: 0.023).
Difference from baseline to seven days between the experimental group and control group.
| Variables | n | Mean | Std. Deviation | F value | p |
|---|
| Endosequence Root Repair Material | 10 | 1.2900 | 0.77810 | 0.956 | 0.424* |
| ProRoot | 10 | 1.1700 | 1.43066 |
| Endocem Zirconia | 10 | 0.8900 | 0.93506 |
| Control | 10 | 0.6000 | 0.66500 |
| Total | 40 | 0.9875 | 0.99439 |
At seven days, no significant difference between the groups (p=0.424*)
Difference from baseline to 30 days between the experimental group and control group.
| Variables | n | Mean | Std. Deviation | F | p-value |
|---|
| Endosequence Root Repair Material | 10 | 2.9500 | 1.84647 | 3.591 | 0.023* |
| ProRoot | 10 | 1.9900 | 1.97341 |
| Endocem Zirconia | 10 | 2.3500 | 1.38984 |
| Control | 10 | 0.7400 | 0.68183 |
| Total | 40 | 2.0075 | 1.70540 |
Multiple Comparisons between the experimental group and control group.
| Bonferroni |
|---|
| Variables | | Mean Difference | Std. Error | Sig. | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Endosequence Root Repair Material | ProRoot | 0.96000 | 0.69643 | 1.000 | -0.9844 | 2.9044 |
| Zr | 0.60000 | 0.69643 | 1.000 | -1.3444 | 2.5444 |
| Control | 2.21000* | 0.69643 | 0.018 | 0.2656 | 4.1544 |
| ProRoot | ERRM | -0.96000 | 0.69643 | 1.000 | -2.9044 | 0.9844 |
| Zr | -0.36000 | 0.69643 | 1.000 | -2.3044 | 1.5844 |
| Control | 1.25000 | 0.69643 | 0.486 | -0.6944 | 3.1944 |
| Endocem Zirconia | ERRM | -0.60000 | 0.69643 | 1.000 | -2.5444 | 1.3444 |
| ProRoot | 0.36000 | 0.69643 | 1.000 | -1.5844 | 2.3044 |
| Control | 1.61000 | 0.69643 | 0.160 | -0.3344 | 3.5544 |
| Control | ERRM | -2.21000* | 0.69643 | 0.018 | -4.1544 | -0.2656 |
| ProRoot | -1.25000 | 0.69643 | 0.486 | -3.1944 | 0.6944 |
| Zr | -1.61000 | 0.69643 | 0.160 | -3.5544 | 0.3344 |
Hence at 30 days, There is a significant difference between the control and Endosequence Root Repair Material (p=0.018)
Difference from baseline to 90 days between the experimental group and control group.
| Variables | n | Mean | Std. Deviation | F | p-value |
|---|
| Endosequence Root Repair Material | 10 | 1.5400 | 1.89982 | 0.572 | 0.637* |
| ProRoot | 10 | 1.9400 | 1.81365 |
| Endocem Zirconia | 10 | 1.4900 | 1.14159 |
| Control | 10 | 1.0400 | 1.13353 |
| Total | 40 | 1.5025 | 1.51446 |
At 7 days, no significant difference between the groups (p=0.637*)
Relevance was analysed with Bonferroni post-hoc test with a 95% confidence level within a group and in between groups. The level of statistically significant difference was accepted at p<0.05. [Table/Fig-6] shows no statistical significant difference between baseline readings and 90 days reading (p=0.637). It was found that a statistically significant difference exists between baseline and 30 days (p<0.001).
The overall change across different time points was statistically significant (p<0.001) for the four groups. The difference between (0-7 days) and (0-30) days was the statistically significant group (p<0.001) as shown in [Table/Fig-7].
Pairwise Comparisons across the different time point among experimental group and control group.
| Measure: MEASURE-1 |
|---|
| Time Interval | (In Days) | Mean Difference | Std. Error | Sig.b | 95% Confidence Interval for Differenceb |
|---|
| Lower Bound | Upper Bound |
|---|
| 0-7 days | 0-30 | -1.020* | 0.222 | 0.000 | -1.577 | -0.463 |
| 0-90 | -0.515 | 0.225 | 0.083 | -1.079 | 0.049 |
| 0-30 days | 0-7 | 1.020* | 0.222 | 0.000 | 0.463 | 1.577 |
| 0-90 | 0.505 | 0.221 | 0.086 | -0.051 | 1.061 |
| 0-90 days | 0-7 | 0.515 | 0.225 | 0.083 | -0.049 | 1.079 |
| 0-30 | -0.505 | 0.221 | 0.086 | -1.061 | 0.051 |
Based on estimated marginal means
*The mean difference is significant at the.05 level.
b) Adjustment for multiple comparisons: Bonferroni.
The overall change across different time points was statistically significant (p<0.001) for the 4 groups. The difference between (0-7 days) and (0-30) was the statistically significant group (p<0.001)
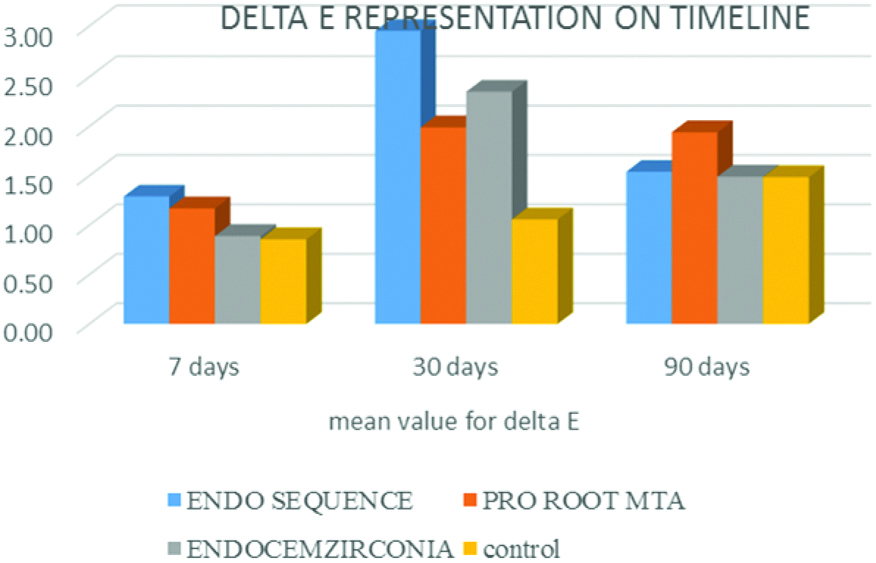
[Table/Fig-8,9] shows that ProRoot MTA have shown a steady increase in discolouration over 90 days time period, ENDOCEM-Zr have shown increase in discolouration from baseline to 30 days and decreases from 30 days to 90 days and EndoSequence Root Repair Material shows an increase in discolouration up to 30 days which gradually decreases from 30-90 days whereas control group over three different time periods shows slight changes in discolouration in three months’ time. [Table/Fig-8] shows the discolouration between the control and the test group which shows that maximum discolouration was attained up to 30 days and shows rebound effect over 90 days. ENDOCEM-Zr and EndoSequence Root repair material (ERRM Putty) shows reduced discolouration with time (90 days) with ENDOCEM-Zr showing reduced discolouration almost equal to that of control group after 90 days’ time period.
Mean value for delta E across different time intervals.
| Materials | Mean value for delta E |
|---|
| 7 days | 30 days | 90 days |
|---|
| ProRoot MTA | 1.17 | 1.99 | 1.94 |
| ENDOCEM-ZR | 0.89 | 2.35 | 1.49 |
| ERRM | 1.29 | 2.95 | 1.54 |
| Control | 0.86 | 1.06 | 1.49 |
Graphical representation of delta E values between experimental group and control group across different time intervals.
Discussion
The current study was conducted to analyse the discolouration of various calcium silicate cements that are indicated for pulpal treatment mainly in aesthetically important areas of jaw [28].
Most commonly accepted among theories of discolouration include that of oxidation of heavy metals (Iron or bismuth present in the cement). Discolouration mainly seen in white MTA is due to oxidation of iron content of the set material mainly calcium aluminoferrite phase of powder [1]. When bismuth oxide reacts with collagen it is converted to a black precipitate. It could also be due to bismuth oxide which gets oxidised and becomes unstable to release nascent oxygen. This nascent oxygen reacts with carbon dioxide in air and produces bismuth carbonate which could be one of the reasons for discolouration [29]. Bismuth oxide when exposed to high temperature or light irradiation in oxygen free environment undergoes dissociation to produce metallic bismuth and oxygen [26]. The main cause of discolouration could be due to those components of MTA which gets bound to phosphate ions or plasma proteins in the dentinal fluid. The chemical reaction between these components and their by-products gets oxidised [28] followed by transformation into pigmented product which could be reason for discolouration.
The chemical composition of Endocem-Zr is similar to that of ProRoot MTA mainly of oxides of silicates, calcium and aluminum and zirconium oxide as a radio-opacifier. It is a Pozzolan-based cement material which chemically reacts in the presence of water. On setting, reaction occurs between calcium hydroxide which is a by product with pozzolan cement. The smaller particle size of the Endocem increases the surface area and helps in greater contact with sterilised water (ease in manipulation). This increase in surface area increases the reactivity of calcium silicate particles to form calcium hydroxide [30] and calcium silicate hydrate phase.
ERRM is a newly developed calcium silicate-based bioceramic material. They are mainly composed of tricalcium silicate, dicalcium silicate, monobasic calcium phosphate, zirconium oxide, tantalum oxide, fillers and thickening agents. They have indications similar to MTA and according to manufacturers, ERRM do not cause tooth discolouration as the radio-opacifier bismuth oxide is replaced by zirconium oxide and tantalum oxide. Studies show that Calcium silicate-based cements exhibit discolouration when the following are simultaneously present: anaerobic conditions, irradiation with curing light [31] or a fluorescent lamp, and bismuth oxide.
Sodium hypochlorite is the most commonly used irrigants in endodontic treatment. Role of sodium hypochlorite on discolouration caused by silicate-based cement has been previously documented. It is been previously explained about the depth of penetration of sodium hypochlorite residues into dentin varying from a value of 77-300 μm which makes it difficult in the removal from the root canal. According to previous studies, discolouration that has been seen after irrigation with sodium hypochlorite followed by distilled water showed lesser discolouration compared to discolouration caused after irrigation with sodium hypochlorite [32].
Furthermore, studies have shown that blood in the pulp can deepen the discolouration which is seen in MTA and hence placement of materials is advised after establishing haemostasis or complete removal of pulp [33]. Previous studies have stated statistically significant difference in ProRoot MTA, Endocem versus control whereas no such difference was seen between Endocem and control group [34]. It has been shown that test materials like ProRoot MTA, ERRM putty in the presence of blood increases the discolouration of tooth. Application of dentin bonding agent before filling the pulp cavity with MTA prevents the component from penetrating the dentinal tubules. Other methods of reducing the discolouration include minimising the metal component of MTA which is responsible for its discolouration [35].
Colour determination with the spectrophotometer, was an advantage compared to conventional method, because it was easy to see different colours of each tooth, independent of lighting, clothing, makeup and eye-fatigue.
Human eyes observation gets determined by various factors like that of previous eye exposures on objects, illuminants position relative to observers colour characteristics, inability of individual to match colour, colour perception, also factors like metamerism plays important role. Even though, during the colour determination in these subjects, few disadvantages were detected.
In few cases, the machine was obviously incorrect relative to visual perception and the same match, and also the tip of the probe of the spectrophotometer does not cover the entire tooth surface. In the literature this is known as “loss edge”, and it was described by authors van der Burgt TP et al., [3].
Spectrophotometers, colorimeters and imaging systems are appropriate tools for tooth colour measurement and analysis and also for quality control of colour reproduction. Different measurement devices measure the complete tooth surface, providing either a “colour map” or an “average” colour of the limited area of about 3-5 mm on the tooth surface. Whenever possible, both instrumental and visual colour matching method should be used together as they complement each other and can lead towards predictable aesthetic outcome [36].
Spectrophotometric evaluation of ProRoot MTA has shown consistent increase in discolouration with time from baseline to 30 days and from 30-90 days. This is consistent with that of previously published studies where ProRoot MTA and White ProRoot MTA caused noticeable discolouration (DE about 3.3) as early as one day after the material was applied [7]. Kang SH et al., stated that MTA and MTA Angelus caused significant changes in tooth colour after 8, 12 and 16 weeks compared with the control group [29]. This could be mainly due to the presence of bismuth oxide which is used as a radio-opacifier in ProRoot MTA which has high staining potential and increase in tooth discolouration in the presence of sodium hypochlorite.
On evaluation of discolouration caused by teeth treated with ENDOCEM-Zr over 90 days has shown that increase in discolouration was seen from baseline to 30 days’ time period and steady decrease was seen from 30-90 days. This could be mainly due the presence of Zirconium oxide which is mainly used as a radio-opacifier replacing bismuth oxide. Similar results were seen in a study that compared discs of ProRoot MTA and MTA Angelus (Angelus, Londrina, PR, Brazil) which showed discolouration whereas RetroMTA (containing calcium zirconia complex), ENDOCEM-Zr (MARUCHI, Wonju, Korea) containing zirconium oxide and zirconium oxide powder were not associated with colour changes [29]. A significant change in colour was noticed when applying materials (PC) that contained bismuth oxide, but there was no change when applying materials that contained zirconium oxide [37].
Spectrophotometric evaluation revealed that discolouration of teeth treated with ERRM have shown increase in discolouration from baseline to 30 days’ time period and steady decrease was seen from 30-90 days. Biodentine and ERRM did not cause significant discolouration within 60 days after application compared with the control group [7]. Similar results of reduced discolouration were seen in a study where ERRM followed by Biodentine exhibited less discolouration over the 60 days period than ProRoot MTA and ProRootwMTA [7]. Other studies showed that significant coronal tooth discolouration was caused by Triple Antibiotic paste, Grey and White MTA but not by Biodentine, ERRM and Endosequence Fast setting [14].
However, these findings are inconsistent with a previous study that reported significantly greater colour change with ERRM than ProRoot MTA. The discrepancies may be related to slight variation in methodology [15]. The study conducted [38] used bovine teeth to evaluate the discolouration potential for experimental materials of biodentine and ERRM, and concluded with increase in discolouration with Biodentine and ERRM after a period of eight weeks compared to ProRoot MTA. Furthermore, their specimens were not exposed to light.
Spectrophotometric evaluation among the three test groups have shown that ERRM, ENDOCEM-Zr exhibited an increase in discolouration upto 30 days and steady decrease from 30-90 days when compared to that of ProRoot MTA. EndoSequence Root Repair and Endocem-Zr showed less discolouration compared to ProRoot MTA after three months follow-up despite its various advantages and hence, it should be cautiously used in aesthetic areas of the jaw. The evident increase in delta E value immediately after placement could be due to grayish colour of the material which later on diminishes with time. The rebound effect was more for ERRM when compared to that of ENDOCEM-Zr from 30-90 days. The results with control was statistically significant in case of ERRM (Group III) at time point of 30 days which showed a p-value 0.023 compared to other groups.
ProRoot MTA should be used with caution, especially in the aesthetic zone, and ERRM and Endocem-Zr may be used as an alternative material. There are various newer calcium silicate-based cements available in the market, the importance of its composition and its various modes of action in terms of discolouration gives us clinical-based evidence in usage of these materials in aesthetic zone.
Limitation
Short coming of the study includes the limited sample size. The study is conducted for a short time span of three months, long term follow-up as long as one year could be evaluated for better results of these materials. The study attempted to mimic clinical scenario ideal results, but the most ideal could have conducted in an in-vivo study. Other factors could have been included in the study like that of presence of blood would affect the final outcome of the study. Other factors which also includes the discolouration like that of blood, sodium hypochlorite which would influence the final outcome.
Conclusion
Within the limitations of the current in-vitro study, it is shown that ProRoot MTA exhibited increase in discolouration from baseline to 90 days. ENDOCEM-Zr and ERRM exhibited increase in discolouration from baseline to 30 days’ time period and steady decrease was seen from 30-90 days. Significant difference in discolouration was noted between baseline and 30 days’ time point in condition of ERRM followed by rebound effect in 90 days’ time period.
Keeping in mind the limitations, the current study has concluded that ENDOCEM-Zr and ERRM can used as an alternative to ProRoot MTA in the aesthetic zone which has shown to increased discolouration with time. Spectrophotometers and colorimeters represent a basic adjunct to visual tooth colour evaluations. Stereomicroscopy for measurements is also being considered for measuring tooth discolouration.
At seven days, no significant difference between the groups (p=0.424*)
Hence at 30 days, There is a significant difference between the control and Endosequence Root Repair Material (p=0.018)
At 7 days, no significant difference between the groups (p=0.637*)
Based on estimated marginal means
*The mean difference is significant at the.05 level.
b) Adjustment for multiple comparisons: Bonferroni.
The overall change across different time points was statistically significant (p<0.001) for the 4 groups. The difference between (0-7 days) and (0-30) was the statistically significant group (p<0.001)