A Case Report of Ureteral Triplication with Contralateral Duplication-A Rare Anomaly with Difficult Diagnosis and Treatment
Sandeep Gupta1, Ankit Vaishnav2, Dilip Kumar Pal3
1 Associate Professor, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
2 Post Doctoral Trainee, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
3 Professor and Head, Department of Urology, Institute of Postgraduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Professor and Head, Department of Urology, Institute of Postgraduate Medical Education and Research, 244, AJC Bose Road, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com
Ureteral triplication is a rare congenital anomaly of the urinary tract with around 100 reported cases in English literature. Rarer is the presence of bilateral ectopic ureter with it. Here, a case of a young female patient who presented with continuous incontinence and right loin pain is reported. On thorough investigation she was found to have trifurcate right renal pelvis with right triple ureter forming single dilated right lower ureter, which was opening ectopically into vaginal vault; associated with hydronephrosis on right side. There was duplex moiety of left kidney with hydronephrosis of upper moiety with ectopic opening of upper ureter into vaginal vault. She was treated with laparoscopic right ureteric reimplantation with successful recovery. Multifarious presentations sometimes make it difficult to identify clinically and diagnose on imaging findings. The presentation of ureteral triplication and the features on diagnostic modalities like ureteroscopy, retrograde pyelography and magnetic resonance urography are hereby discussed with review of literature.
Hydronephrosis, Magnetic resonance urography, Retrograde pyelography, Wolffian ducts
Case Report
A 22-year-old female presented to us with complaints of continuous urinary incontinence since birth and pain and dysuria from last one year. She had been visiting near by health care facilities for the same complaint and been managed conservatively for her symptoms.
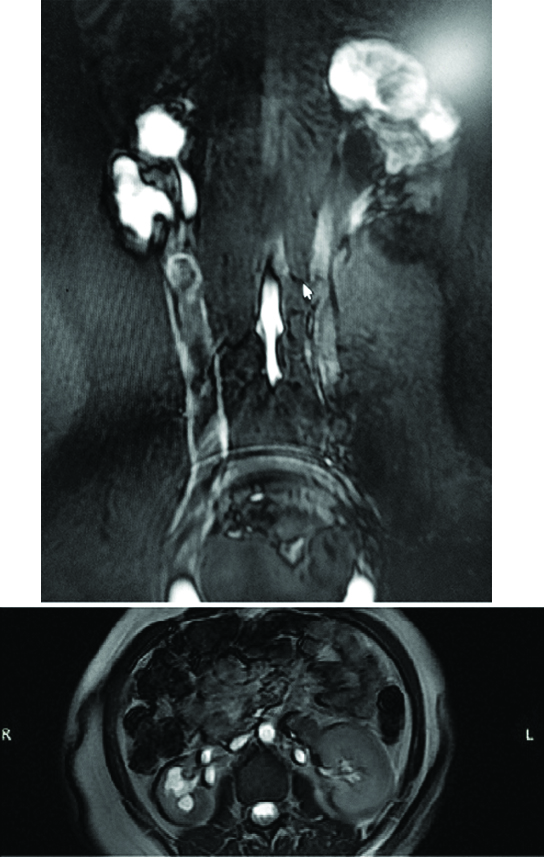
A systemic examination was done which was unremarkable. Urinalysis and a complete blood count were essentially normal. An ultrasound showed bilateral duplex moiety with bilateral hydronephrosis and right ureter was dilated. Computed Tomography (CT) scan showed triple calyceal system with hydronephrosis on right side. The three ureters joined at upper part at L3 level, forming a dilated common ureter which drains below bladder neck along with complete duplication on left side with gross hydronephrosis of upper moiety. The upper moiety ureter was ectopic draining below bladder neck and lower moiety ureter was normally opening at trigone. Magnetic Resonance Urography (MRU) was suggestive of trifurcate right renal pelvis with dilated right ureter opening ectopically into vaginal vault. Duplex moiety of left kidney with hydronephrosis of upper moiety with ectopic opening of upper ureter into vaginal vault [Table/Fig-1].
Magnetic resonence urogram-showing right side triple ureter.
Diethylenetriaminepentaacetic Acid (DTPA) Renogram showed normal function in right kidney and left lower moiety, non-functional left upper moiety. The left upper moiety hydronephrosis was mainly due to obstruction at the ectopic opening of the upper moiety ureter, which might be functioning normally earlier, as apprehended by her incontinence episodes, followed by cessation of function due to long term obstruction and parenchymal damage. Although no past imaging records were available. We proceeded further with cystoscopy with vaginoscopy which showed single right ureter opening at vaginal vault and single left ureteric opening at trigone. Ureteroscopy and retrograde pyelography on the right side showed triple ureter joining to form a single lower ureter [Table/Fig-2]. Left ectopic ureter opening could not be localised on cystourethroscopy. It was concluded that this case was likely to be a Smith Type-3 triplication on right side and complete duplication with ectopic upper ureter on left side [1].
Right ureteroscopy-luminal openings of right triple ureters seen forming a single lower ureter.

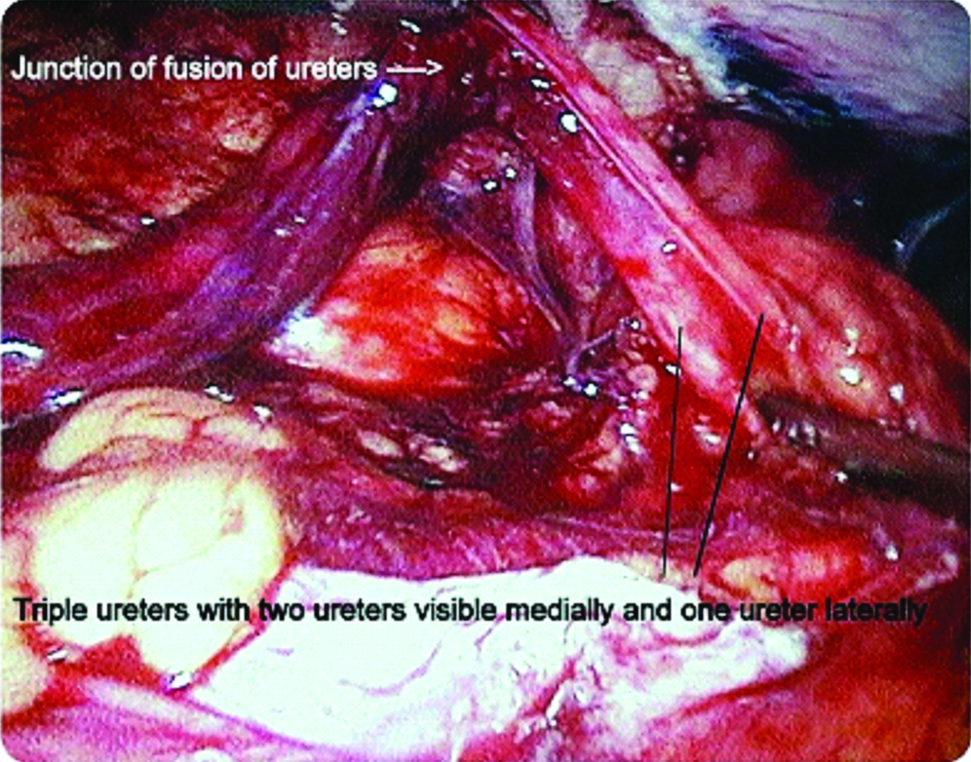
As the patient was symptomatic on right side, we decided to perform laparoscopic right ureteric reimplantation [Table/Fig-3]. The post-operative period was uneventful. The patient was discharged on post-operative day seven after removal of drain and per urethral catheter.
Laparoscopic view of right triple ureters joining to form a single ureter.
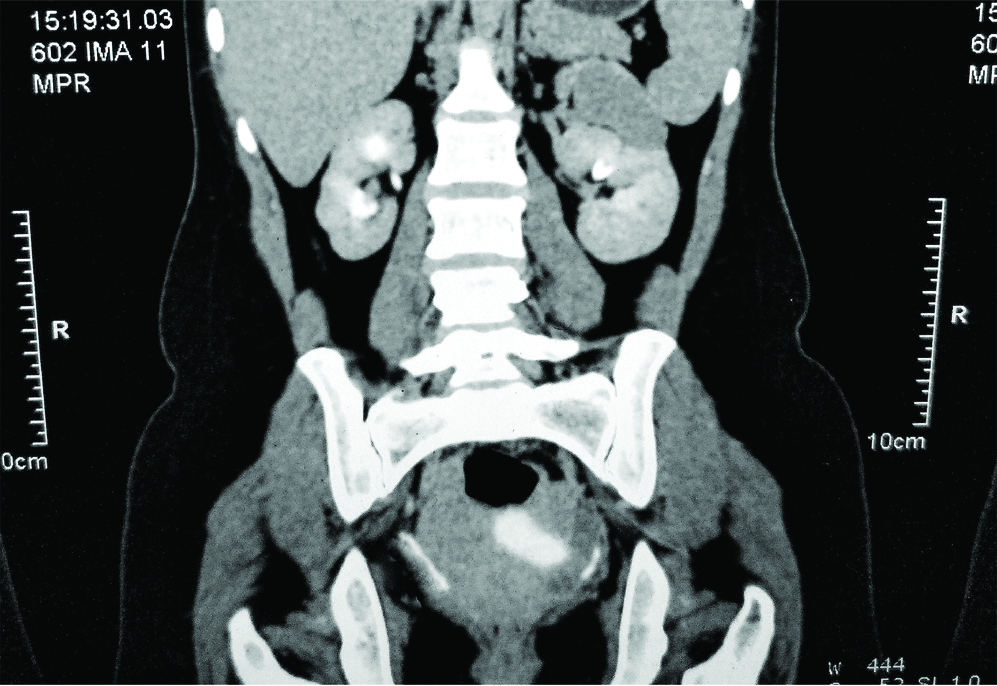
On follow-up, the patient was doing well. Patient was continent even at one year. The follow-up CT scan showed resolution of Hydronephrosis (HDN) on right side to mild degree with persistent hydronephrosis on left side, without any emergence of symptoms on that side [Table/Fig-4].
Postoperative CT images on follow-up-decreased hydronephrosis on right side.
Discussion
Triplication of the ureter is an extremely rare congenital anomaly first described by Wrany in 1870 [1], and subsequently first reported in the literature by Lau and Henline in 1931 [1]. Triplication of the ureter can be bilateral or unilateral with female predominance [2]. Ureteral triplication might occur from the presence of three ureteral buds that arise independently from the Wolffian duct or early fusion of one of the buds. In 1946, Smith presented a simple classification of triplicate ureter, which is still in use today [Table/Fig-5] [3]. In duplex system, two ureters that empty separately into the bladder follow the Weigert-Meyer law, the ureter from the upper pole usually inserts more medially and inferiorly than the ureter from the lower pole which drains superiorly into the bladder. This was evident in our case with the left side complete duplex system. In triplication, this principle does not apply uniformly [4,5]. Ureteral triplication is mainly diagnosed incidentally during radiological examinations. This perhaps explains the wide range of age of 1-74 years at presentation in the literature [6,7]. Clinical signs of triplication are non-specific. They consist of abdominal or back pain, haematuria, fever and urine storage and voiding symptoms [8].
Smith classification of triplication of ureter.
| Type | Smith classification |
|---|
| 1 | Triple ureters, (Complete triplication) Three separate ureters and three separate ureteral orifices in bladder, urethra or ectopic location (35%) |
| 2 | Incomplete triplication: Three ureters arise from the kidney, two join on the way to the bladder and two orifices present in the bladder (21%) |
| 3 | Trifid ureter: All three ureters unite and drain through a single orifice (31%) |
| 4 | Two ureters from the kidney: One divides into two to have three draining orifices (9%) |
In our case, the major symptom was continuous incontinence, pain and dysuria. Triplication may be associated with urinary tract calculi, infection, obstruction, reflux and recurrent acute epididymitis [9].
Diagnostic tools include ultrasonography, intravenous pyelography, CT urography, retrograde pyelography, Magnetic Resonance Urography (MRU) and cystoscopy. MRU is an emerging technique, which provides a non-invasive visualisation of the urinary tract with high-quality images and in multiple projections without the use of ionising radiation. With the use of diuretic and contrast media, MRU can provide excretory functional information of the kidney as well as the morphological information, the level of fusion is also better visualised and the type of triplication is easily determined [10].
Triplication of ureter may have varied clinical presentation and management depends on the symptomatology and investigative findings. Our case presented with obstructive features on the right side and managed with laparoscopic ureteric reimplantation. As patient was asymptomatic on left side, no surgical intervention was done on that side.
Conclusion
Ureteral triplication is a very rare condition. Clinical signs of triplication are non-specific, and duplication and triplication are often incidental findings on investigation. In the case of a female child, enuresis can occur with ectopic ureteric orifice. A large battery of tests and imaging studies may be needed to diagnose and classify the disease accurately. The diagnosis of triplication is important to avoid complications and progressive renal damage. In our case, accurate diagnosis and timely intervention lead to prevention of any further kidney damage on the affected side.
[1]. Smith I, Triplicate ureterBritish Journal of Surgery 1946 34(134):182-85.10.1002/bjs.1800341340920278127 [Google Scholar] [CrossRef] [PubMed]
[2]. Sánchez-de-Badajoz E, Ramos J, Burgos R, Ureteral Triplication with Contralateral Ureter DuplicationUrologia Internationalis 1992 48(2):217-18.10.1159/0002823361585519 [Google Scholar] [CrossRef] [PubMed]
[3]. Spangler E, Complete Triplication of the UreterRadiology 1963 80(5):795-97.10.1148/80.5.79513978511 [Google Scholar] [CrossRef] [PubMed]
[4]. Bhattacharyya S, Basu K, Samanta N, Unilateral ureteral triplication with duplex kidney and megaureterJournal of Indian Association of Pediatric Surgeons 2005 10(2):10810.4103/0971-9261.16475 [Google Scholar] [CrossRef]
[5]. Fernbach S, Poznanski A, Pediatric case of the day. Complete ureteral triplicationRadioGraphics 1989 9(2):359-60.10.1148/radiographics.9.2.29285762928576 [Google Scholar] [CrossRef] [PubMed]
[6]. Verdú F, Moneada , Diez Cordero J, Herranz F, Pardo E, Triplicidad ureteralActas Urol Esp 1990 14:452-54. [Google Scholar]
[7]. Ali SN, Ali AN, Ahmad N, Ali MN, Ureteral triplication and contralateral duplication with vesicoureteral refluxJournal of Ayub Medical College, Abbottabad: JAMC 2014 26(2):258-60. [Google Scholar]
[8]. Villanueva Peña A, De Diego Rodríguez E, Triplicid ureteral. una inusual presentación aisladaActas Urológicas Españolas 2004 28(10):766-70.10.1016/S0210-4806(04)73179-4 [Google Scholar] [CrossRef]
[9]. Soyklemez H, Koplay M, Altunoduk B, Oguz F, Ureteral triplication and contralateral duplication with vesicuoureteral reflexBalkan Med J 2011 28:469-70.10.5174/tutfd.2010.04021.2 [Google Scholar] [CrossRef]
[10]. Kocaoğlu M, Turan Ilıca A, Bulakbaşı N, Ergin A, Üstünsöz B, Sanal T, MR urography in pediatric uropathies with dilated urinary tractsDiagn Interv Radiol 2005 11:225-35. [Google Scholar]