Aesthetic dentistry has transformed into a solution to routine hassles in dental practise concerning patient’s demand for natural appearance of restoration. Improvements in ceramic systems and resin cements have provided aesthetically successful treatments in the anterior region to correct discolourations and unaesthetic tooth forms. Porcelain fused metal restoration proved beneficial in this field but the metal coping impaired the light transmission creating shadows in the joints. For many years, all ceramic restorations has been a predictable and durable option in aesthetic correction except for the substantial removal of sound tooth structure. Porcelain laminate veneers which are more conservative has extensively contributed to the popularity of aesthetic dentistry in the past twenty years [1].
Porcelain veneers have been evolving as a reliable option for both patients and clinicians seeking superior aesthetics [2]. These restorations are preferred due to their minimally invasive tooth preparation when compared with existing treatment options [3]. Long term clinical success of laminate veneers is determined by marginal adaptation of the veneer restoration, design of preparation, functional and morphological condition of the abutment tooth. The colour of the underlying tooth structure or restorative foundation material, shade and thickness of the resin luting cement used and ceramic material selected widely attribute to the superior optical properties, biocompatibility, increased translucency and exceptional aesthetic outcome of the final restoration [4-7].
Resin luting cements, considered as active-type cements, have rising applications in the cementation of fixed prostheses, as they exhibit improved mechanical and adhesive properties when compared with other conventional luting cements. Furthermore, they offer acceptable stability and better fracture resistance of porcelain laminate veneer, in combination with a satisfactory aesthetic outcome. Currently, resin luting cements are available in various shades to improve final colour match with the adjacent natural tooth and to allow the clinicians to select the accurate cement shade to gain desirable aesthetic enhancement of laminate veneer restoration [3,5]. However, research and investigations emphasising the impact of cement shades on the final colour of ceramic restorations remains limited and the effect of resin cement thickness remains controversial.
Hence, the purpose of this scoping review was to analyse whether the shade and thickness of resin cement will affect the final colour of the porcelain in the in-vitro studies as a very minimal focus was emphasised in this area of interest.
Materials and Methods
Information Sources and Search Strategy
An electronic database search was conducted in Cochrane, MEDLINE and PubMed via Ovid for articles published in English between 1990 and 2017. To identify the studies to be considered, search strategy was developed for each database. Additional hand search of literature for bibliographies in the chosen articles was done using Google Scholar. The subject search based on the search strategy used specific keywords and their combinations in MEDLINE [Table/Fig-1]. The Mesh terms used were Dental veneers, porcelain laminate veneers, cement thickness, cement shade, cement colour, Prosthesis Colouring and Prosthesis shade.
| #1 exp Dental Veneers/or porcelain laminate veneers.mp. |
| #2 (cement adj3 thickness).mp. |
| #3 1 and 2 |
| #4 (shade adj3 cement).mp. |
| #5 2 or 4 |
| #6 1 and 5 |
| #7 exp Colour/or color.mp. |
| #8 exp Colour/or color.mp. |
| #9 6 and 8 |
| #10 exp Prosthesis Colouring/or shade.mp. |
| #11 7 or 10 |
| #12 6 and 11 |
| #13 1 and 4 |
| #14 3 or 12 or 13 |
Study Eligibity Criteria
Studies which satisfied the following inclusion criteria and those published in English language were only considered for review:
Preclinical studies
Studies evaluating the effect of shade of resin cement on the final colour or aesthetics of the porcelain laminate veneers
Studies evaluating the effect of thickness of resin cement on the final colour or aesthetics of the porcelain laminate veneer.
Studies which used a standard measurement system for evaluation of colour change.
Clinical trials were excluded as they used subjective method of evaluation like patient and operator satisfaction and not a standard objective method to evaluate the final shade which was one of the inclusion criteria.
Study Selection
A two stage reviewing process was undertaken. In the initial stage, titles and abstracts identified through the search were scanned and in the second stage full report of studies which met with the inclusion criteria were screened independently by two reviewers. A third reviewer resolved the disagreements and conflicts. This systematic review was conducted and presented in accordance with Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines [8].
Data Extraction
Data and information from the included studies were extracted using a specially designed data extraction form. The following data was recorded: author, country, year of publication, study design, study type, sample preparation, intervention which include type of resin cement, parameters evaluated, outcome reported based on colour change of porcelain laminate veneers and the mode of outcome measurement, the equipment used to measure colour change.
Results
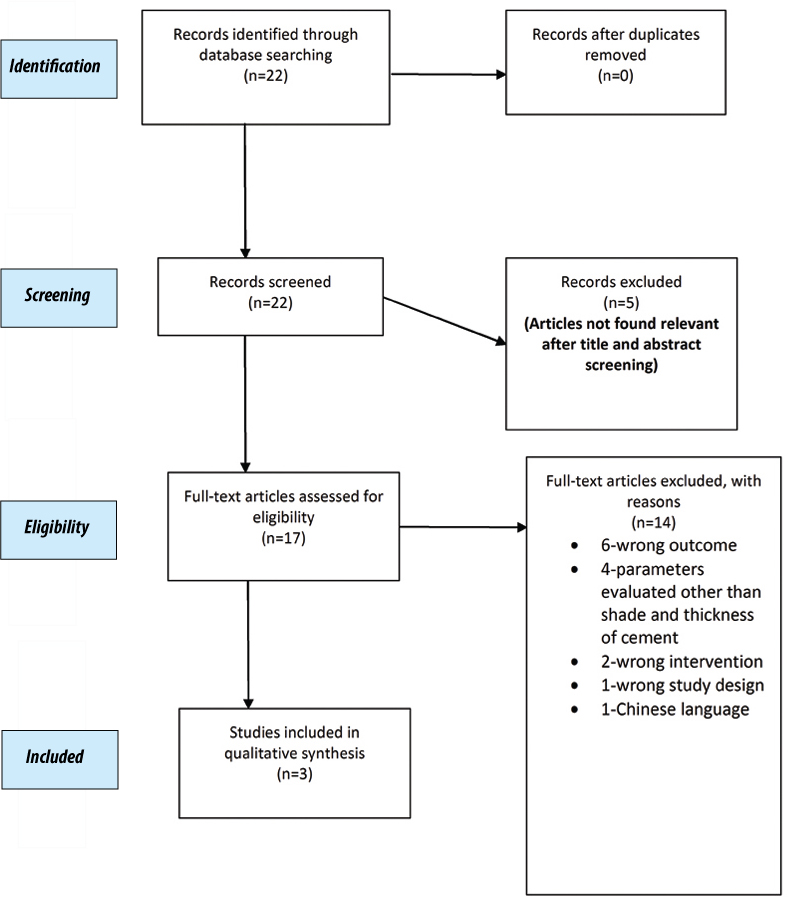
Following the initial search of literature, 22 studies were identified through primary database searching. As there were no duplicate references to be removed; all the studies underwent a thorough title and abstract screening. Five articles were excluded after resolving the disagreements. This yielded a total of 17 articles for full text reading. After an in depth assessment of these studies, 3 articles fully satisfying the inclusion criteria were accepted as eligible for the scoping review and the remaining 14 articles were eliminated for definite reasons which are presented in detail in the study inclusion flowchart below [Table/Fig-2] [9-11].
Study inclusion flowchart.
Description of Included Studies
All the three studies reported in this scoping review were in-vitro type and had comparative study design. [Table/Fig-3] summarises the characteristics of the included studies in detail.
Detailed summary of the included studies.
| Type of study | Shade of porcelain Ingot/disc | Type of resin cement | Parameters evaluated | Measurement system | Outcome colour difference(ΔE) |
|---|
| Shade | thickness |
|---|
| Hernandes et al., [11] | In vitro study | A2 shade (IPS e.max press) High translucence (HT) Low translucency (LT) 1 mm | Light activated Resin cement | A1 and A3 Variolink II, Ivoclar vivadent | 100 μm (control) | CIEL*a*b* system using reflectance spectrophotometer | ΔE values showed statistically significant difference for cement shade (p<0.0001) ΔE value for HT ceramics were significantly higher than LT ceramic regardless of RC shade |
| Kürklü D et al., [9] | In vitro study | A1 shade 0.5 mm and 1.0 mm | Light activated Resin cement | Clearfil EX Chroma (CA) Clear (CR) Opaque white (O) | 0.2 mm (control) | CIEL*a*b* and CIEDE2000 system using non contact spectroradiometer Relative translucency parameter (RTP) | The colour differences between the tested porcelain/cement combinations were only clinically acceptable when the Clear cement shade (CR) was applied (mean ΔEab=2:71 and mean ΔE00=2.06)The mean RTP with the Clear (CR) and Chroma (CA) cement shades were greater than that of the Opaque white (O) cement shade for each thickness (p<0.001). |
| Turgut S et al., [10] | In vitro study | A1, A3, EO, and ET shades of IPS Empress 0.5 mm and 1 mm | Dual-polymerizable resin cement Light polymerizable resin cement | Relyx X veneer(A1, A3, Tr, WO)Variolink veneers (+3, MO, -3.)Maxcem Elite(Clear, WO, Yellow, white)Variolink II (Tr, WO) | 0.1 mm | CIEL*a*b* Colorimeter | The highest colour change was shown when Variolink Veneer-3 cement used with ET ceramic combination, irrespective of the porcelain thickness.(ΔE=9.8 in 0.5 mm and ΔE=6.0 in 1 mm)The lowest colour change was shown when RelyX Veneer Tr and Variolink II Tr used with EO ceramic in 0.5 mm (ΔE=0.9) and 1 mm (ΔE=0.6) porcelain thickness respectively. |
*HT (High Translucence); *LT (Low Translucence); *CIEL (International Commission On Illumination);* RC (Resin Cement) *CA (Chroma); *CR (Clear); *O (Opaque White); *RTP (Relative Translucency Parameter); *EO (Opaque); *ET (Translucent)
Kürklü D et al., conducted an in-vitro study on effect of cement shade on colour and translucency of porcelain veneering materials [9]. Authors compared three different shades of light activated resin cement; Chroma (CA), Clear (CR) and Opaque white (O) on porcelain disc of thickness 0.5 mm and 1 mm. A standard of 0.2 mm resin cement thickness was applied. Colour difference was measured with non-contact spectral radiance measuring system and assessed in terms of perceptibility and acceptability using Commission Internationale de l’Eclaige (CIE) L*a*bΔ*(ΔE*ab) and CIEDE2000 (ΔE00) colour difference formula on grey background. The results showed significant colour difference intervals (ΔE00) between dissimilar shades of resin cement beyond clinical acceptability and perceptibility threshold regardless of porcelain thickness.
Among the porcelain/cement combinations in A1 shade porcelain thickness .5 mm and 1 mm using, only Clear shade (CR) presented mean colour difference below clinically acceptable threshold (ΔE*ab=2.71 and ΔE00=2.06). The thickness of cement calculated by subtracting the thickness of porcelain disc before and after cementation reported no significant effect on mean cement thickness (p>0.291). Relative Translucency Parameter (RTP) values were also assessed with TPCIELAB formula over black and white background. There was an increase in relative translucency when the porcelain thickness was reduced from 1 mm to .5 mm. Chrome (CA) and Clear (CR) cements showed significantly high translucency when compared to Opaque (O) (p<0.001).
Turgut S et al., performed another invitro study on effect of resin cement on final colour of laminate veneers [10]. Specimens were fabricated with A1, A3, EO (opaque) and ET (translucent) shades of IPS Empress Aesthetic, in 0.5 mm and 1 mm thicknesses. A total of 13 shades - Two dual polymerizable and two light polymerizable resin cement system from different manufacturer were selected for cementation. For Rely X Veneer and Maxcem Elite cement systems; porcelain ingot shades A1, A3, opaque and translucent shades were chosen. Highest (+3), medium (0), and low (3) shades were used for opaque and translucent Variolink II resin cement system. Colourimeter was the measuring tool used and colour difference (ΔE) was calculated using CIEL*a*b*system. The highest colour change was shown when Variolink Veneer-3 cement used with ET ceramic combination, irrespective of the porcelain thickness. The lowest colour change was shown when RelyX Veneer Tr and Variolink II Tr used with EO ceramic in 0.5 mm and 1 mm porcelain thickness respectively. 1 mm EO shade ceramics were least influenced by resin cements when compared to other shades whereas a visually unacceptable colour change was reported by RelyX Veneer A3 and Variolink Veneer-3 resin cements in .5 mm thick ceramic disc.
An in-vitro study reported by Hernandes DKL et al., evaluated the effect of two different shade of resin cement (A1 and A3) layer on colour difference (ΔE), translucency parameter (TP) and chroma of low (LT) and high (HT) translucent reinforced lithium disilicate ceramic laminates of A2 shade of 1 mm thickness [11]. The thickness of the resin cement applied was standardized as 100 μm in all the specimens. Regardless of resin cement shade, the results showed significantly higher colour difference, higher translucency and lower chroma in HT ceramics than LT ceramics. Despite ceramic translucency, A3 shade resin cement promoted higher colour difference than A1 shade when luted to ceramic disc. When comparing Translucency Parameter of ceramic discs with A1 and A3 shade cement, no significant difference was observed whereas higher chroma value was noted in A3 shade resin cement. Ceramic with underlying resin cement presented low translucency than disc without resin cement.
Discussion
Porcelain laminate veneers has evolved as a desirable treatment option primarily because of its excellent aesthetic outcome in terms of colour stability, translucency, optical properties similar to natural tooth and minimally invasive tooth preparation. The external factors that influence the final colour of the laminates are shade of the underlying tooth, resin cement used for cementation and ceramic material selected. Shade and thickness of underlying resin cement contribute to enhancement of the final outcome of restoration. The present scoping review aims to evaluate the effect of shade and thickness of resin cement on the final colour of laminate veneers.
Shade and Thickness of Procelain Core
The shade of porcelain disks used in the studies were mostly of lighter shades like A1 and A2 as its translucency enable the evaluation of effect of various resin cement shades in particular [9]. Turgut S et al., used four porcelain shades (A1, A3, EO and ET) where the highest colour change was observed in ET (translucent) ceramic-cement combination irrespective of porcelain thickness and lowest colour change in EO (Opaque) ceramic-cement combination [10]. Hernandes DKL et al., stated that high translucency (HT) ceramics present significant colour difference and more translucency than LT ceramics [11]. This results favoured the previous studies which reported that the core shade influences the final colour of translucent porcelain than opaque shade porcelain [12-15].
When compared to crown restorations, a minimally invasive and more conservative preparation is expected for porcelain laminate veneers. Some of the previous studies have reported the ideal thickness of porcelain laminate veneers to range between 0.3 mm and 1.5 mm, where as some authors stated a ceramic thickness range of 0.5-1 mm [16-20].
Among the included studies [13,21], of this review, two authors compared the effect of two different ceramic thickness on the final shade of laminate veneers [9,10]. According to Turgut S et al., greatest colour difference was observed when 0.5 mm thick ET ceramic was used and the least colour difference was exhibited in 1 mm EO ceramics [10]. Difference on evaluation of ceramic shade effect on the final colour of restoration, 1 mm thick veneer showed no clinically perceptible colour change whereas 0.5 mm presented colour change beyond acceptable perceptibility. According to Kürklü D et al., change in colour of final restoration was with in acceptability threshold in ceramic thickness 0.5 mm and 1 mm when Clear Shade resin cement was used [9]. Whereas variation in ceramic thickness showed clinically unacceptable result when chromatic and opaque shade were applied. Author of the forementioned study also emphasised that the relative translucency of the final restoration significantly increased when porcelain thickness reduced.
Shade of Underlying Resin Cements
Among the three studies discussed in this review, two studies used light activated resin cements [9,11], whereas one study has mentioned the use of both light polymerizable and dual polymerizable resin cements systems [10]. The brand of resin cements evaluated in the three comparative studies varied resulting in heterogeneity among the studies. Even though two studies used Variolink II resin cement in common, the shade selected by each study varied. Hernandes DKL et al., preferred A1 and A3 shades of Variolink II, whereas Turgut S et al compared Translucent (Tr) and White Opaque (WO) shades [11].
Thickness of Underlying Resin Cements
The results of this review studies strongly emphasises the fact that there is a major scarcity of literature to confirm the effect of cement thickness on the shade of final restoration. Among the various interactions of elements that contribute to colour of the ceramic veneer restoration, thickness of the underlying cement also adds to the ultimate result. From the previous authors who reported on cement thickness, a range of 0.1 mm-0.2 mm thickness has been considered acceptable [22]. In this review, studies by Turgut S et al., and Hernandes DKL et al., adjusted the cement layer to a standard of 0.1 mm [10,11]. Kürklü D et al., maintained the thickness in 0.2 mm range which was calculated by subtracting thickness value of ceramic disc before and after cementation [9]. There was no significant effect noticed on mean cement thickness.
Effect on Final Colour in Laminate Veneers
Colour difference represented as ΔE was measured using spectroradiometer which provide with the reflectance standard. The effect of change in cement shade and porcelain thickness were calculated using colour difference formulas (CIE)L*a*b*(ΔE*ab) and CIEDE2000 which were then assessed in terms of perceptibility and acceptability [23]. Ghinea R et al., in 2010 has set the clinical acceptability threshold at 3.46 ΔE*ab and 2.25ΔE00 units and perceptibility threshold at 1.80ΔE*ab and 1.30ΔE00units [24].
This scoping review supports the capability of luting resin cements to mask the underlying tooth shade. Chang J et al., has emphasized that there has been no standardized resin cement shade classification published till date [25]. According to Hernandes DKL et al., A3 shade resin cement showed a significant colour difference in the final restoration than A1 shade when used on A2 shade ceramic disk [11]. Turgut S et al., reported that all the resin cement shades had influence on the ultimate shade of laminates and the effect of each shade also varied based on ceramic shade and thickness [10]. The colour change was noted to be beyond the standard perceptibility threshold of 3.5ΔE units. Comparative study by Kürklü D et al., reported that variation within the resin cement shades clear, chromatic and opaque exhibited a colour change in the final restoration which was within the clinical acceptability level [9].
Limitation
The main limitation of this review is that the body of evidence is very low to explain the actual effect of cement thickness on the final colour of veneers. The patient and clinician acceptability level could not be assessed as the studies included were in-vitro studies, definite type of porcelain material was considered and limited resin cement brands evaluated. Following the detailed full text screening, 14 articles were excluded due to various reasons. The most common reasons for exclusion were the studies which reported evaluation of parameters other than shade and thickness of the cement and other reported outcomes such as material properties and fatigue resistance of final restoration because these studies did not contribute to the review and some important results may be missing. Meta analysis was not attempted as the included studies showed heterogeneity. Further research is required to establish a standardised resin cement shade classification.
Conclusion
There is an imperative need for further investigations in this field to extract detailed information regarding the effect of shade and thickness of resin cement on the final colour of veneer restoration to arrive at a definite conclusion. Considering the limitations of this scoping review, it can be interpreted that the aesthetic outcome of the definitive porcelain laminate veneer restorations is reflected by the shade of the resin luting cements applied. Resin cement systems with similar shade display different colour parameters and change the final ceramic translucency. Variations in underlying porcelain core shade and material thickness may also influence the optical properties of the final restoration. Even though all these changes may not be clinically differentiable, clinicians face a challenge in selection of cement shade within the clinical acceptability and perceptibility threshold to achieve best final result.