Effects of Antenatal Exercise Programme and Education on Health Related Quality of Life: A Randomised Controlled Trial
B Sathya Prabha1, Jaya Vijayaraghavan2, Arun G Maiya3, N Venkatesh4, R Sivakumar5
1 Associate Professor, Faculty of Physiotherapy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
2 Professor, Department of Obstetrics and Gynaecology, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
3 Professor, Department of Physiotherapy, Manipal University of Higher Education, Manipal, Karnataka, India.
4 Course Chairman, Faculty of Physiotherapy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
5 Principal, Faculty of Physiotherapy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. B Sathya Prabha, Associate Professor, Faculty of Physiotherapy, Sri Ramachandra Medical College and Research Institute, Porur, Chennai, Tamil Nadu, India.
E-mail: bsathya_physio@yahoo.co.in
Introduction
Women experience significant physiological and anatomical adaptations during pregnancy to meet the maternal and foetal demands. Most of the women stop exercising or reduce their routine physical activity during pregnancy. Sedentary lifestyle during pregnancy leads to maternal discomforts and complications.
Aim
To evaluate the effect of structured antenatal exercise programme and education on health-related quality of life.
Materials and Methods
In this randomised controlled trial 186 mothers were recruited for the study. A total of 94 Participants were selected as the study group samples and 92 were chosen as the control group as per block randomisation method. The study group received structured antenatal classes and education from 20-weeks of gestational age in addition to routine antenatal care where as the control group received routine antenatal care and antenatal exercises. SF 36 questionnaire-V2 was assessed at baseline and 32-weeks of gestation. Comparison of psychometrically-based Physical Component Summary (PCS) and Mental Component Summary (MCS) scores were done using paired and unpaired t-test.
Results
A significant difference in the PCS and MCS values between the groups at 32-weeks (p-value<0.05) was observed. The results showed that the exercise programme benefitted the study group. Exercise during pregnancy increased the β endorphin levels and decrease the perception of pain and could contribute of better improvement in physical and mental health of the participants.
Conclusion
The health-related quality of life of pregnant women were improved by the 12-week antenatal exercise programme and education.
Antenatal education, Gestational period, Pregnancy exercises
Introduction
Pregnancy induces profound alterations in hormonal, cardiovascular, respiratory, renal and gastrointestinal systems which allow the development of the foetus and prepare the mother and the foetus for the process of delivery [1]. Physical and physiological changes along with general and musculoskeletal discomforts during pregnancy influence the functional status of mothers in various aspects, there by affecting their quality of life. Earlier, the aims of antenatal care were to screen the mothers to detect, prevent and manage the maternal and foetal complications during pregnancy [2]. The antenatal care has been extended to promote awareness of the multiple aspects involved in childbearing such as physical health, mental health and family support [3].
Pregnancy, a phase in a women’s life plays a vital role bringing in subtle changes which hindering their ability to carry out their daily routines, affecting their overall health-related quality of life that reflects on the physical and emotional stress [4]. The goal of medical care during pregnancy aims at favourable outcome of the mother and the baby considering the health-related functional status.
Earlier, there was a lack in the evidence-based practice and guidelines for exercise during pregnancy and the antenatal exercises focus mainly on pelvic floor muscles alone or else symptom-specific approach. The publications of guidelines on “Exercise during Pregnancy” (1985) underwent subsequent revisions from 1994 to 2002 which have become less restrictive but have more progressive evidence-based proofs that are accepted in a wide range [5]. In connection to this, the Canadian guidelines on exercise during pregnancy throws awareness that pregnancy is the apt time to inculcate healthy living styles that includes nutrition and exercise. Antenatal preparation programmes involve several techniques and activities focused on physical and mental health performed by different healthcare professionals. Such programmes may include educational activities for posture care, nutrition, and physical exercise and relaxation techniques [6].
The changes during pregnancy affect not only the musculoskeletal structures but also interfere with the psychological and social aspects, which extend till postnatal period and impact on quality of life of women. Health-related quality of life has physical and mental health components which include the parameters such as physical functioning, body pain, role limitations due to physical health problems, and role limitations due to emotional problems, emotional well-being, social functioning, energy/fatigue, and general health perceptions. Hence, there is a strong indication for checking the effect of antenatal exercise and education on health-related quality of life. Therefore, the present study aimed to evaluate the effect of structured antenatal exercise programme and education on health-related-quality of life.
Materials and Methods
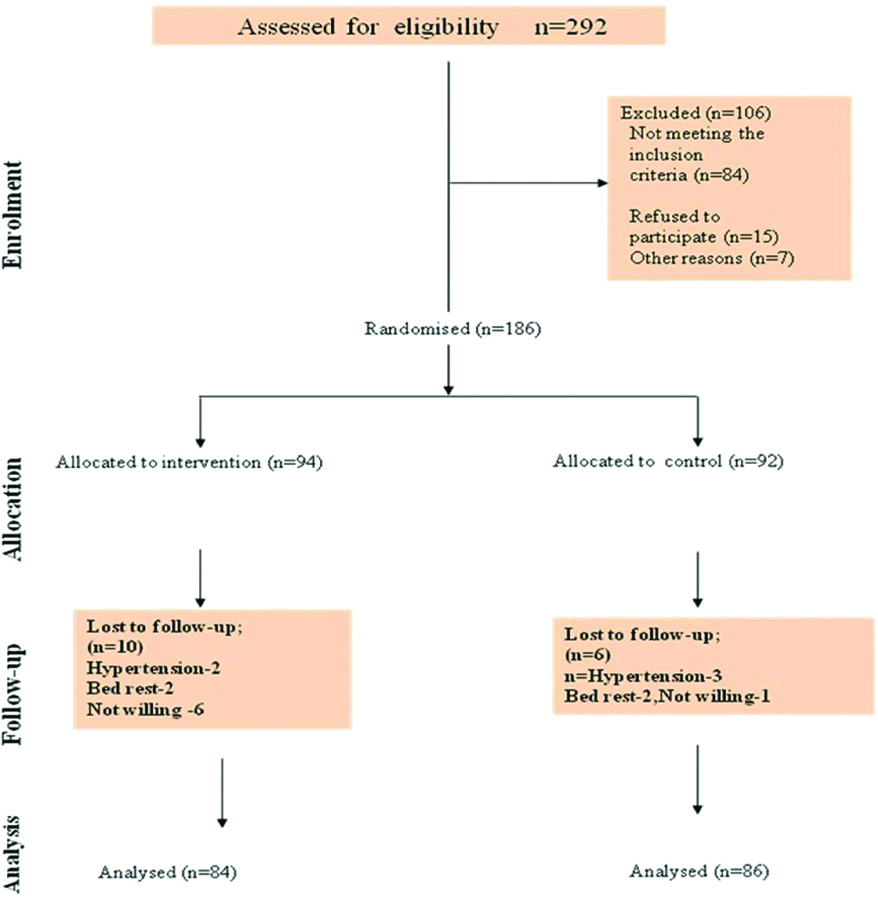
This randomised controlled trial conducted during January 2014-May 2016 at Sri Ramachandra Hospital, Chennai, Tamil Nadu, India, (CTRI/2017/06/008757). The study was approved by Institutional Ethics Committee of Sri Ramachandra Medical College and Research Institute (IEC-NI/11/APR/22/24). Sample size was calculated by Hypothesis Testing for Single Proportion. With a 20% dropout, the Sample size was calculated as 98 in each group. The consort flow chart for the study is shown in [Table/Fig-1]. A total of 292 mothers were screened for eligibility criteria,186 mothers were selected for the study. Mothers aged 21-36 years, gestational age >20 weeks, mothers who planned their childbirth in Sri Ramachandra Hospital were included in the study. Mothers with history of thyroid disease, miscarriage, cervical incompetence, vaginal bleeding or fluid loss, hypertension, pre-existing cardiovascular, respiratory or renal diseases, multiple pregnancies, chronic musculoskeletal pain, anaemia and blood disorders were excluded. Allocation concealment was executed by Sequentially Numbered Opaque and Sealed Envelops (SNOSE) method by using brown opaque envelopes. After the sequence generation was completed, the envelopes were arranged in blocks. Each block consisted of ten participants. The principal investigator generated the sequence, allocated the participants into groups based on the numbers found in the envelope. A total of 94 participants were chosen as the study group participants and 92 were assigned to the control group as per block randomisation method. Informed written consent was obtained from all the study participants.
Antenatal classes were conducted as individualised therapy for interventional group along with routine antenatal care from the 20th week of gestation. Deep breathing exercises, pelvic floor exercise, neck exercises, arm and leg exercises, trunk exercises, pelvic tilting exercises, relaxation technique, Stretching exercise for low back, calf, adductors, wall exercises, Floor exercises for stretching hamstrings, low back, adductors (8-10 repetitions with the duration of 15-20 minutes; 3-5 times a week). Education on pregnancy changes, guidelines and warning signs of exercise, posture and back care were given. Walking for 15-20 minutes was advised to improve aerobic endurance. As per the set principles of the American College of Sports Medicine (ACSM) and the American College of Obstetricians and Gynaecologists (ACOG) guidelines such as regular exercise 3-5 times/week, heart rate should not exceed 70% of maximal heart rate, moderate intensity exercise for 20 minutes, maintain adequate fluid in take, to ensure adequate warm up and cool down period, avoid exercising in supine after the end of fourth month and warning signs for training sessions were followed [7]. Audiovisual aids and handouts were used for education and follow-up were ensured.
The mothers of each group were asked to fill SF 36 questionnaire (Short Form v2-four week recall) at their first session. The SF-36v2 comprised of 36 questions which derive psychometrically-based PCS and MCS scores. The functional health and the general well-being of the patients were determined using SF-36v2 health Survey tool. Both the English and Tamil versions of SF36 were used in this study. Certified scoring software 5.0 was used for analysis. The SF-36v2 Health Survey can be completed in 5-10 minutes and found to be a practical, reliable and valid measure of physical and mental health [8].
First two sessions were conducted between 20-24 weeks of gestational age. Next three sessions were conducted, once every two weeks. At the end of the fifth session (32 weeks), mothers in the interventional and control group were requested to fill SF 36 questionnaire. The principal investigator rendered the care to both groups. The SF-36v2 was administered by a well-qualified, experienced physiotherapist who was blinded about the group allocation. Control group were on routine antenatal care (Deep breathing exercise, pelvic floor exercises, ankle exercises. Education on posture and back care and walking for 15-20 minutes). Exercise adherence diary maintained for 12-weeks follow-up. SF 36 was assessed at 20 and 32 weeks of gestation.
Statistical Analysis
The data were analysed using SPSS 23.version. Certified scoring software 5.0 was used for SF 36-v2 analysis. Descriptive statistics was done to analyse the demographic characteristics. Frequency and percentage was used to summarise categorical variables. Unpaired t-test used to compare the domains of SF 36 questionnaire between the groups. Paired t-test used to compare the domains of SF 36 questionnaire within groups.
Results
The baseline demographic characteristics such as age of both the groups were comparable at the baseline. The anthropometric characteristics such as height and BMI were also comparable at baseline [Table/Fig-2]. The interventional and the control group mothers were analysed using the SF 36 questionnaire to assess health related quality of life. It was evaluated with a baseline at 20-weeks and 32-weeks. The between group analysis showed an improvement in PCS and MCS score in the interventional group at 32-weeks [Table/Fig-3]. The within group analysis revealed a significant improvement in MCS score in the interventional group [Table/Fig-4]. The results showed that the exercise programme benefitted the study group. Following the 12-week antenatal exercise programme, trends of improvement in the Physical Component Summary, mental component summary and several of its domains with statistically significant changes were observed (p<0.05). Most of the participants in the study and control group adhered to the exercise programme for a minimum of four days per week. Among the exercising group, 51.19% of the mothers showed a minimum four days adherence with exercise programme. In the control group maximum of mothers (68.60%) practiced the exercises for four days per week.
Baseline characteristics of both groups.
| Characteristics | Interventional Mean (SD) | Control Mean (SD) |
|---|
| Age (years) | 26.30 (3.35) | 26.24 (2.55) |
| Height (cm) | 159.61 (4.61) | 158.97 (3.63) |
| Prepregnancy BMI (kg/m2) | 24.2 (1.68) | 24.41 (1.54) |
| Numbers (%) | Numbers (%) |
| Education-schooling | 22 (26.2%) | 20 (23.3%) |
| Under graduates | 53 (63.1%) | 50 (58.1%) |
| Post graduates | 9 (10.7%) | 16 (18.6%) |
| Employment status |
| Homemaker | 63 (75%) | 60 (69.8%) |
| Employed | 21 (25%) | 26 (30.2%) |
| Residence |
| Rural | 52 (61.9%) | 49 (57%) |
| Urban | 32 (38.1%) | 37 (43%) |
| Total | (n=84) | (n=86) |
Comparison of physical cumulative score, mental cumulative score between the study and the control group.
| SF-36 | Mean (SD) | Mean (SD) | Mean diff. | p-value |
|---|
| Interventional | Control |
|---|
| PCS |
| 20 weeks | 51.05 (6.90) | 49.82 (7.97) | 1.23 | 0.284 |
| 32 weeks | 52.25 (5.75) | 49.97 (6.92) | 2.28 | 0.020* |
| MCS |
| 20 weeks | 42.70 (4.78) | 42.47 (05.82) | 0.24 | 0.773 |
| 32 weeks | 46.07 (7.05) | 43.02 (05.61) | 3.05 | 0.002* |
PCS: Physical cumulative score; MCS: Mental cumulative score
*Significant at p<0.05, unpaired t-test
Comparison of PCS, MCS score within the study and control groups.
| SF-36 | Group | Mean (SD) | t-value | p-value |
|---|
| 20 week | 32 week |
|---|
| PCS | Interventional | 51.05 (6.90) | 52.25 (5.75) | 1.045 | 0.299 |
| Control | 49.82 (7.97) | 49.97 (6.92) | 0.183 | 0.855 |
| MCS | Interventional | 42.70 (4.78) | 46.07 (7.05) | 3.700 | 0.0001* |
| Control | 42.47 (05.82) | 43.02 (05.61) | 0.723 | 0.472 |
PCS: Physical cumulative score; MCS: Mental cumulative score
*Significant at p<0.0001, paired t-test
Discussion
The physical and the physiological changes during pregnancy would have an impact on the physical and mental health and thus affecting the well-being of the mother [9]. Bringing in awareness on benefits of physical activity during pregnancy would helpful us in giving effective interventions which would better result in the health-related quality of life of a pregnant woman.
The between group analysis revealed that physical functioning, general health, vitality, social functioning, and mental health are positively influenced by the moderate intensity of physical activity. Similarly, within group results showed improvements in the physical and mental health domains such as general health, vitality, social functioning and mental health. This finding is similar to the previous study by Montoya Arizabaleta AV et al., in contrast to that, the study by Petrov-Fieril K et al., observed that the resistance training during pregnancy showed normal health related quality of life in both the groups [10,11].
During pregnancy, both the musculoskeletal and psychological symptoms seemed to be important determinants of health status of a mother where as in the postpartum period social support was one of the main factors than the physical symptoms and lactation problems [12]. Physiologically, exercise during pregnancy increased the β endorphin levels above the increased levels in pregnancy. Therefore, by exercising during pregnancy could decrease the perception of pain and could contribute to improvement in physical and mental health of participants. The study results have shown that moderate-intensity physical activity of the participants was positively associated with one or more domains of health-related quality of life.
The adaptation during pregnancy induces both physical and psychological changes. The pregnant women in this randomised controlled trial group showed better physical and psychological well-being than the control group participants. The inference from the study confirms that antenatal exercise programme improved the health-related quality of life of mothers.
It was found that most of the participants in the study group adhered to the exercise programme for a minimum of four days per week. As per the set principles of the ACSM and the ACOG [13], the frequency of antenatal exercises could be minimum 3-5 days per week. In spite of the increased exercise adherence in the control group (68.60%), the interventional group had exhibited better health-related quality of life. Six mothers in interventional group and one mother in the control group were not able to comply with the exercise sessions due to tiredness, lack of motivation, cultural aspects and beliefs, lack of familial support, work commitments and transportation [14]. Davies GA et al., stated that pregnant women should be motivated to participate in aerobic exercise to improve healthy lifestyle [15]. Jackson RA et al., found that the educational intervention on diet and exercise improved exercise performance and health perception among pregnant mothers [16]. The current study shows that the interventional exercise programme proved to be feasible for pregnant mothers that benefitted the improvement of their quality of life.
Limitation
Mothers baseline parameters at 20-weeks such as physical activity levels, first trimester discomforts like nausea, vomiting and tiredness were not included in the study.
Conclusion
The 12-week antenatal exercise programme brought about statistically significant changes in the Physical Component Summary, Mental Component Summary and several of its domains. Hence, the present study suggests the comprehensive structured antenatal exercise and education programme in routine antenatal care.
PCS: Physical cumulative score; MCS: Mental cumulative score
*Significant at p<0.05, unpaired t-test
PCS: Physical cumulative score; MCS: Mental cumulative score
*Significant at p<0.0001, paired t-test
[1]. Stephenson RG, O’Connor LJ, Obstetric and gynecologic care in pregnancy 2000 second editionSlack Incorporated [Google Scholar]
[2]. World Health Organization (WHO), What is the effectiveness of antenatal care. 2005. Available from: http://www.euro.who.int/ data/assets/pdf file /0005/74660/E87997.pdf [Google Scholar]
[3]. National Health Service (NHS), United Kingdom, Ante-natal care: routine care for the healthy pregnant woman. 2008. Available from: http://www.nice.org.uk/nicemedia/pdf/CG062NICEguideline [Google Scholar]
[4]. Gustafsson MK, Stafne SN, Romundstad PR, Mørkved S, Salvesen K, Helvik AS, The effects of an exercise programme during pregnancy on health-related quality of life in pregnant women: a Norwegian randomised controlled trialBJOG 2016 123:1152-60.10.1111/1471-0528.1357026265465 [Google Scholar] [CrossRef] [PubMed]
[5]. Wolfe LA, Davies GAL, Canadian guidelines for exercise in pregnancyClinical Obstetrics and Gynecology 2003 46(2):488-95.10.1097/00003081-200306000-00027 [Google Scholar] [CrossRef]
[6]. Miquelutti M, Cecatti J, Makuch M, Developing strategies to be added to the protocol for antenatal care: An exercise and birth preparation programClinics 2015 70(4):231-36.10.6061/clinics/2015(04)02 [Google Scholar] [CrossRef]
[7]. Artal R, Exercise in pregnancy: GuidelinesIn Clinical Obstetrics and Gynaecology 2016 59(3):639-44.10.1097/GRF.000000000000022327398880 [Google Scholar] [CrossRef] [PubMed]
[8]. Mc Dowell I, Measuring health: A guide to rating scales and questionnaires 2006 3rd edNew York: NYOxford University Press:520-703.General health status and quality of life10.1093/acprof:oso/9780195165678.003.0010 [Google Scholar] [CrossRef]
[9]. Haas JS, Jackson RA, Fuentes-Afflick E, Stewart AL, Dean ML, Brawarsky P, Changes in the health status of women during and after pregnancyJ Gen Intern Med 2005 20(1):45-51.10.1111/j.1525-1497.2004.40097.x15693927 [Google Scholar] [CrossRef] [PubMed]
[10]. Montoya Arizabaleta AV, Orozco Buitrago L, Aguilar de Plata AC, Mosquera Escudero M, Ramirez-Velez R, Aerobic exercise during pregnancy improves health-related quality of life: a randomised trialJournal of Physiotherapy 2010 56:253-58.10.1016/S1836-9553(10)70008-4 [Google Scholar] [CrossRef]
[11]. PetrovFieril K, Glantz A, Fagevik Olsen M, The efficacy of moderate-to-vigorous resistance exercise during pregnancy: A randomized controlled trialActa Obstetriciaet Gynecologica Scandinavica 2015 94(1):35-42.10.1111/aogs.1252525287282 [Google Scholar] [CrossRef] [PubMed]
[12]. Hueston WJ, Kasik-Miller S, Changes in functional health status during normal pregnancyJ Fam Pract 1998 47(3):209-12. [Google Scholar]
[13]. ACOG Committee on Obstetric PracticeCommittee opinion 267: exercise during pregnancy and the postpartum periodObstetrics & Gynaecology 2002 99(1):171-73.10.1016/S0029-7844(01)01749-5 [Google Scholar] [CrossRef]
[14]. Smith KM, Campbell CG, Physical activity during pregnancy: Impact of applying different physical activity guidelinesJournal of Pregnancy 2013 2013:165617http://dx.doi.org/10.1155/2013/16561710.1155/2013/16561723476778 [Google Scholar] [CrossRef] [PubMed]
[15]. Davies GA, Wolfe LA, Mottola MF, MacKinnon C, Arsenault MY, Bartellas E, Exercise in pregnancy and the postpartum periodJournal of Obstetrics and Gynaecology Canada 2003 25(6):516-29.10.1016/S1701-2163(16)30304-8 [Google Scholar] [CrossRef]
[16]. Jackson RA, Stotland NE, Caughey AB, Gerbert B, Improving diet and exercise in pregnancy with Video Doctor counselling. A randomized trialPatient Education and Counselling 2011 83(2):203-09.10.1016/j.pec.2010.05.01921459255 [Google Scholar] [CrossRef] [PubMed]