A Rare Case of Primary Hydatid Cyst of Right Thigh
Esheet Shah1, Shailesh Shah2
1 Senior Consultant, Department of General Surgery, Dr Shailesh Shah Surgical Hospital and Endoscopy Clinic, Ahmedabad, Gujarat, India.
2 Senior Consultant, Department of General Surgery, Dr Shailesh Shah Surgical Hospital and Endoscopy Clinic, Ahmedabad, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shailesh Shah, Dr Shailesh Shah Surgical Hospital and Endoscopy Clinic, Ahmedabad-380022, Gujarat, India.
E-mail: srsnss@hotmail.com
Hydatid cyst is a parasitic infestation caused by Echinococcus granulosus commonly affecting liver and lung. Hydatid disease of the soft tissue is uncommon. Here, we present a case of 48-year-old male with multicystic hypoechoic lesion seen deep to muscular layer in the posteromedial region of the right thigh. The initial diagnosis was made based on Ultrasonography (USG) and Magnetic Resonance Imaging (MRI). Complete surgical excision of the mass was done and the patient had an uneventful postoperative recovery. Hydatid cyst should be diagnosed with USG and MRI. Complete excision of the hydatid cyst is recommended.
Echinococcus, Intramuscular, Parasitic infestation
Case Report
A 48-year-old male presented to our hospital with a cystic mass in the posteromedial region of the right thigh. Chief complaints were swelling over the right thigh gradually increasing in the size for the past 6-7 years. No significant medical or family history was noted.
A 12×10 cm mass was present in the right lower limb, 10 cm below and 6 cm lateral to the pubic symphysis. Swelling was firm in consistency, fixed to the skin, non-mobile in any axis and was prominent on flexing the lower limb. No pulsation or transillumination was noted.
Initial laboratory results were normal except for haemoglobin level that was 10.4 gm%. Ultrasonography (USG) examination was performed using 10 MHz high-frequency probe, which revealed an approximately 19×19 cm sized multicystic hypoechoic lesion deep into the muscular layer of the posteromedial region of the right thigh. Multiple cysts of varying size and multiple small foci of calcifications were also noted. The underlying muscles appeared normal and no abscess was noted.
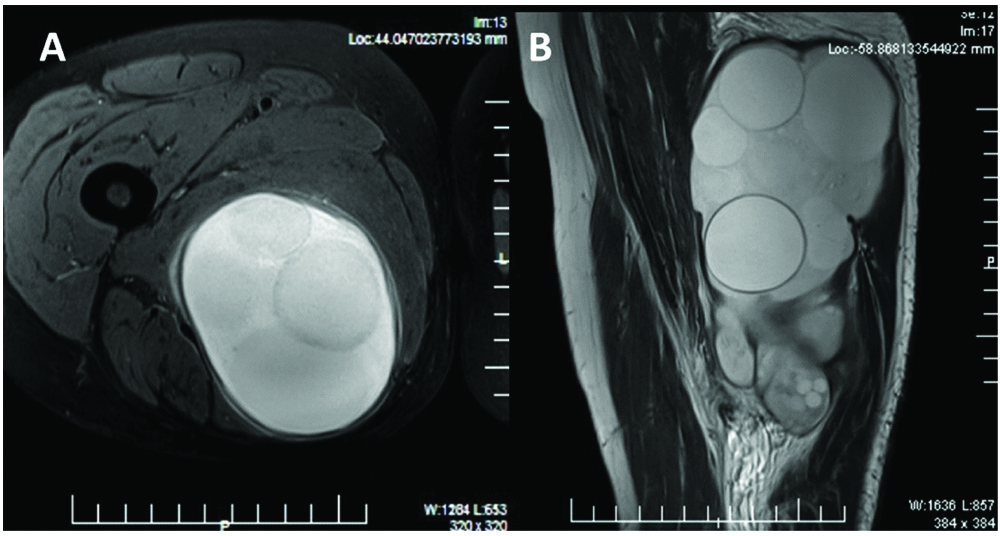
MRI revealed a 9.5×7.3×16.5 cm well-defined oval cystic lesion involving right adductor muscle at upper mid-thigh level with perifocal inflammatory oedema [Table/Fig-1]. Femur showed normal signal intensity. No abnormal medullary signal intensity was seen. No evidence of fracture, stress response or bone oedema was seen. Femoral neuro-vascular bundle and sciatic nerve appeared remarkable. The surgery was planned considering hydatid cyst as a provisional diagnosis.
(a) Transverse, (b) Longitudinal MRI section through the lesion.
Surgical exploration of the mass was performed under regional (spinal) anaesthesia. Operative findings revealed a 12×12×10 cm swelling over the medial, anterior and posterior aspect of right thigh adherent to the adductor longus and adductor magnus muscle. The cystic mass was also adherent to the sciatic nerve posteriorly and the Hunter canal. After the mass was separated from surrounding structures, a thorough examination was done for any daughter cyst or satellite lesion. The surgical site was irrigated with betadine and hydrogen peroxide and the subcutaneous tissues and skin were closed.
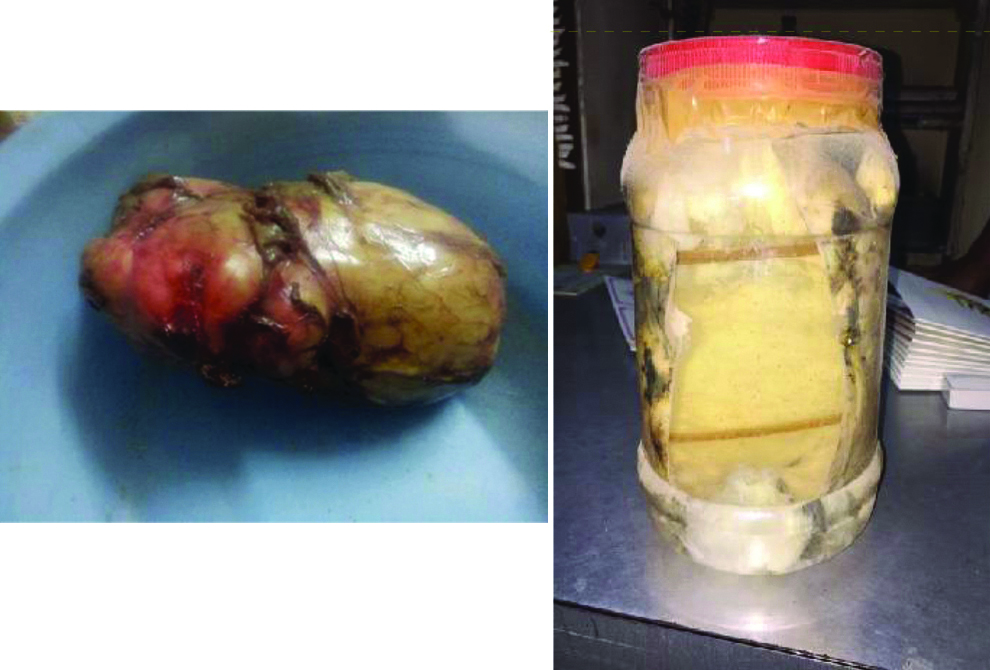
Histopathological examination confirmed the diagnosis of hydatid cyst. The gross description reported a large shaped cystic yellowish-brown soft tissue mass 14×10×8 cm oozing a milky white material on sectioning [Table/Fig-2]. Inner wall showed multiple tender coconuts like daughter cysts. No evidence of granuloma or malignancy was noted. The postoperative period was uneventful and the patient was discharged on oral cefpodoxime proxetil.
Discussion
Echinococcosis or hydatid disease is commonly found in rural areas and the primary hosts for E.granulosus are carnivore and intermediate hosts are herbivore [1]. More than 90% of these cases occur in the liver, lungs or both [2]. However, musculoskeletal involvement is rarely found in around 1% to 4% of overall cases [1,3].
Humans are accidentally infected by ingesting contaminated water or vegetables. As the larvae enter the host’s body it migrates through the bloodstream penetrating the intestinal mucosa and gets stuck in the capillary bed of the liver, resulting in the liver cysts occurring in around 75% of cases. However, some penetrate into systemic circulation resulting in cysts of lung, muscles, soft tissues, brain or bones [4].
Around 15% of occurrence of cysts accounts for lung, 8-10% extra-ordinary sites and 1-4% in musculoskeletal regions [5,6]. Muscle is considered an unfavourable site for the survival of parasites due to the presence of high lactic acid level, muscular contractions and blood filtering functions of liver and lungs. Hydatid cysts may occur in any part of the human body except nails, hair, and teeth. However, proximal muscles of lower extremity could be one of the sites due to rich blood supply and presence of muscle mass [7].
Few cases of hydatid cysts of thigh have been reported [Table/Fig-3], our case adds to the literature on how these rare cases can be successfully diagnosed and managed [6-15]. It may also help in future to develop treatment strategies for such rare occurrences.
Summary of previously reported cases of primary hydatid cyst of thigh [6-15].
| Author | Country | Age (years) | Sex | Side | Size | Symptoms since | Treatment |
|---|
| Landolsi MM et al., [8] | Tunisia | 27 | Male | Right | 10×6 cm | 6 months | Excision |
| Taki-Eldin AA [9] | Saudi Arabia | 45 | Female | Right | 8×6 cm | 1 year | Excision and albendazole |
| Bothale KA et al., [10] | India | 70 | Female | Right | 2 cysts. 10×4.5×4 cm and 4.5×2.5×2 cm | 2 years | - |
| Argy N et al., [11] | France | 60 | Female | Right | 2 cysts of 7×3.5 cm | 6 months | Pericystectomy and albendazole |
| Yalavarthi S et al., [12] | India | 75 | Male | Left | 18×15 cm | 2 years | Excision |
| Gupta A et al., [7] | India | 38 | Male | Right | 5×7 cm | 10 months | Excision and albendazole |
| Bansiwal RK et al., [13] | India | 60 | Female | Left | 25×15 cm | 30 years | Excision and albendazole |
| Hamdi MF et al., [6] | Tunisia | 25 | Female | Right | 8×5×5 cm | - | Excision |
| JerbiOmezzine S et al., [14] | Tunisia | 82 | Male | Left | 10×5 cm | 5 months | Excision |
| Arora V et al., [15] | India | 50 | Female | - | 10×5 cm | 4 months | Excision |
| Current case | India | 48 | Male | Right | 12×12×10 cm | | Excision |
Surgery is the most effective treatment of choice for hydatid cysts. It should be removed radically whenever possible. During surgery, spillage of the cysts content is to be avoided as it causes dangerous anaphylaxis and dissemination. Intraoperative irrigation using 0.5% cetrimide, 15% hypertonic saline and 0.5% silver nitrate solution can be done which kills the daughter cysts and further reduces the occurrence of the anaphylactic reaction [7]. In our case, after excision of the cysts, the surgical site was irrigated using betadine and hydrogen peroxide to avoid dissemination of the hydatid cysts.
Conclusion
A hydatid cyst is rarely seen in the thigh and should be diagnosed with USG and MRI. Complete excision of the hydatid cyst is recommended.
[1]. McManus DP, Zhang W, Li J, Bartley PB, EchinococcosisLancet 2003 362(9392):1295-304.10.1016/S0140-6736(03)14573-4 [Google Scholar] [CrossRef]
[2]. Koc Z, Ağıldere AM, Yalcın Ö, Pourbagher A, Pourbagher M, Primary hydatid cyst in the anterior thigh: Sonographic findingsJ Clin Ultrasound 2004 32(7):358-60.10.1002/jcu.2004415293304 [Google Scholar] [CrossRef] [PubMed]
[3]. Vicidomini S, Cancrini G, Gabrielli S, Naspetti R, Bartoloni A, Muscular cystic hydatidosis: Case reportBMC Infect Dis 2007 7:2310.1186/1471-2334-7-2317397535 [Google Scholar] [CrossRef] [PubMed]
[4]. Abi Saad GS, Musallam KM, Korban ZR, Reslan OM, Mneimne M, Solitary hydatid cyst of the thigh: A challenging diagnosisVector Borne Zoonotic Dis 2009 9(6):743-45.10.1089/vbz.2008.008619272001 [Google Scholar] [CrossRef] [PubMed]
[5]. Ghoroobi J, Mohajerzadeh L, Mirshemirani A, Mahdavi A, Primary hydatid cyst of thigh: a case report in childJ Krishna Inst Med Sci 2017 6(1):111-13. [Google Scholar]
[6]. Hamdi MF, Touati B, Abid A, Primary hydatid cyst of the biceps femorisMusculoskelet Surg 2010 94(1):59-61.10.1007/s12306-010-0056-920131024 [Google Scholar] [CrossRef] [PubMed]
[7]. Gupta A, Singal RP, Gupta S, Singal R, Hydatid cyst of thigh diagnosed on ultrasonography - A rare case reportJ Med Life 2012 5(2):196-97. [Google Scholar]
[8]. Landolsi M, Kouki S, Abdennadher A, Hydatid cyst of the thigh: a challenging diagnosisBMJ Case Rep 2017 2017:piibcr-2017-222113. doi: 10.1136/bcr-2017-22211310.1136/bcr-2017-22211329025784 [Google Scholar] [CrossRef] [PubMed]
[9]. Taki-Eldin AA, A solitary primary subcutaneous hydatid cyst in the thigh: A case reportInt Surg J 2016 3(1):411-14.10.18203/2349-2902.isj20160272 [Google Scholar] [CrossRef]
[10]. Bothale K A, Kolhe H, Mahore SD, Wilkinson AR, Diagnosis of primary hydatid cyst of thigh by fine needle aspiration cytologyIndian J Med Microbiol 2015 33(1):151-53.10.4103/0255-0857.14842625560023 [Google Scholar] [CrossRef] [PubMed]
[11]. Argy N, AbouBacar A, Boeri C, Lohmann C, Pfaff AW, Hansmann Y, Primary musculoskeletal hydatid cyst of the thigh: Diagnostic and curative challenge for an unusual localizationCan J Infect Dis Med Microbiol 2013 24(3):e99-e101.10.1155/2013/82947124421841 [Google Scholar] [CrossRef] [PubMed]
[12]. Yalavarthi S, Satya NV, Ramamurti T, Supriya M, Intermuscular hydatid cyst in the thigh: An unusual presentationMed J DY Patil Univ 2013 6:191-93.10.4103/0975-2870.110311 [Google Scholar] [CrossRef]
[13]. Bansiwal RK, Sharma R, Attri AK, A large primary hydatid cyst of thigh: A case reportIndian J Surg 2011 73(2):158-60.10.1007/s12262-010-0205-222468070 [Google Scholar] [CrossRef] [PubMed]
[14]. JerbiOmezzine S, Abid F, Mnif H, Hafsa C, Thabet I, Abderrazek A, Primary hydatid disease of the thigh. A rare locationOrthop Traumatol Surg Res 2010 96(1):90-93.10.1016/j.otsr.2009.10.016 [Google Scholar] [CrossRef]
[15]. Arora V, Nijjar IS, Gill KS, Singh G, Case report: Primary hydatid cyst of muscle - a rare siteInd J Radiol Imag 2006 16(2):239-41.10.4103/0971-3026.29100 [Google Scholar] [CrossRef]