The success of a replanted or revascularised limb depends not only on the survival of the limb but also on the functional recovery and the ability of the patient to perform Activities of Daily Living (ADL) with minimal or no effort. The speed of recovery must be within acceptable limits and the limb has a satisfactory appearance with little or no pain [1].
The success rate for digital replantation surgery can be as high as 94.98% as reported by Chen J et al., [2]. They concluded that decreasing ischaemic time and prevention of vascular crises were important in ensuring survival of the digital replant. They alluded to the importance of functional outcome but did not include it in their study. Estrella EP et al., in a study done in Philippines mentioned stiffness in their digital replant patients even after six months post surgery [3]. However, at least four patients in their study did not have data on functional outcomes. There is a perception that distal digital replant has little functional gain but Sebastin SJ et al., in a systematic review dismissed this perception reporting good functional outcomes [4]. Their review included studies done in East Asia, Thailand, Europe and North America.
Mahajan R et al., assessed 17 patients in India who underwent replantation surgery at the wrist level and reported that patients were able to perform most activities [5]. Two had excellent results and ten had good results. Kamarul T et al., studied the functional outcome of 55 patients undergoing either revascularisation or replantation surgery at the wrist, thumb, transmetacarpal and fingers using the Quick-DASH and MHQ scores [6]. They categorised it as a least satisfactory outcome. Both Kamarul T et al., and Sebastin SJ et al., agreed that there is a lack of studies on functional outcome for comparison [4,6].
The present aimed to evaluate the long-term functional outcome of revascularisation and replantation surgery of the fingers, thumbs, transmetacarpal, wrists, forearms and arms. Specifically, this study included more detailed functional outcomes such as grip strength, pinch strength, motion, 2 point-discrimination and cold intolerance.
Materials and Methods
This was a retrospective cross-sectional study. Twenty-seven patients over the age of 17-years-old with partial or total amputation of the upper limb {digit(s), wrist, forearm and arm} who underwent revascularisation or replantation between June 2003 and May 2006 were included in this study. Authors had obtained approval from the Ethical Committee-Code SPPI/UKM/2010/K013465.
Inclusion criteria were viable and successful replanted or revascularised limb/digits. Viable and successful was defined as a pink distal segment with circulation and not necrotic or gangrenous. Exclusion criteria were patients who did not attend further follow-up clinic sessions or declined to be in the study.
Data were collected from the Hand and Microsurgery database and operative records between June 2003 and May 2006 were included. Patients were assessed in clinic between June 2008 and May 2009. Details obtained included occupation, dominant hand, level of injury, mode and severity of injury, delay until operative time, length of hospital stay and length of absence from work. Delay until operative time was defined as the duration between the injury and the time of surgery. Surgery was performed by two surgeons with experience in Hand and Microsurgery.
Grip strength was measured using the Jamar dynamometer, whilst the pinch strength was measured using a pinch gauge. Total Active range of Motion (TAM) was measured using a goniometer. Percentage of TAM was calculated using the formula below:

Estimate of normal PIP and DIP motion is 175 degrees. The calculated value is converted into grades according to the “Modified Strickland classification” with 0-24% (Poor), 25-49% (Fair), 50-74% (Good) and 75-100% (Excellent) [7].
Two Point Discrimination (2PD) with a measurement of 5 mm or less was considered normal, 6-10 mm considered moderately impaired and >10 mm is considered severely impaired. McCabe’s questionnaire was used to assess cold intolerance which was divided into four groups according to the severity of the cold intolerance: normal/minimal (<10), mild (10-20), moderate (21-30) and severe (>30 severe) [8]. The DASH questionnaire was used to assess the patients’ symptoms and physical function. The lower the score the better the outcome [9].
Statistical Analysis
Statistical analysis using Pearson linear correlation was used to find correlation between DASH score and delay to time for operation and between DASH score versus hand grip power. The student t-test was used to test statistical significance between mean of DASH score to mean of other similar studies and between DASH score and cold intolerance. SPSS utilised was SPSS version 17.0.
Results
All 27 patients were males between 17 to 46-year-old (mean age of 27 years). Ethnic composition was Chinese (55%), followed by Malay (30%) and Indian (15%).
A total of 28 surgeries were performed: 18 revascularisations and 10 replantations. One patient required both revascularisation and replantation surgery where the index finger was replanted and the middle finger radial digital artery was revascularised. Another patient underwent heterotropic implantation with the middle finger implanted to the index finger of the left hand after sustaining complete amputation of both fingers.
The level of amputation was thumb (n=6, 21.4%), fingers (n=6, 21.4%), transmetacarpal (n=6, 21.4%), wrist (n=4, 14.2%), forearm (n=5, 18.0%) and arm (n=1, 3.6%). Mechanism of injury comprised of 12 cases (44%) with industrial or work-related injury and another 12 cases (44%) were due to assault by a sharp object. Two patients (8%) were involved in motor vehicle accidents and 1 (4%) patient sustained the injury at home.
The mean length of stay following revascularisation and replantation surgery was 11 days, ranging from 4 to 20 days. The mean period of absence from work was 9.6 months (range 3-24 months). The mean delays until operative time (time to surgical operation from the moment of trauma) were 8 hours and 30 minutes (range 4-12 hours). Duration of follow-up ranged from a minimum of 24 months to 72 months. The mean result for 2PD test was 8.03 mm (range 4-20 mm). Only two patients had normal 2PD, whilst, 22 patients had moderate impairment and three patients had severe impairment. Of the three patients with severe impairment, their 2PD was >10 mm with two sustaining crush injuries and one with multi-level lacerations.
Objective variables were measured and statistical analysis was done [Table/Fig-1].
Variables measured in the study and type of comparison made with the relevant statistical test.
| Variable | Method of comparison | Statistical Test |
|---|
| Level of injury | Simple comparison | None |
| Power grip, pinch grip | Simple comparison | None |
| Two point discrimination | Simple comparison | None |
| Total active motion | Simple comparison | None |
| DASH versus delay until operation | Pearson’s correlation | Negative r=-0.644 p<0.001 |
| DASH versus power grip of hand | Pearson’s correlation | Positive r=0.193 |
| DASH versus cold intolerance | Student t-test | No significance |
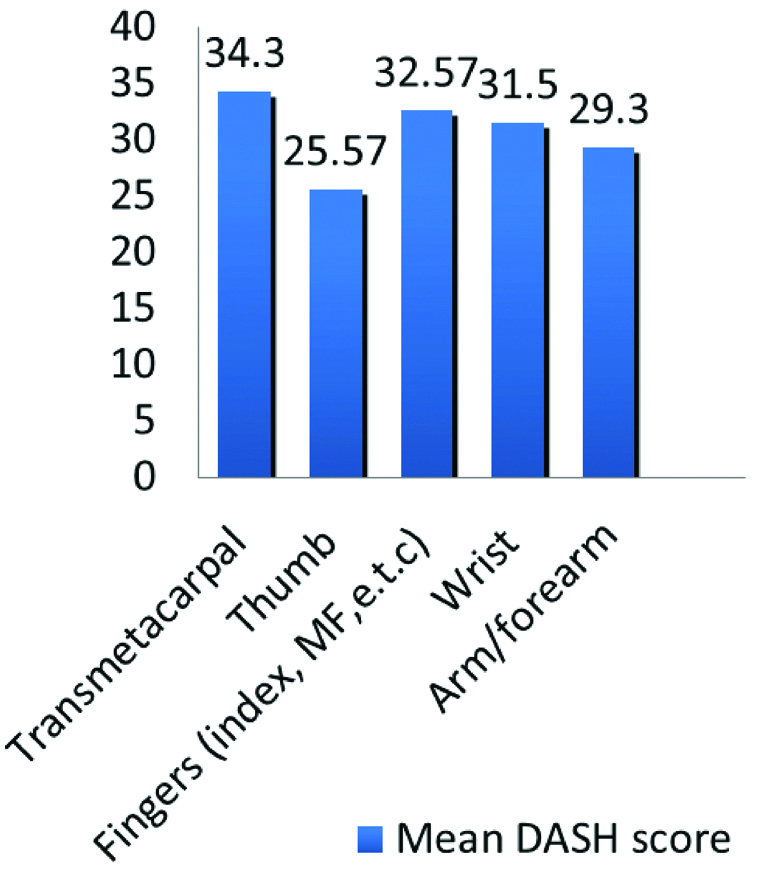
Level of injury: The mean DASH score was 30.1 (range 12 to 78). Majority of the patients (19) had impairment of ADL. Five patients had no impairment in ADL or work and only three had impairment in both ADL and work. When the mean DASH score was compared according to level of injury, the highest mean DASH score was noted in the transmetacarpal group (34.3). This was followed by injury at the level of the finger (32.6), wrist (31.5), arm (29.3) and thumb (25.6) [Table/Fig-2].
Bar graph comparing mean of DASH score according to level of injury.
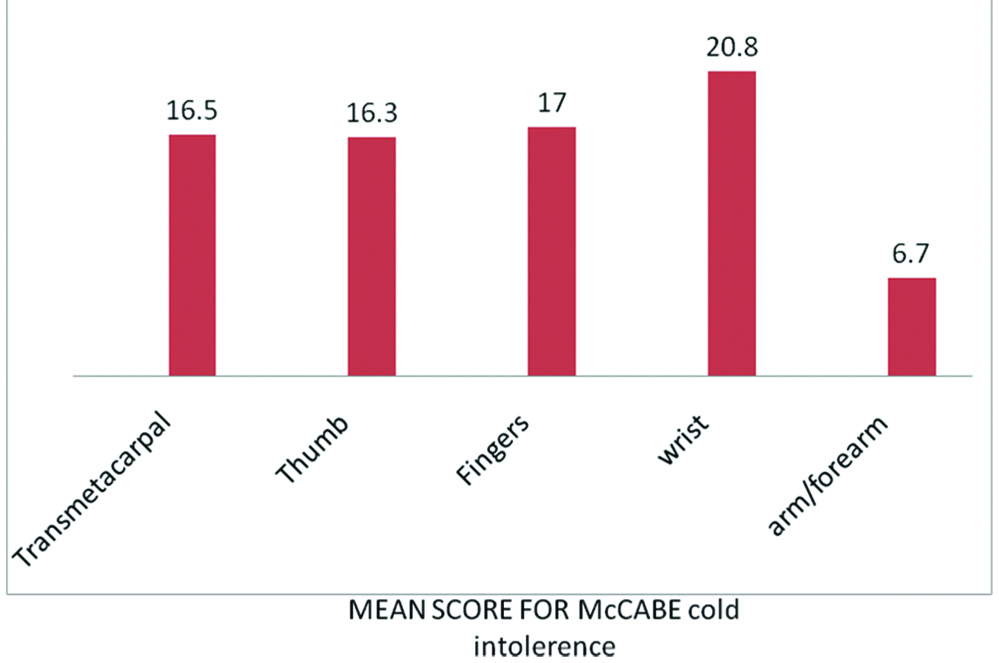
Cold intolerance: The mean score recorded for McCabe’s cold intolerance test was 15.03 (range 3-30). The number of patients that had mild, minimal and moderate cold intolerance was 6, 14 and 7, respectively. None of the patients had severe cold intolerance. The highest mean score was recorded in the wrist level injury group (20.8). This was followed by injury at the level of the finger (17), transmetacarpal (16.5), thumb (16.3) and arm/forearm (6.7) [Table/Fig-3].
Bar chart comparing the mean of McCabe’s cold intolerance score according to level of injury.
Hand and pinch grip: The mean grip strength of the affected hand was 5.26 kg (range 2-10) whilst the mean grip strength for the unaffected hand was 14.07 kg (range 10-20). The grip strength of the affected hand was 37.4% of the normal grip strength of unaffected side. The mean pinch grip of the affected hand was 15.4 kg (range 13 to 20) and for the unaffected hand was 20.7 kg (range 18 to 23). The pinch grip of the affected hand was 74.4% of the unaffected hand strength.
Total active range of motion: There is higher mean range of motion at the metacarpophalangeal joint level (mean score of 70° in finger(s) as compared to the transmetacarpal or thumb level). Mean results were noted to be fair in the transmetacarpal group (91.4°, score of 28%) and thumb group (75°, score 42.8%) according to modified Strickland classification; while for finger(s) level of injury, the mean score was poor (33°, score 19%). As for wrist and arm/forearm level of injury, the mean active range of motion was 46.3° for the wrist joint and 86.7° for the elbow respectively in which both groups achieved 50% of the active range of motion of the normal ipsilateral joint.
DASH comparisons with statistical analysis: There was positive correlation between the DASH score and delay to operation time (r=0.193) signifying poorer outcome (higher DASH score) with a delay to operation time. There was a negative correlation between DASH score and power of hand grip (r=-0.644, p<0.001) signifying a lower DASH score (i.e., better function) correlates to a stronger hand grip. Comparing DASH scores with cold intolerance, there was no significant difference.
Discussion
Survival of an amputated limb can be as high as 80%-94.98% with advancement in microsurgery techniques [2,10,11]. However, success of surgery depends not only on the survival of a limb but also on its function. A functionless upper limb can ultimately become a hindrance to a patient’s activity. In the present study, the mean DASH score was 30 hence present DASH scores were lower than Zyluk A and Walaszek I, with a recorded mean DASH score of 103 (range 72-148) in their series [12]. Sugun TS et al., recorded the lowest DASH score of 6.7 (range 0-32.5) [13].
Delay to Operative Time
Waikakul S et al., found that the longer the period of warm ischaemia, the poorer the nerve regeneration in replanted fingers [14]. Authors have found that there is positive correlation (r=0.193) between delay in time to surgery and DASH score in which the longer the delay the higher the DASH score.
Two Point Discrimination
The mean 2PD in the present study result was 8.03 mm (range 4-20 mm). In three of present patients, the 2PD was more than 10 mm. Mahajan R and Mittal S, reported a 2PD ranging from 10 to 12 mm [5]. Walaszek I and Zyluk A, reported out of 59 digits, they had three patients with 6 mm and 33 patients with 10 mm 2PD [15]. Urbaniak JR et al., obtained an average 2PD of 12 mm [16].
Level of Injury
The mean DASH scores according to level of injury/amputation were transmetacarpal 34.3, thumb 25.57, multiple fingers 32.57, wrist 31.5 and arm/forearm was 29.3. Dabernig J et al., studied 38 patients with successful replantations with much lower mean DASH scores compared to present score [11]. Their DASH scores were multiple fingers 16.1, thumb10 and single digit replants 11.2. However, Zyluk A and Walaszek I, reported a much higher mean DASH score, transmetacarpal and wrist mean scores were 98 (14 patients) and arm/forearm were 117 (5 patients) [12]. The functional outcome post replantation and revascularisation in present centre are in an acceptable range. The mean DASH score in the present study is statistically significant when compared to the studies of Dabernig J et al., and Zyluk A and Walaszek I, (t=-26.7, p <0.001) [11,12].
Studies by Dabernig J et al., and Walaszek I and Zyluk A, reported proximal injuries had poorer functional outcome as although microsurgery is more complex in the finger, rehabilitation is faster and easier distally i.e., fingers [11,15]. A more proximal injury has a risk of reperfusion injury due to much larger muscle bulk. However, the present study showed a fairly similar range of mean DASH scores for all levels of injury i.e a range between 25.6 to 34.3. Thus, the level of injury does not influence the functional outcome.
A recent study by Kamarul T et al., had an overall Quick-DASH score of 42.82±23.69 which they mentioned as least satisfactory [6]. The score was best for the fingers, followed by the thumbs, wrists and finally the transmetacarpal area. The present scores were best for thumbs, followed by arm and forearm, fingers, wrist and finally transmetacarpal.
Cold Intolerance
The phenomenon of cold intolerance is a common complaint reported by patients after digital replantation. In the present study, majority of our patient had mild or minimal cold intolerance and none complained of severe cold intolerance. The highest mean McCabe’s score was recorded in the wrist level of injury, followed by fingers, transmetacarpal, thumb and the arm, forearm level. The cold intolerance rate found in a study performed by Dabernig J et al., was 86.7% which he attributed to cold climate in their country [11]. They found that the incidence of cold intolerence was 95% in thumb replantations, 81% in single finger replantations and 85% in multiple finger replantations. Authors reported a much higher cold intolerance seen in the wrist level of injury and lowest is in the arm/forearm group. The present mean cold intolerance score of 15.03 was remarkably similar to Walaszek I and Zyluk A, study with a mean score of 15 [15]. Statistical analysis showed no significant correlation between DASH score and McCabe score. Thus, in the present series, cold intolerance was not a major factor affecting the functional outcome.
Grip and Pinch Strength
The mean grip strength postoperatively was 37% of the uninjured contralateral side. This result was lower compared to previous studies [12,15]. The mean pinch grip postoperatively was 71% of the normal side. However, the total grip strength of the hand with at least one replanted/revascularised digit was influenced both by the number of replanted/revascularised digits and the number of missing digits. The worst results were noted in cases of multi digital amputations when not all fingers were replanted. Patients with a lower DASH score had a better grip strength, and it was statistically significant (p<0.001).
Total Active Motion
It is recommended that an attempt should be made to replant instead of performing refashioning of a digit. Hattori Y et al., in their series of 46 patients found that active range of motion and the DASH score was better in the replanted group [17]. All the patients in the replanted group were satisfied compared to only 60% in the refashioned group. In the present study, authors only had two patients with digital replants. One patient with an index finger replant had a DASH score of 12 with full range of motion and normal sensation. The other patient underwent heterotropic replantation (middle finger replanted to the index finger position) and had a DASH score of 33. Authors consider the first patient as having a good outcome and the second as a fair outcome and agree that one should always attempt replants.
Papers reporting on Total Active range of Motion (TAM) of digits following transmetacarpal injuries show range of motion varied from 94°-192°. The mean TAM of 154 degrees was published by Paavilainen P et al., in a series of 43 patients, which is the largest to date for transmetacarpal injuries [18]. The present study had a fair range of motion postoperatively (28%) when classified according to Strickland classification. In transmetacarpal and thumb level of injuries; however the mean TAM was lower compared to Paavilainen P et al., but it was still within the 94°-192° range of motion for the transmetacarpal level injury. However, with only six patients with transmetacarpal level of injury, authors are not able to compare the present study statistically.
Sugun TS et al., reported that amputation located at the level of elbow joint or avulsion type of injury had the most limited range of motion of all upper extremities amputation because of disintegration of the elbow joint in addition to surrounding soft tissue injury [13]. Authors recorded a good range of motion of the elbow in the patients with injuries at the arm/forearm level. Mean active range of motion is 46.3° for the wrist joint and 86.7° for the elbow in which both groups achieved 50% of the active range of motion of the normal ipsilateral joint.
Limitation
Limitations of this study include inability to determine accurately the number of soft tissue injuries such as tendon involvement or muscle injury and a standardised postoperative rehabilitation programme for each patient due to logistical and financial issues.
Conclusion
A longer duration from trauma to surgery significantly resulted in poorer functional outcome. Stronger grip strength significantly resulted in better functional outcome. Cold intolerance did not significantly affect functional outcome. Replantation or revascularisation surgery to attach a partial or total amputation remains a worthwhile endeavour as it shows a considerably good outcome.