Root canals begin as funnel-shaped orifices, generally at or just apical to the cervical line, and end at the apical foramen, which opens apically onto the root surface at or within 3 mm of the centre of the root apex. The success of endodontic treatment revolves around the efficient and effective manipulation and three-dimensional obturation of the apical third of the root canal system [1].
Generally, one or more than one root canal can be observed in a root. In fact, as the canal moves apically two changes can be observed-splitting of the canal into two or more canals or merging of two or more canals into one or more canals. These result in various root canal configurations [2], which Vertucci classified into eight types [3]. With the introduction of newer assessment techniques, several other configurations have been reported, resulting in classifications supplemental to Vertucci’s classification [Table/Fig-1] [4-7].
Simple tubular root canal configurations like Vertucci Types I, IV and VIII are easier to prepare and obturate than configurations involving canal splitting or merging during their course. In Vertucci configuration Types IV (2-2), V (1-2), VI (2-1-2) and VII (1-2-1-2), two canals are present apically, but Type V is more difficult to treat [8] than Type IV owing to splitting of one canal into two in the former. Similarly Types VI and VII require special attention due to merging and splitting of the canals during their course. Gulabivala’s additional configuration Type II (3-2), involving merging of three canals, is more complex than Vertucci Type II (2-1) which involves merging of two canals.
It is important to determine the level at which the root canal splits or merges. Root canals which split in the apical third are more difficult to manage as compared to those that split in the coronal and middle thirds. The early recognition of these configurations may facilitate negotiation, cleaning, shaping, and obturation of the root canal system [9].
Mandibular first molars are the earliest permanent posterior teeth to erupt and are, hence, most frequently in need of endodontic treatment. It is reported that merging is more common than splitting in mandibular teeth and that these variations are more common in the apical third [10].
While several studies have investigated the morphology of mandibular molars, no studies have evaluated the prevalence of configuration types in terms of the number of canals at the apical third, such as the prevalence of configuration Types I (1), II (2–1) and III (1-2-1) in the apical third of roots with one canal or the prevalence of configuration Types IV (2), V (1-2), VI (2-1-2) and VII (2-3-1-2) in roots with two canals at the apical third. Hence, this study was conducted to study the prevalence of configuration types in relation to number of canals at the apical third of mandibular first molar roots.
Materials and Methods
The present experimental study was conducted in the Department of Conservative Dentistry and Endodontics, Institute of Dental Sciences Bareilly, UP after obtaining ethical clearance (Ref No.: IDS/ETHCC/17/39) from the Institutional Ethics Committee. The study was completed in one year (May 2017 to April 2018).
Experimental design: A pilot study was conducted and based on its result using G-Power software sample size was calculated. Sample calculation was performed using 95% confidence intervals. Approximately 250 samples were needed. Mandibular first molars extracted from individuals above 30 years of age were collected without gender bias. Teeth that demonstrated fully-formed roots and intact external root morphology were selected and those with open apices, root resorption, calcifications, damaged roots or endodontic treatment were excluded. Written consent was obtained for usage of patient’s extracted teeth for the purpose of research.
Endodontic procedure: The extracted teeth were cleaned of debris and blood, freed of plaque, calculus and tissue attachments by scaling and stored in normal saline (Kunal remedies Pvt., ltd., Lko, India) until use. Access cavity was prepared on each tooth using round diamond point number 2 (Tizkavan, Iran) and high speed handpiece (Kavo, West Germany). Orifices of the canals were identified using DG16 endodontic explorer (Hu Freidy, Chicago, IL, USA). Teeth were rendered transparent by clearing technique as used in previous studies [3] using the following procedure.
Removal of pulpal tissue with sodium hypochlorite: To remove pulpal tissue and to make canals patent; teeth were stored in 5.25% sodium hypochlorite solution (Magma Polykem UP India) for 48 hours at room temperature (37°C). They were then rinsed in running water for 4 hours to remove all traces of sodium hypochlorite. Sodium hypochlorite removed the pulpal tissue and thus made canals patent.
Decalcification with nitric acid: To avoid distortion of tooth during demineralisation process a weak concentration (5%) of nitric acid (Ranken, Maharashtra, India) was used to remove inorganic tooth structure (enamel). Teeth were stored in acid for 2 to 3 days at room temperature, to achieve demineralisation. The solution was stirred 3 to 4 times a day and replaced daily, as demineralisation occurs at the top of the static acid instead of the bottom. Demineralisation procedure was continuously monitored just to remove inorganic tooth structure and was confirmed by checking for tooth softening felt with a sharp-pointed instrument inserted into the tooth crown. After completion of decalcification, the teeth were rinsed under running tap water for 4 hours. Similar technique was used by Vertucci FJ et al., to study the morphology of lateral canals [3].
Dehydration with ascending gradient of alcohol: The dehydration process consisted of a series of rinses with ascending concentrations of ethyl alcohol (Rankem, Maharashtra, India), starting with 80% solution overnight, followed by 90% solution for an hour and 100% solution for an hour.
Staining with dye: Diluted India ink (CDH, New Delhi, India,) was injected into the pulp chamber with a number 27 gauge needle on a Luer-Lok plastic, disposable syringe (Atico Medical Pvt., Ltd., Ambala, India). The ink was drawn through the canal system by applying pressure at the apical-third using chair-side suction. This helps the dye to penetrate into minute details of pulp structure. The appearance of the dye at the apical end indicated the end of the process. The excess ink was removed from the root surface with gauze soaked in 100% ethyl alcohol.
Clearing with methyl salicylate: Samples were then placed in 100% methyl salicylate (CDH, New Delhi, India) for another two hours for complete clearing.
Stereomicroscopic evaluation: Each tooth was vertically sectioned in a buccolingual direction through the furcation, to separate the mesial and distal halves. Sectioning was done to avoid the overlapping of mesial and distal or distolingual roots during examination under stereomicroscope (Alco Steriozoom microscope Model CD 500A, Made in India Ambala). The root length was measured using Verniercallipers (Mapra Q1, India) and the apical third was marked. The root canal configuration in each root was examined under stereomicroscope and classified according to the number of canals in the apical third [Table/Fig-1]. Prevalence of number of canal at apical third was evaluated. Further prevalence of type of configuration in relation to number of canals in each root was evaluated. Comparative evaluation of prevalence of one, two, three and four canals at apical third of mesial and distal root of mandibular first molar were done.
Teeth with fused roots were observed from both mesial and distal aspects without splitting them into two.
Statistical Analysis
The data collected was tabulated using Microsoft Excel program and statistically analysed using the Statistical Package for Social Sciences (SPSS) software version 22. Since it was qualitative analysis, prevalence of configuration types was calculated and expressed as percentage. Chi-squared test was applied to compare the prevalence of one, two, three and four canals in mesial and distal roots. Statistical significance was considered for p<0.05.
Results
Number of roots: Two roots were observed in 227 samples (90.8%), three in 15 samples (6%), four in 5 samples (2%) and fusion between roots in 3 samples (1.2%) [Table/Fig-2]. Third root in three rooted molar was named as (E). Among four rooted molar two mesial roots were labeled as M1 to main root and M2 to accessory root. Similarly D1 to main distal root and D2 to accessory root.
Frequency distribution of mandibular first molar root types in the study sample.
| Root type/number | n (%) |
|---|
| Fused roots | 3 (1.2) |
| Two roots | 227 (90.8) |
| Three roots | 15 (6) |
| Four roots | 5 (2) |
| Total | 250 (100) |
Canal configurations (numbers) in the apical third: In the mesial root, two canals (48.4%) in the apical third was most prevalent, followed by one (25.8%), three (14.7%) and four (11.1%) canals. In the distal root, one canal in the apical third (74.2%) was the most prevalent finding followed by two (21.8%), four (2.8%) and three (1.2%) canals [Table/Fig-3,4]. The difference in prevalence of canal numbers in the apical third of the mesial and distal roots was statistically significant [Table /Fig-5].
Frequency distribution of one, two, three and four canals at apical-third of mesial root of mandibular first molar.
| Number of canals | Two-rooted molars (%) | Three-rooted molars (%) | Four-rooted molars (%) n=5×2*=10 | Total |
|---|
| One | 44 (19.4) | 12 (80) | 9 (90) | 65 (25.8) |
| Two | 118 (51.9) | 3 (20) | 1 (10) | 122 (48.4) |
| Three | 37 (16.3) | - | - | 37 (14.7) |
| Four | 28 (12.3) | - | - | 28 (11.1) |
| Total | 227 | 15 | 10 | 252 |
*2 represents the number of mesial roots in 4 rooted teeth
Frequency distribution of one, two, three and four canals at apical-third of distal root of mandibular first molar.
| Number of canals | Two-rooted molars (%) | Three-rooted molars (%) | Four-rooted molars (%) n=5×2*=10 roots | Total (%) |
|---|
| One | 162 (71.4) | 15 (100) | 10 (100) | 187 (74.2) |
| Two | 55 (24.2) | - | - | 55 (21.8) |
| Three | 3 (1.3) | - | - | 3 (1.2) |
| Four | 7 (3.0) | - | - | 7 (2.8) |
| Total | 227 | 15 | 10 | 252 |
*2 represents the number of distal roots in 4 rooted teeth
Comparative evaluation of prevalence of one, two, three and four canals at apical third of mesial and distal root of mandibular first molar.
| Mesial root (n=252) | Distal root (n=252) | p-value |
|---|
| One Canal | 65 (25.8%) | 187 (74.2%) | 0.0001 (HS) |
| Two Canal | 122 (48.4%) | 55 (21.8%) | 0.0001 (HS) |
| Three Canal | 37 (14.7%) | 3 (1.2%) | 0.0002 (HS) |
| Four Canal | 28 (11.1%) | 7 (2.8%) | 0.026 (S) |
*p<0.05 consider statistically significant, S: significant; HS: Highly significant, Chi-square test was used for finding the significant difference.
1. Two-Rooted Mandibular First Molars
a) Mesial Root
Configuration types with one canal in the apical third [Table/Fig-6,7]: The mesial root of 44 samples (19.4%) exhibited one canal in the apical third. Five different root canal configurations were observed in these samples.
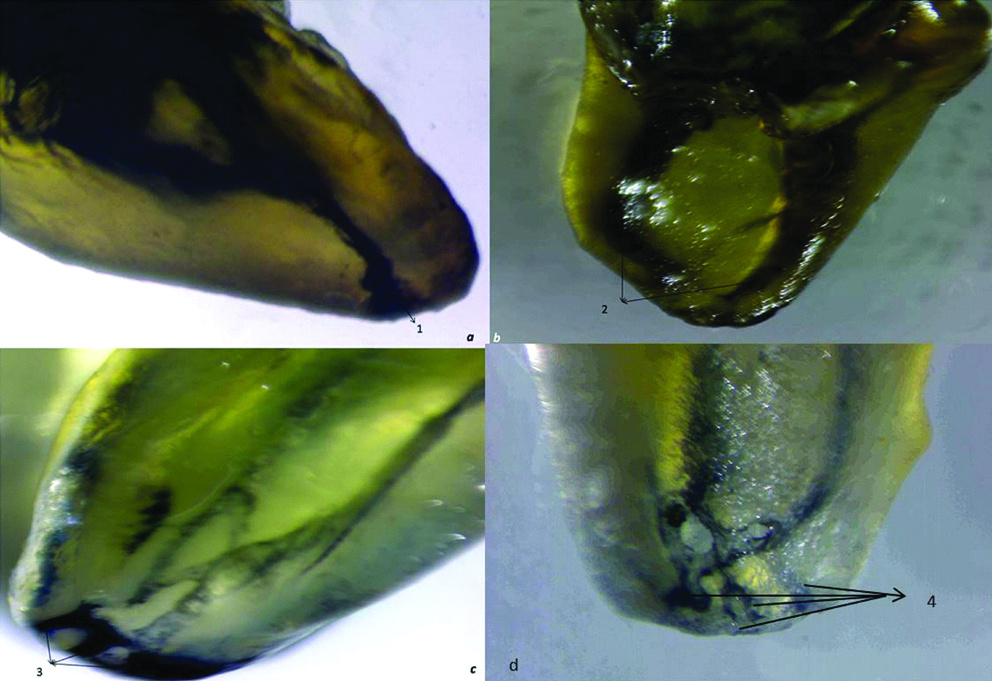
The mesial roots of mandibular first molar samples showing single: (a) double; (b) triple; (c) and four canals; (d) exiting at the apex.
Frequency distribution of single canals at apical-third of mandibular first molar roots.
| Root number/type | Root | Type I (1-1) n (%) | Type II (2-1) n (%) | Type III (1-2-1) n (%) | G-Type I (3-1) n (%) | S-Type XII (2-3-1) n (%) | Total |
|---|
| Fused root (n=3) | | | | | | | |
| Two roots (n=227) | M | 4 (1.8) | 37 (16.2) | 1 (0.4) | 1 (0.4) | 1 (0.4) | 44 (19.4) |
| D | 88 (38.8) | 74 (32.6) | - | - | - | 162 (71.4) |
| Three roots (n=15) | M | 1 (0.7) | 11 (73.3) | - | - | - | 12 (80) |
| D | 14 (93.3) | 1 (6.6) | - | - | - | 15 (100) |
| E | 15 (100) | - | - | - | - | 15 (100) |
| Four roots (n=5) | M1 | 2 (40) | 2 (40) | - | - | - | 4 (80) |
| M2 | 3 (60) | 2 (40) | - | - | - | 5 (100) |
| D1 | 5 (100) | - | - | - | - | 5 (100) |
| D2 | 5 (100) | - | - | - | - | 5 (100) |
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration
Configuration types with two canals in the apical third [Table/Fig-6,8]: Two canals were observed in the apical third of the mesial root of 118 samples (51.9%). Six different root canal configurations were observed in these samples. They were also observed in non-classifiable configuration types also.
Frequency distribution of two canals at apical-third of mandibular first molar roots.
| Root number/type | Root | Type IV (2-2) n (%) | Type V (1-2) n (%) | Type VI (2-1-2) n (%) | Type VII (1-2-1-2) n (%) | G-Type II (3-2) n (%) | G-Type V (4-2) n (%) | N 2-3-2 n (%) | N 3-1-2 n (%) | Total |
|---|
| Fused root (n=3) | - | - | - | - | - | - | - | - | - | - |
| Two roots (n=227) | M | 94 (41.4) | 3 (1.3) | 4(1.8) | 1 (0.4) | 13 (5.7) | 1 (0.4) | 1 (0.4) | 1 (0.4) | 118 (51.9) |
| D | 42 (18.5) | 13 (5.7) | - | - | - | - | | | 55 (24.2) |
| Three roots (n=15) | M | 2 (13.3) | - | - | - | - | 1 (6.7) | | | 3 (20) |
| D | - | - | - | - | - | - | | | - |
| E | - | - | - | - | - | - | | | - |
| Four roots (n=5) | M1 | 1 (20) | - | - | - | - | 1 (20) | | | 2 (40) |
| M2 | - | - | - | - | - | - | | | - |
| D1 | - | - | - | - | - | - | | | - |
| D2 | - | - | - | - | - | - | | | - |
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; N: New configuration
Configuration types with three canals in the apical third [Table/Fig-6,9]: The root canal exited as three canals in the apical third of the mesial root of 37 samples (16.3%) Five different root canal configurations were observed in these samples.
Frequency distribution of three canals at apical-third of mandibular first molar roots.
| Root number/type | Root | Type VIII (3-3) n (%) | G-Type III (2-3) n (%) | S-Type IX (1-3) n (%) | S-Type XIII (1-2-1-3) n (%) | S-Type XVI (2-3) n (%) | P-Type (1-2-3) n (%) | A-Type XXIII (3-2-3) n (%) | N-Type (4-3) n (%) | Total |
|---|
| Fused root (n=3) | - | - | - | - | - | - | - | - | - | - |
| Two roots (n=227) | M | 18 (7.9) | 5 (2.2) | 3 (1.3) | - | 8 (3.5) | 1 (0.4) | - | 2 (0.8) | 37 (16.3) |
| D | 1 (0.4) | - | - | - | 2 (0.8) | - | - | - | 3 (1.3) |
| Three roots (n=15) | M | - | - | - | - | - | - | - | - | - |
| D | - | - | - | - | - | - | - | - | - |
| E | - | - | - | - | - | - | - | - | - |
| Four roots (n=5) | M1 | - | - | - | - | - | - | - | - | - |
| M2 | - | - | - | - | - | - | - | - | - |
| D1 | - | - | - | - | - | - | - | - | - |
| D2 | - | - | - | - | - | - | - | - | - |
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration; P: Peiris configuration; A: Al-Qudah and Awawdeh configuration; N: New configuration
Configuration types with four canals in the apical third [Table/Fig-6,10]: Four canals were observed in the apical third of the mesial root of 28 samples (12.3%). Three different root canal configurations were observed in these samples.
Frequency distribution of four canals at apical-third of mandibular first molar roots.
| Root number/type | Root | G-Type VI (4-4) n (%) | G-Type VII (5-4) n (%) | S-Type XI (1-2-3-4) n (%) | N-Type (2-4) n (%) | S-Type XXIII (3-4) n (%) | Total |
|---|
| Fused root (n=3) | - | - | - | - | - | - | - |
| Two roots (n=227) | M | 7 (3) | 2 (0.8) | - | 13 (5.7) | 6 (2.6) | 28 (12.3) |
| D | 3 (1.3) | 1 (0.4) | - | 1 (0.4) | 2 (0.8) | 7 (3.0) |
| Three roots (n=15) | M | - | - | - | - | - | - |
| D | - | - | - | - | - | - |
| E | - | - | - | - | - | - |
| Four roots (n=5) | M1 | - | - | - | - | - | - |
| M2 | - | - | - | - | - | - |
| D1 | - | - | - | - | - | - |
| D2 | - | - | - | - | - | - |
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration; N: New configuration
b) Distal Root
Configuration types with one canal in the apical third [Table/Fig-7,11]: The distal root of 162 samples (71.4%) showed the presence of one canal in the apical third.
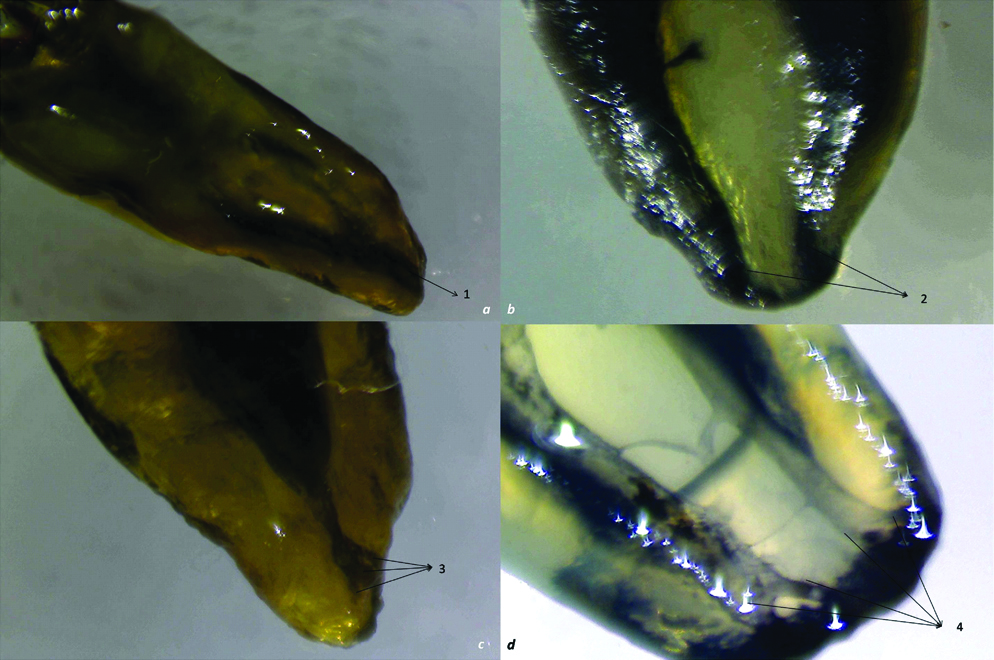
The distal roots of mandibular first molar samples showing single: (a) double; (b) triple; (c) and four canals; (d) exiting at the apex.
Configuration types with two canals in the apical third [Table/Fig-8,11]: Fifty-five (24.2%) samples showed the presence of two canals in the apical third of the distal root. Two different root canal configurations were observed in these roots.
Configuration types with three canals in the apical third [Table/Fig-9,11]: The distal roots of three (1.3%) samples exhibited the presence of three canals in the apical third. Two different root canal configurations were observed in these samples.
Configuration types with four canals in the apical third [Table/Fig-10,11]: The distal roots of seven samples (3.0%) had four canals in the apical third. Four different root canal configurations were observed in these samples.
2. Three-Rooted Mandibular First Molars:
a) Mesial Root:
Configuration types with one canal in the apical third: In the three-rooted molars, the canals in the mesial roots of 12 samples (80%) exited as one canal in the apical third. Two different root canal configurations were observed in these samples. They were Vertucci Types I (0.7%) and II (73.3%) [Table/Fig-7].
Configuration types with two canals in the apical third: Three (20%) samples showed root canals in the mesial root exiting as two canals in the apical third. Vertucci Type IV (13.3%) and Gulabivala Type V (6.7%) configurations were observed [Table/Fig-8].
More than two canals were not observed in mesial root of three rooted mandibular first molar [Table/Fig-9,10].
b) Distal Root and Third Root:
Both the distal and third roots of three-rooted molars in the sample showed the presence of canal configurations exiting as only one canal in the apical third. Vertucci Types I (93.3%) and II (6.6%) configurations were observed in the distal root, while in the third root only Vertucci Type I (100%) was observed [Table/Fig-7].
3. Four-Rooted Mandibular First Molars:
a) Mesial Roots:
Configuration with one canal in the apical third: Vertucci Type I and II configurations were observed in both mesial roots (M1 and M2) [Table/Fig-7].
Configuration with two canals in the apical third: Out of two mesial root of four rooted mandibular first molar in M1 root only two canals at apical third were observed. They appeared in two configuration types-Vertucci Type IV (20%) and Gulabivala Type V configuration (20%) [Table/Fig-8].
b) Distal roots:
In four rooted mandibular first molar there were two distal roots (D1 and D2). In both roots only one canal was observed at the apical third [Table/Fig-7].
4. Mandibular First Molars with Fused Roots
[Table/Fig-2] C-shaped configuration was observed in all three teeth with fused roots.
Many new configurations (N) not reported till now were observed in the study [Table/Fig-8,9 and 10].
Discussion
The mandibular first molar is a frequently-treated tooth. It generally has two roots, a mesial and a distal. In the present study, 90.8% of mandibular first molars had two separate roots. These results are in line with those of other studies from India [11,12], Italy [13] and Chile [14]. However, the prevalence of two-rooted molars in the present study was higher than that reported in Chinese [15] and Korean [16] populations.
The prevalence of three-rooted mandibular first molars in the present study was 6%. This finding is in agreement with the observation of Tratman E [17] who reported a 5% prevalence of three-rooted mandibular first molars in Europeans but higher than that reported in a south Asian Pakistani population [18] (2.3%) and less than that reported in Thai [19] (19%) and Chinese [15] (20%) populations.
Four-rooted mandibular first molars made up only 2% of the samples in the present study. There are few reports on four-rooted mandibular first molars. In an in-vitro study on a Japanese population, only 0.04% mandibular first molars were four-rooted [20]. Several elaborate studies have not reported the presence of four-rooted mandibular first molars [4,6,7]. A search of the literature reveals only two case reports of four-rooted mandibular first molars [21,22]. Further, in the present study, fusions between mesial and distal roots were observed in three teeth only (1.2%).
The complexity of root canal treatment is directly associated with the number of root canals and the position where splitting or merging may occur. A root canal splitting in the coronal or middle portion may be easy to locate and examine but an abrupt separation in the apical portion is difficult to manage [10,23,24]. Martins J et al., studied the location of merging of the main root canals in fused roots of molars and reported that, while merging occurred at all levels of the root canal, there was a higher incidence in the apical third [10].
Although prevalence of four canals in the apical third of mesial root of two rooted mandibular first molars was least common (11.1%), it was observed to have a new configuration Type 2-4 which has not been reported in literature to date. In this configuration, splitting of two canals was observed to occur in the apical third, which resulted in four canals. The findings of the present study differ from those reported by Torres A et al., who observed the most common configurations in the mesial root to be Vertucci Types III and V in their Belgian population [14]. This difference could be attributed to the difference in population types in the two studies.
In the distal root of two-rooted mandibular first molars, Vertucci Type I configuration was frequently observed in single canals, Vertucci Type IV in two canals, Sert and Bayirli Type XVI in three canals and Gulabivala Type VI in four canals.
Identification of Vertucci Types I, II, IV and VIII and Gulabivala Type VI configurations is relatively straightforward as each of the canals is separate and distinct between the orifice and the apex without splitting or merging during its course. Root canal preparation and obturation become more complicated when single canals split or merge in the apical third. Martins J et al., reported on splitting and merging of canals in a Caucasian population [10]. They observed splitting in the apical third in 3.2% of mesial roots and 1.8% of distal roots of first molars in their sample, and merging in the apical third in 30% of mesial roots and 6% of distal roots.
In the present study, the prevalence of complicated configurations was low but clinically significant. In mesial roots, a single canal at the apex resulting from merging of canals was observed in Vertucci Types II and III, Gulabivala Type I and Sert and Bayirli Type XII configurations. Similarly, Gulabivala Types II and V appeared as two canals and Gulabivala Type VII as four canals. In distal roots, merging of canals was less frequent and observed in Vertucci Type II as one canal at the apex and in Gulabivala Type VII as four canals at the apex.
Splitting of the canal in the mesial root was observed as two canals in Vertucci Types V, VI, VII and 3-1-2, as three canals in Gulabivala Type III, Sert and Bayirli Types IX and XVI and Peiris 1-2-3 configurations, and as four canals in Sert and Bayrili Type XXIII and new configuration 2-4. In distal roots splitting resulted in two canals in Vertucci Type V, three canals in Sert and Bayrili Type XVI and four canals in Sert and Bayrili Type XXIII and new configuration 2-4.
Configurations resulting from splitting of canals, such as Sert and Bayirli Types XVI (2-3) and XIII (1-2-1-3), Gulabivala Type III (2-3) etc., are less prevalent, but whenever they are encountered, they are one of the most challenging configurations to clean and disinfect. Vertucci FJ et al., observed that only 8% of a hundred mandibular molar samples showed the presence of the type V configuration in the distal root [3]. Similarly, in Type VII (1-2-1-2) configuration, canals divide into two twice and hence, it is difficult to negotiate the full working length in the apical third where the canal again splits into two. In Type VI configuration (cross-over configuration) two canals leave the pulp chamber, intersect as they progress in the middle or apical third and then re-divide short of the apex into two separate canals with two separate apical foramina. During cleaning and shaping, only one file at a time could pass through the root canal intersection.
In contrast with Vertucci’s observation that the percentage of human permanent teeth with Type III configuration is 0% for mandibular first and second molars, in the present study, Type III configuration was observed in one sample (0.4%).
In the present study, complex configurations were more commonly observed in two-rooted molars than in three-rooted molars. In three- and four-rooted mandibular first molars, simple configurations like Vertucci Types I, II and IV were observed. Vertucci Type I configuration was observed in the distobuccal and distolingual roots of all three-rooted mandibular molars in the present study. Similar observations were reported by Gu Y et al., who examined 20 extracted three-rooted mandibular first molars of a Chinese population by micro-computed tomography [25].
The only tooth reported in literature to show all types of Vertucci configurations is the maxillary first premolar [26]. In the present study, all eight Vertucci configuration types as well as many other configurations were observed in the permanent first molar. This may be due to variations in population type, method of evaluation and sample size.
Many methods have been used to investigate root canal anatomy in-vitro, each having its own advantages and disadvantages and with variable degrees of accuracy and procedural complexity. Of these, the most detailed information can be obtained by demineralisation and clearing technique. In this study clearing technique provided a three-dimensional view of pulp cavity towards the outside of the tooth. Recent studies also reported clearing technique as an excellent procedure to observe root canal morphology [27-31].
The pulp canal system is complex, with canals branching, dividing and rejoining. Vertucci’s classification was proposed several years ago based on results from his study of an American population. Canal configurations vary with geographical distribution as is reflected in the new, hitherto unreported anatomical configurations 2-3-2, 3-1-2, 4-3 and 2-4 observed in the present study. These configurations are unclassified by existing system. Hence there is a need in modification of existing classification system as reported in review article [32]. In such a scenario, gender, racial and ethnic aspects must be considered in the pre-treatment evaluation for root canal procedures. Complex configuration were prevalent as Sert and Bayirli Type XII (2-3-1), Gulabivala Type VII, Vertucci Types VI, VII, Peiris 1-2-3 as merging configuration. Vertucci Types VI, Sert and Bayirli Types IX, Sert and Bayrili Type XXIII configurations were observed as splitting configuration. In this study, configuration due to merging and splitting of canals were equally prevalent in mandibular first molars.
Complex root canal configurations with more than one canal and involving merging or splitting of canals at the apical third pose a challenge to the clinician aiming to achieve this. A root canal splitting in the coronal or middle portion may be easy to locate and examine but an abrupt separation in the apical portion is difficult to manage. The main aim of endodontic treatment is the prevention or treatment of apical periodontitis. Three-dimensional seal at the apical third is crucial for successful endodontic treatment. However, complex root canal configurations with more than one canal and involving merging or splitting of canals at the apical third pose a challenge to the clinician aiming to achieve this. A sound knowledge of such complex configurations can greatly help in favourable treatment planning. Careful pre-operative evaluation using angled radiographs and 3D imaging is must in order to diagnose canal configuration.
Limitation
Clearing technique is a traditional technique to study root canal morphology. Still it is considered gold standard [19]. It gives detailed information on root canal morphology if samples are handled carefully during demineralisation and dehydration. Dye penetration under suction allows evaluation of canal course from orifice to apex. However, this technique cannot be used clinically. Further in-vivo studies are required to evaluate prevalence of root canal configuration types based on number of canals at apical third of mandibular first molar roots.
Conclusion
Two rooted mandibular first and second molars are prevalent in Indian population. Three and four rooted mandibular first molar also exist in the population. In mesial root of mandibular first molar two canals at apical third are more prevalent. In distal root of mandibular first molar one canal at apical third is prevalent. Three to four canals at apical third also exist in mandibular first molar. In both mesial and distal root simple tubular configurations like Vertucci Type IV (2-2), Vertucci Type VIII (3-3) are prevalent. Configurations in extra root of mandibular first molar are simple tubular. All configurations types cannot be classified by currently available classification system.
*2 represents the number of mesial roots in 4 rooted teeth
*2 represents the number of distal roots in 4 rooted teeth
*p<0.05 consider statistically significant, S: significant; HS: Highly significant, Chi-square test was used for finding the significant difference.
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; N: New configuration
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration; P: Peiris configuration; A: Al-Qudah and Awawdeh configuration; N: New configuration
M, M1, M2: Mesial roots; D, D1, D2: Distal roots; G: Gulabivala additional configuration; S: Sert and Bayirli configuration; N: New configuration