Experiential learning in its simplest form means learning from experience or learning by doing. Experiential education first immerses learners in an experience and then encourages reflection about the experience to develop new skills, new attitudes, or new ways of thinking [1]. Thus, it stresses the importance of experience and reflection, while also requiring the participant to be active in their learning. The experiential learning theory was developed by Kolb D, and stems from the work done by Dewey, Lewin, and Piaget [1]. According to Kolb D, Knowledge results from the combination of grasping experience and transforming it. Kolb model identifies the four different kinds of abilities present in all learners: concrete experience, reflective observation, abstract conceptualisation, and active experimentation. He stressed that in order for learning to occur the student must exercise all four of these abilities [1]. Harb J et al., broke down the learning model into quadrants and developed a list of specific classroom learning activities [2].
Basic epidemiology is a requirement of all students of life sciences and public health. Due to didactic teaching methods mostly concentrating on a theoretical framework, students tend to lose interest in learning epidemiology. Epidemiology in itself is complex nature as population level thinking is not easy. Teachers teach epidemiology in discrete units and ensure the student is competent in that part. We ensure that students are competent with regard to each piece of information, requiring students to memorize lists of study strengths and limitations, rules for assessing confounding, and the definitions of concepts like misclassification. Teachers fail to unify the concepts and make the student understand how the whole epidemiology works together. This runs the risk of eliding the fundamental commonalities of epidemiological approaches. Students are not able to link epidemiology with clinical subjects or day to day practice. This will hamper the research quality and create evidence. There is a risk of low motivation, poor performance in the exam. Basic epidemiology is a basis of clinical epidemiology and Evidence-Based Medicine (EBM) so the experiential learning was included in this study to teach epidemiology to medical undergraduates so that they get a broader perspective and become a lifelong learner.
Therefore, authors planned to introduce experiential learning as a new teaching methodology in epidemiology. This study was carried out to assess the effectiveness of teaching epidemiology using experiential learning method for undergraduates with the specific objective to develop interest among students in learning epidemiology, to substantiate the satisfaction of students with experiential learning in terms of learning outcome, relevance, extrinsic motivation, attitude and overall satisfaction. Also, authors need to assess the difference in the competency of a student in integrating the gained knowledge for problem-solving, exposed to experiential learning and those exposed to traditional lecture approach. A sequential explanatory mixed method approach was employed in order to explain the results of quantitative data (i.e., improvement in knowledge, skill and competency) with subjective feeling and perception of students related to experiential learning.
Materials and Methods
A sequential explanatory mixed method study was planned in All India Institute of Medical Sciences, Rishikesh in July 2017-December 2017. Assuming 5% alpha error and fixed finite population of 50 students, the sample size comes to be 44 in total [3].
An educational intervention was planned by introducing experiential learning to one batch of 25 students posted for clinical posting. Next sequential batch posted were exposed to traditional teaching method with some problem-solving exercises. An exemption from the review was obtained from the Local Ethics Committee (IEC code. 31/IEC/IM/NF/2017 letter no. AIIMS/IEC/17/122). An informed consent was taken prior to the start of the educational intervention. All the students in batch gave the consent to experiment with new learning methodology.
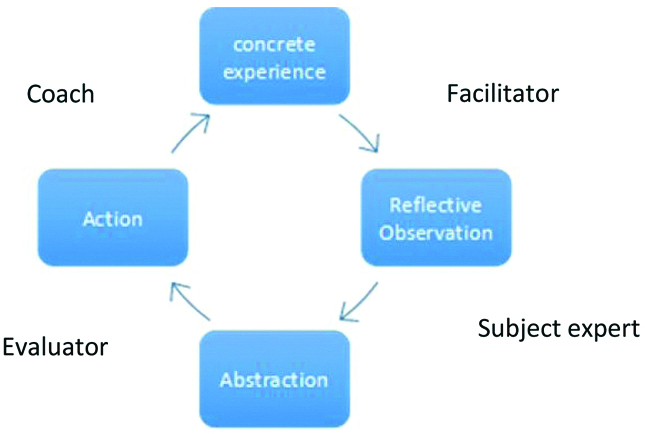
Priority topics were selected after brainstorming with five faculty members of which two were the researchers of the study and three were external members. These topics were concept of epidemiology, measurements in epidemiology, study designs, ecological, case study and case series, descriptive, case-control, cohort and experimental, Measures of association, confounding and bias, outbreak investigations. A classroom-based experiential learning methodology, encompassing action, reflection, analysis, and application for each topic was planned accordingly and a module was prepared. After this preparation, the students and facilitators were oriented to new learning methodology and reflection in two-hour session. Then with the help of experiential learning module, the teaching was carried out that took around 12 days with two hours per session. The students were given an individual/group task in the phase of concrete experience. Then they take a break or time out, review what has been done and experienced, and give feedback to teachers and students. In the phase of abstract conceptualisation, the student tries to read a material or listen to the lecture of teacher and link the theory to situations. At the final stage, the student tries to solve the same problem or new projects, fieldwork, case study, simulations etc with gained knowledge by either refining or revising the ways to solve the task [4]. However, this sequence is not fixed and students can enter into the cycle at any stage depending on the topic and learning style and complete the logical sequence as said by Kolb [5]. To make the learning to be effective the student should go through all the four stages. Therefore, the sequencing in the sessions was tailor-made to suit the entire batch. As the student move from one phase to another, teacher had to adopt varying roles. From concrete experience to reflection, the teacher’s role was as a facilitator. From reflection to abstraction phase, the teacher acted as a subject expert, making the connection between what they have experienced and observed. From abstraction to action, the teacher’s role was evaluator or setter sharing with students the goals they need to achieve and the right answers. Moving from action to experience, teacher acted as a coach helping the student to apply the knowledge back into the experience [Table/Fig-1]. The details of each session are given in [Annexure 1].
Role of teacher in various phases of the learning cycle.
Sequential next batch (25 students) was exposed to traditional lectures with some problem-solving exercises as appropriate at the end of class. The lectures were on the same topic as in earlier batch of experiential learning with the help of PowerPoint presentation and interaction during problem-solving exercises. These exercises were related to the calculation of various rates, ratio, proportions, measures and strength of associations. It was also carried out in 10 sessions, two hours per session. For quantitative data, the direct evidence of learning outcome was assessed by Multiple Choice Questions (MCQ) consisting of knowledge or recall type, 10 questions one mark each and higher order (analytical and problem-solving type) 30 questions, one mark each administered to both the group at completion of epidemiology. Further to get more in-depth insight into the experiences of the student in this new learning methodology and to explain the findings of quantitative data, a qualitative approach was undertaken. Students were told to give feedback on experiences with experiential learning on self-constructed five-point Satisfaction scale questionnaire. The 12 items were generated after brainstorming with all researchers for various items related to satisfaction with learning experiences. These items were later grouped into four factors viz., perceived learning outcome, relevance, affective attitude, and course satisfaction. Each factor comprised of three items amounting to overall 12 items. The composed scale was unidirectional. Each item was rated on the seven-point Likert scale, 1 being strongly disagreed to 7 strongly agreed. Two faculties trained in medical education did the face validity of the scale. Cronbach alpha was used to assess reliability. Cronbach alpha for perceived learning outcome, relevance, affective attitude, and course satisfaction was 0.83, 0.823, 0.92 and 0.89 respectively which means the items were consistent with each other as a group. Written reflections on Driscoll (Barton) model was also invited at the end of the topic from the interventional group only [6]. It consisted of simple questions like What, so what and now what. Having experienced a new learning, the student first had to describe the event. Then they reflected on the experiences and analysed and examined their new learning. In the last question now what, the student listed down the proposed action in the purview of new learning gained.
Statistical Analysis
Data were analysed by MS-Excel 2016 and SPSS version 23. For comparing the marks obtained in two groups nonparametric Mann-Whitney U-test was used. A p-value less than 0.05 were considered to be a significant difference. Satisfaction scale was analysed by the proportion of student rating each item. Reflections from students were analysed qualitatively by content analysis. Two independent researchers analysed the written reflection and any discrepancies were resolved by discussion. Then the contents were coded and categories assigned [7].
Results
The module took around 10 days with two hours for each session. Though each of batches was of 25 students, only 22 students were present during the final assessment in experiential learning group and 20 students in the group exposed to traditional lecture with problem-solving exercises. Absent students were excluded from analysis.
The [Table/Fig-2] shows all students (22) those exposed to experiential learning in epidemiology score more than 70% in MCQ knowledge-based while in another group only 10 students (50%) scored more than 7 (70%) marks. So this is the highly appreciable result. Out of 10 maximum marks mean score±SD was 8.18±1.0 and 6.9±1.8 respectively in experiential and lecture group respectively.
Distribution of no of students and marks obtained in MCQ level 1.
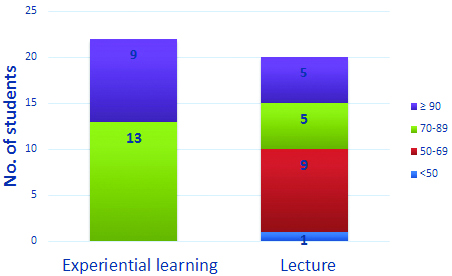
Independent sample Mann-Whitney U Test is significant at 0.014 levels.
The [Table/Fig-3] shows 16 students (72%) score >21 (70%) marks in MCQ Level 2 (analytic and knowledge-based) and only one student score <60% in an experiential learning group. In another group, only one student score more than 70% while all others scored lower. Out of 30 maximum marks, the mean score was 22.22±2.4 and 14.65±4.2 in experiential and lecture group respectively.
Distribution of no of students and marks obtained in MCQ level 2.
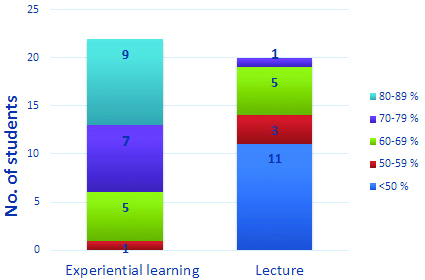
Independent sample Mann-Whitney U Test is significant at ≤0.001 levels so those exposed to experiential learning scored higher than exposed to lecture.
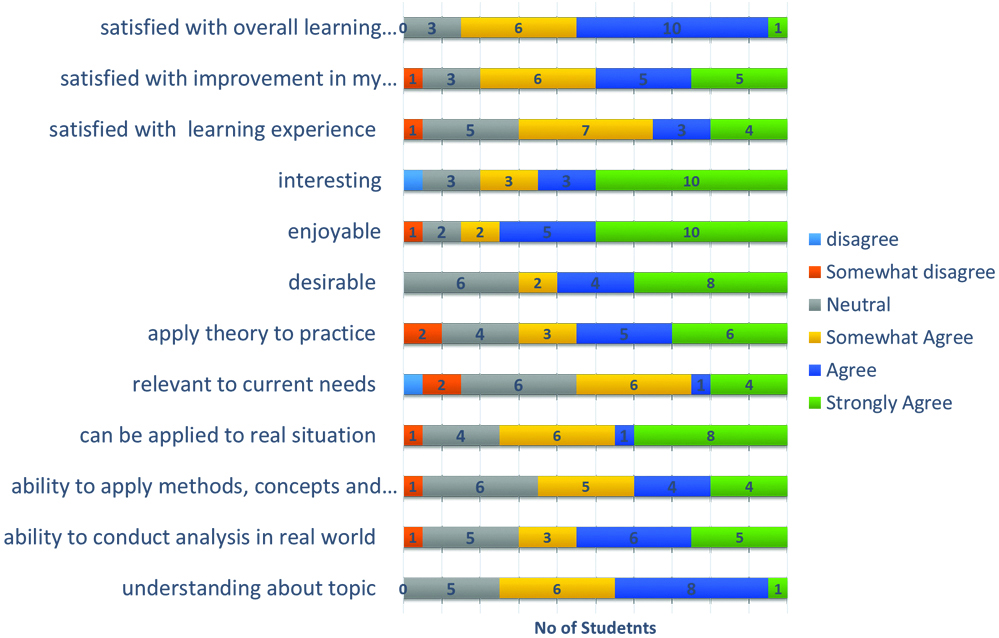
The [Table/Fig-4] shows student views of the experiential learning in epidemiology. Fifteen students perceived methodology to be effective in a good understanding of the topic. Fourteen students were of opinion that the experiential learning had given them the experience to apply the new knowledge in real field scenario. Thirteen students had confirmed that they applied the methods, theories, and concept of epidemiology in problem solving. Fifteen agreed that teaching can be applied to the real situation but still only 11 were of opinion that epidemiology teaching is relevant to current need or can be applied in real practice. 14-17 students found it to be desirable, enjoyable and interesting. Overall 14 (70%) were satisfied with a learning experience, 16 with improvement in their learning and 17 were of opinion that experiential learning was effective.
Student Views of the experiential learning.
Qualitative Analysis of Written Reflection
Total 23 students had written the reflections which were analysed here with an objective to understand the perception of a student regarding experiential learning and whether it was successful in developing an interest in learning epidemiology.
The [Table/Fig-5] shows 12 subcategories emerged while analysing the data which was reduced to four main categories. The first category was what happened during experiential learning (Input), Second was how did student experience learning (Process), Third consisted of the yield of experiential learning and fourth was the student’s opinion regarding the inclusion of experiential learning in the curriculum.
Coding tree of reflection.
| Codes | Subcategories | Main categories |
|---|
Basics of epidemiological studies A systematic approach to studies Risk factors for disease Epidemiological triad Sampling Sensitivity and specificity Outbreak investigations
| Content taught | What happened |
Active participation Raise own ideas, queries solved Brainstorming on issues Break monotony Creative group activities Faculty facilitated the understanding Increased confidence and morale Team building
| Aid of experiential learning |
Effective learning Interesting Helpful in future Interesting than books Lifetime experience Simple, easy to understand and apply
| Experience with learning | Overall experience and environment (Process) |
Enjoyable Interactive Friendly
| Learning environment |
Clearly understanding of basic concepts
| Output (Knows) | Yield |
Analyse the diagnostic test and its values Management of disease at community and individual level Community needs assessment Analyse risk factors and prioritisation
| Know how |
Do sampling Conduct epidemiological studies Apply knowledge gained in thereal field Outbreak control
| Show how |
Boring topic to interesting Motivation Disease can be controlled by applying the epidemiological knowledge
| Change in attitude |
Develop intellectual Thinking Application of learned theory to real world Change perspective of learning epidemiology Generate new ideas innovative ways Improved understanding Deep knowledge Motivated further learning
| Outcome |
Study (Epidemiology) can be made enjoyable and interesting
| Impact |
Create interest Clear understanding Higher level of learning Discourage mugging up
| Favor of inclusion in the curriculum | Perception of inclusion |
Not suitable for current theory based curriculum Time-consuming
| Barriers to inclusion |
When prompt about what happened students gave a brief of all the content they learned during the session with the help of the experiential method.
“I learned a systematic approach to epidemiology studies” (Interviewee 21, m)
“I learned three parameters that need to be considered while studying, Agent, host environment, study designs, sampling methods etc.,”
All the students were of opinion that experiential learning helped them to learn better.
“This kind of learning made me participate in activities which helped me to raise my own ideas, queries and get them solved.”
“…… creating groups and having a discussion at the end was very creative”
“There was active participation of every student s learning was fun and not monotonous”
All students find it effective and very interesting. One student quoted it as a lifetime experience. “We enjoyed it a lot simultaneously learned a lot in a slightly different manner”. Friendly and non-coercive learning environment helped students to actively involved in problem-solving, generate ideas etc.
Finally, the students were able to meet the learning objectives at know, knows how, shows how level. “There were some concepts about relative risk, odds ratio which we applied in the present study and how to know which factor contribute to disease”.
We performed a study on stress, found the risk factors and finally performed a short intervention that can be done to prevent stress”.
“We learned of how to make a hypothesis and how to test it by feature studies”. This output was further assessed by MCQ’s after a week of the session already mentioned in quantitative analysis.
Most of the student (15) said that it made them think and develop the intellectual thinking.
“In-depth knowledge of epidemiology was ascertained by mixing theory with practical near, real field setting.
“We learned about sensitivity and specificity of the test and how to apply the concept in clinical practice, whether to rely on a test or not and how much.”
Finally, all the students enjoyed the sessions.
“This new learning technique changed the perspective of studying epidemiology by making it more enjoyable.”
Twenty were of opinion that this need to be included in regular studies for some important topics. However, four students were of opinion that it was time-consuming. Also, as present medical curriculum is mostly theoretical so for writing a full long answer, mugging up needs to be done. In spite of having a good understanding of the practical application, this will not help in theory test. A student recommended.
“However, this type of study not theory based curriculum, for that lectures should be supplemented with these approach in practical classes. If properly implemented will not consume much time.”
Discussion
Many medical universities have incorporated experiential learning through practicum and internship. The present study is only one study that involves classroom experiential learning with the multi-method approach in epidemiology as a whole. It has been observed through personal and colleagues’ perception that there is a loss of students learning epidemiology. The main reason for the loss of interest is due to the perception of students like content is irrelevant to clinical practice, passive learning with no input from students, perceived being toughest part in medicine and theoretical approach of teaching.
Therefore, the experiential education has incorporated that stress on education to meaning, relevance and active participation from students. Through qualitative and quantitative inquiry it was found that student demonstrated an interest in learning epidemiology. All of them found it to be an enjoyable, interactive and non-threatening environment to learn. It helped them to broaden their perspective regarding the use of epidemiology in real life. Many studies in science in past had demonstrated that students learn more deeply when given a learning opportunity which addresses real-world problems and classroom teaching that promotes experiential education has been shown to promote higher order thinking skills in students [8-12]. The students’ gave a favourable score on perceived learning outcome, relevance, attitude and overall satisfied with the course.
Simon L et al., studied experiential learning in psychology for undergraduates also confirmed that students developed a deeper understanding of the psychological content and acquired interpersonal and multicultural skills. Students also gained professional knowledge about workplace behaviours and were better prepared for future work or graduate school [13]. Healey M and Jenkins A, had shown how the Kolb theory could be applied to whole degree programme of universal geography [14]. Experiential learning teaches the student to be a culturally competent thinker. It is an effective method to strengthen the community and university partnership and building the relationship with local community and agencies [13,15,16]. If the students go regularly to the field practice area for epidemiology class then along with students, community, local organisations will be benefitted. The institution can deliver its basic health care services through these students and further strengthen the partnership.
No studies compared the experiential teaching with traditional teaching until date. In the present study students exposed to experiential learning scored higher than another group in MCQ test conducted for knowledge or recall type as well as problem-solving or analytical type. Thus the interest in learning motivated them for self-directed learning, get an in-depth understanding of the subject and at last able to efficiently solve the test imparted. This further led to an increase in overall satisfaction of students.
Being a new and unexplored method of teaching in epidemiology authors reflected on their own experiences so that could help other researchers or educationalist. It needed skilled facilitators and preparedness. Class of 25 students needs three to four facilitators. It can be effectively done in small groups only. Time was another challenge. At least two hours’ session is needed at a time. It will take more than 24 hours of teaching-learning sessions. Authors propose to utilise the tutorials or community postings for epidemiology classes through an experiential learning approach. The student needs to realise the importance of learning Epidemiology in not only community medicine but also in future to clinical practice or research work.
Limitation
Due to short-term nature of project, only two batches could be included in the study. Therefore, the result of this setting could not be generalised to other settings. Change in facilitators may increase or decrease the effectiveness. Further study can be taken to include more batches and different settings for the effectiveness of module on experiential learning in epidemiology. Non-randomisation of students in two groups may have affected the difference in knowledge and skill due to other potential confounders. However, on basis of qualitative data, authors can state that experiential learning brings new promise to epidemiology in creating interest among students and reproducible in other settings.
Conclusion
Overall the Experiential learning in epidemiology build excitement in the classes, relate the information on a personal level, and provide in-field learning experiences. Students perceived to have left feeling a greater sense of connectedness to their learning in the classroom. Experiential education activities provide an effective alternative for teaching epidemiology in terms of producing measurable outcomes as in the present study.