Quality of Life (QoL) is a multidimensional concept, including the functional ability, health, and psychological state of the individuals, which is influenced by many important factors such as the physical and mental status, personal belief, and social relationships [1,2]. Job has been identified as one of the affecting factor on the QoL [3]. Although job is a very important source of livelihoods and a means of acquiring social positions, it can also lead to dissatisfaction and degradation of the physical and mental forces. The workplace may be full of physical, psychological and social stimuli, each of which can be a stress factor and these stressors may have negative impact on physical well-being (individual’s health and performance) and psychological well-being [4,5].
The Quality of Working Life (QWL) includes individuals’ feelings about all aspects of their work, such as the financial rewards, job benefits, job security, comparing their job conditions with the employees of other organisations, working conditions, career development opportunities, decision-making power, relations with their colleagues and with the organisation [6,7].
Health system reform has been the topic of interest all over the world, especially developing countries, over the past decades. Nurses are considered to be the integral and important part in any health system [8]. Among all the human resources employed in a hospital, nursing staff is of great importance due to the provision of health care for patients and being in direct communication with patients. Delivery of the optimal nursing services is associated with the quantity and quality of nurses’ work in the hospital [9]. At present, there is a shortage of health-care workers in the health system. The widespread shortage of nurses and also the high level of turnover among nurses have become a global issue [10]. The shortage of nursing workforce reduces the positive mood of the remaining workforce and increases stress caused by the high level of workload and ultimately leads to changes in the behaviour of nurses towards their jobs. Among these changes are the low level of job satisfaction, low level of productivity, high level of cognitive failure and eventually quitting the organisation [11-14].
In the United States, between 44,000 and 98,000 people die annually in the hospitals as a result of medical errors [15]. Despite the efforts made in the fields of appropriate education and employment of nurses, we are still struggling in this area. Therefore, improving the organisational effectiveness, strengthening the organisational commitment of employees, and reducing turnover in nurses is of great importance in the health system [6].
Workload, which is defined as the total amount of work that must be done by a person or a group of people over a given time period, is high among nurses and hospital staff [16]. High workload has been reported to be as one of the main sources of occupational stress among the nurses working in the Intensive Care Units (ICUs) [17,18].
Furthermore, some issues such as getting a second job, the working unit, monthly income, age, and work experience are other factors that affect the QoL of nurses [11,19-21]; each of which has independent or interactive effects on job satisfaction and QWL.
The present study aimed to investigate the interactive effects of background variables (job and demographic characteristics) and workload parameters on the WRQoL among 840 nurses working in highly complex hospital units including the Emergency Departments (EDs), Intensive Care Units (ICUs) and Coronary Care Units (CCUs) of the hospitals affiliated to Tehran University of Medical Sciences, Tehran, Iran.
Materials and Methods
This was a cross-sectional study conducted in 2017 among all male and female volunteer nurses (n=840) working in hospital units including EDs, ICUs and CCUs of the hospitals affiliated to Kermanshah University of Medical Sciences. This study received ethical approval from research ethics committee of Kermanshah University of Medical Sciences and all the subjects signed an approved consent form from issued by this committee.
The NASA-Task Load Index (NASA-TLX) (Version. paper and pencil) was used to determine the workload of the subjects. The WRQoL scale was applied to determine the QWL. A general questionnaire was also used to collect the job and demographic information of nurses. The questionnaires were distributed among volunteer nurses and the method of completing the questionnaires was explained. Nurses were asked to return the completed questionnaires. The process of data collection lasted for three months from March through July 2017. A brief description of the questionnaires is presented below.
NASA-Task Load Index (NASA-TLX)
The NASA-TLX is a multi-dimensional assessment tool which evaluates the perceived workload in order to assess a task, system, or team’s effectiveness or other aspects of performance [22]. The NASA-TLX originally consisted of two sections; the total workload which is divided into the six sub-scales, serving as the first part of the questionnaire:
Mental demand
Physical demand
Temporal demand
Performance
Effort
Frustration
There are explanations for each of these sub-scales which the subject should read before rating. They are rated for each task within a 100-points range with 5-point steps. These ratings are then combined to the Task Load Index (TLX). In second section of TLX these subscales allow subjects weighing them by pairwise comparison based on the perceived importance of those. This requires the user to choose which measurement is more relevant to work. The number of times each is chosen is the weighted score. This is multiplied by the scale score for each dimension and then divided by 15 to get a workload score from 0 to 100, which is the overall TLX [23,24]. The reliability and validity of the Persian version of this questionnaire was evaluated by Mohammadi M et al., in a study on nurses’ workload (a=0.897) [23].
Work-Related Quality of Life (WRQoL) Scale
In this study, the 23-item WRQoL scale, developed by Van Laar D et al., was applied to assess the QWL [25]. This scale uses six main components to measure the QWL of employees: career and job satisfaction, work conditions, general well-being, work-life balance, stress at work, and control at work. The questions are on 5-point Likert scale with the total score range of 0-100 in each category. The higher total scores represent the higher level of QoL. The validity and reliability of the Persian version of this scale have been confirmed by Shabaninejad H et al., [26].
Statistical Analysis
Multivariate Analysis Of Variance (MANOVA) was used to investigate the effect of job and demographic variables (such as gender, marital status, working unit, number of patients per shift, overtime hours per month, second job, BMI, age, work experience, and monthly income) on the mean scores of WRQoL and workload. This test allowed examining the effect of one independent variable on more than one dependent variable.
Furthermore, to analyse the differences of the dependent variables between each of the independent variables (i.e., to examine the differences between each of the variables of the QWL and workload between each of the background variables), separate variance analyses were used as tests of between-subject’s effects. It is worth noting that the hypothesis of homogeneity of variance-covariance matrix was investigated using Box’s M method. To compare the effects of the estimated marginal means of the categorical variables (background variables) on each of the response variables (the mean scores of QWL and workload), the pair-wise comparison method was applied using the Bonferroni method. Moreover, after investigating the significance level of research variables on the two variables of the QWL and workload, in the next step, multiple regressions was applied to examine the factors affecting the QWL. In this study, alpha and beta were set up at 0.05 and 0.20 (a power of 0.80) respectively.
Results
The sample of the present study consisted of 61.4% women and 38.6% men. The mean age and BMI of the participants was 33.36±7.9 years, and 24.22±3.08 kg/m2 respectively. The mean QWL of subjects was obtained as 75.79±13.64 and the mean workload was calculated as 69.41±9.57 [Table/Fig-1].
Description of the background variables of the participants.
| Variable | Frequency | Percentage |
|---|
| Gender | Female | 516 | 61.4 |
| Male | 324 | 38.6 |
| Marital status | Single | 438 | 52.1 |
| Married | 402 | 47.9 |
| Hospital unit | Emergency | 216 | 25.7 |
| ICU | 384 | 45.7 |
| CCU | 240 | 28.6 |
| Extra working hours (overtime)* | <30 | 180 | 21.4 |
| 30-60 | 258 | 30.7 |
| 60-90 | 246 | 29.3 |
| >90 | 156 | 18.6 |
| Having a second job | Yes | 294 | 35 |
| No | 546 | 65 |
| Mean | SD |
| Number of patients per shift | 7.32 | 3.85 |
| Age (years) | 33.36 | 7.9 |
| BMI (kg/m2) | 24.22 | 3.08 |
| Work experience (years) | 10.53 | 7.33 |
| Monthly income (1000 Toman**) | 1522.86 | 446.41 |
| Quality of working life | 75.79 | 13.64 |
| Workload | 69.41 | 9.57 |
*Time worked in addition to one’s normal working hours
**The Iranian toman is a superunit of the official currency of Iran, the Rial
The initial assessment of the data showed that the QWL and workload scores did not include extreme outliers. A significant correlation was found between the variables of the QWL and workload using Bartlett’s test of sphericity (Chi-Square=123.35, p<0.001). Also, using the Box’s M test, the hypothesis of equality of covariance matrices of variables of the QWL and workload was examined among the different categories of background variables (Box’s M=648.96, p<0.001); therefore, the assumption of the homogeneity of the covariance matrices of the quantitative variables of this study (dependent) could not be approved in the different classes of the qualitative variables (independent). The results of the tests of between-subjects effects are presented in [Table/Fig-2]. This test examines the effects of each of the dependent variables individually in the groups of independent variables.
Estimated marginal means and tests of between-subjects effects.
| Source | Dependent variable | Group | Mean | SD | p-value |
|---|
| Gender | WRQoL* | Female | 75.28 | 0.34 | 108.0 |
| Male | 76.33 | 0.45 |
| AWWL** | Female | 69.76 | 0.44 | 0.163 |
| Male | 68.69 | 0.58 |
| Marital status | WRQoL | Single | 76.65 | 0.38 | 0.001 |
| Married | 74.96 | 0.36 |
| AWWL | Single | 66.96 | 0.49 | <0.001 |
| Married | 71.49 | 0.47 |
| Hospital unit | WRQoL | Emergency | 72.99 | 0.52 | <0.001 |
| ICU | 77.26 | 0.36 |
| CCU | 77.15 | 0.46 |
| AWWL | Emergency | 71.23 | 0.68 | <0.001 |
| ICU | 68.97 | 0.47 |
| CCU | 67.49 | 0.59 |
| Extra working hours* | WRQoL | <30 | 81.89 | 0.67 | <0.001 |
| 60-30 | 80.09 | 0.44 |
| 90-60 | 75.22 | 0.46 |
| >90 | 66.01 | 0.58 |
| AWWL | <30 | 66.19 | 0.76 | 0.001 |
| 30-60 | 69.08 | 0.59 |
| 60-90 | 69-96 | 0.87 |
| >90 | 71.68 | 0.57 |
| Having a second job | WRQoL | Yes | 73.79 | 0.44 | <0.001 |
| No | 74.82 | 0.31 |
| AWWL | Yes | 69.27 | 0.57 | 0.913 |
| No | 69.19 | 0.4 |
| Number of patients per shift | WRQoL | <0.001 |
| AWWL | 0.057 |
| BMI (kg/m2) | WRQoL | 0.437 |
| AWWL | 0.059 |
| Age (years) | WRQoL | <0.001 |
| AWWL | 0.001 |
| Work experience (years) | WRQoL | <0.001 |
| AWWL | 0.147 |
| Monthly income (1000 Toman) | WRQoL | <0.001 |
| AWWL | <0.001 |
*Work-Related Quality of Life
**Adaptive Weighted Workload
The results of the Pillai’s Trace test showed that the variable of gender had a weak but significant effect on the QWL and workload (pillai’s F(2,825)=3.15, p=0.043, Partial Eta2=0.01). The results of the Tests of between-subject’s effects also indicated that there was no significant difference between the estimated quality of life between the men and women; as the estimated workload was not significantly different among them (p>0.1).
The results of paired comparisons of the estimated marginal means using the Bonferroni method showed that there was no significant difference between the men and women in terms of the QWL and workload level. However, the QWL for the single individuals was higher than that for the married ones (p=0.001). Workload level was found to be higher in the married people than the single ones (p=0.001).
Based on the results of separate analysis of variance presented in [Table/Fig-2], it was found that there is a significant difference in the QWL among different departments of the hospital (p<0.001). There was also a significant difference among the different departments of hospitals in terms of the workload variable (p<0.001).
The findings of the study showed that the age of the employees had a significant multivariate effect on the response variables (Pillai’s F(2,825)=21.00, p<0.001, Partial Eta2=0.05). The results of the tests of inter-subject effects showed that this variable (age) had a significant effect on the QWL of employees (p<0.001), as its effect on the employees’ workload level was also significant (p=0.001).
The quality of working life for the emergency department staff was significantly lower than that of ICU (p=0.001) and CCU (p=0.001) staff, while the ICU and CCU staff’s QWL were approximately at the same level. Meanwhile, the workload level of the emergency department staff was significantly higher than that for the ICU staff (p=0.019); such a difference was also observed between the emergency department staff and CCU staff (p=0.001). However, no significant difference was found between the employees working in the ICUs and CCUs in terms of the workload level.
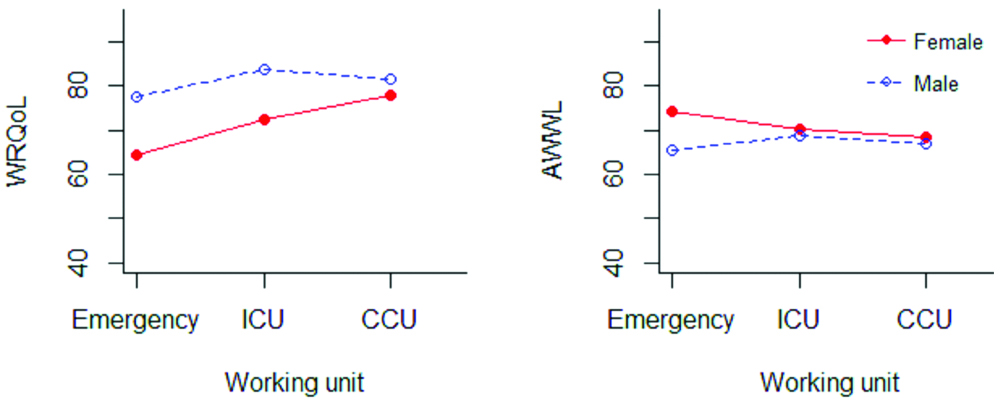
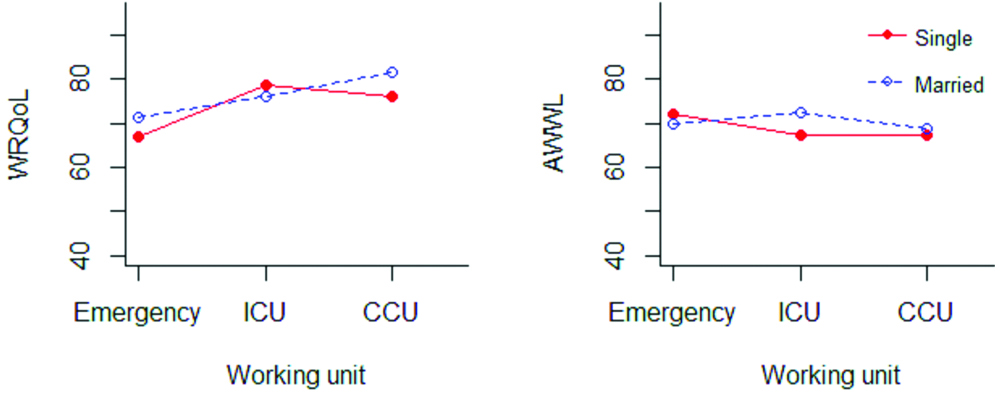
Comparison of the WRQoL and the workload mean scores of the employees in the various studied departments of the hospital in terms of gender and marital status is represented in [Table/Fig-3,4]. As it is evident, the lowest WRQoL score is associated with the female and single nurses in the emergency departments.
Work-related quality of life and workload of male and female nurses in different units of the hospitals.
Work-related quality of life and workload of single and married nurses in different units of the hospitals.
In order to investigate the effect of the background variables and workload on the QWL of employees, the multivariate regression analysis was applied using the Forward method. The results of the regression analysis indicated that the variables of the overtime hours, number of patients per shift, age, and the workload level would ultimately remain in the model (F5.134=79.67, p<0.001), as they can account for 73.9% of the changes (Adjusted R2=0.739).
Based on the results of regression analysis [Table/Fig-5], the effects of the variables of overtime hours, the number of patients per shift, and age on the QWL of employees were obtained as 43% (Beta=-0.43, p-value=<0.001), 23% (Beta=-0.23, p-value=<0.001), and 19% (Beta=-0.19, p-value=<0.001), respectively. The workload level (Beta=-0.15, p-value=0.001) had adverse effect on the employees’ quality of working life.
The effect of background and workload parameters on the work-related quality of life.
| Independent variable | Model coefficients |
|---|
| Regression coefficient (B) | Standard error | Standardised coefficient of regression (β) | t-value | p-value |
|---|
| Working overtime | -5.79 | 0.71 | -0.43 | -8.17* | <0.001 |
| Number of patients per shift | -0.81 | 0.21 | -0.23 | -3.84* | <0.001 |
| Age | -0.33 | 0.09 | -0.19 | -3.63* | <0.001 |
| Workload | -0.22 | 0.07 | -0.15 | -3.25* | 0.001 |
*Significant at the 5% level
In order to further investigate the effect of workload on the QWL of employees, the regression of sub-scales of workload was used to evaluate its effect on the quality of employees’ working life, using the Forward method. The results of this analysis showed that the physical and mental workload variables could ultimately remain in the model (F3,136=9.05, p<0.001), as they can explain 14.8% of the changes (Adjusted R2=0.148) [Table/Fig-6].
The effect of workload elements on the work-related quality of life of employees.
| Independent variable | Model Coefficients |
|---|
| Regression coefficient (B) | Standard error | Standardised coefficient of regression (β) | t-value | p-value |
|---|
| Mental demand | -0.13 | 0.06 | -0.19 | -2.19* | 0.03 |
| Physical demand | -0.16 | 0.06 | -0.21 | -2.59* | 0.011 |
*Significant at the 5% level
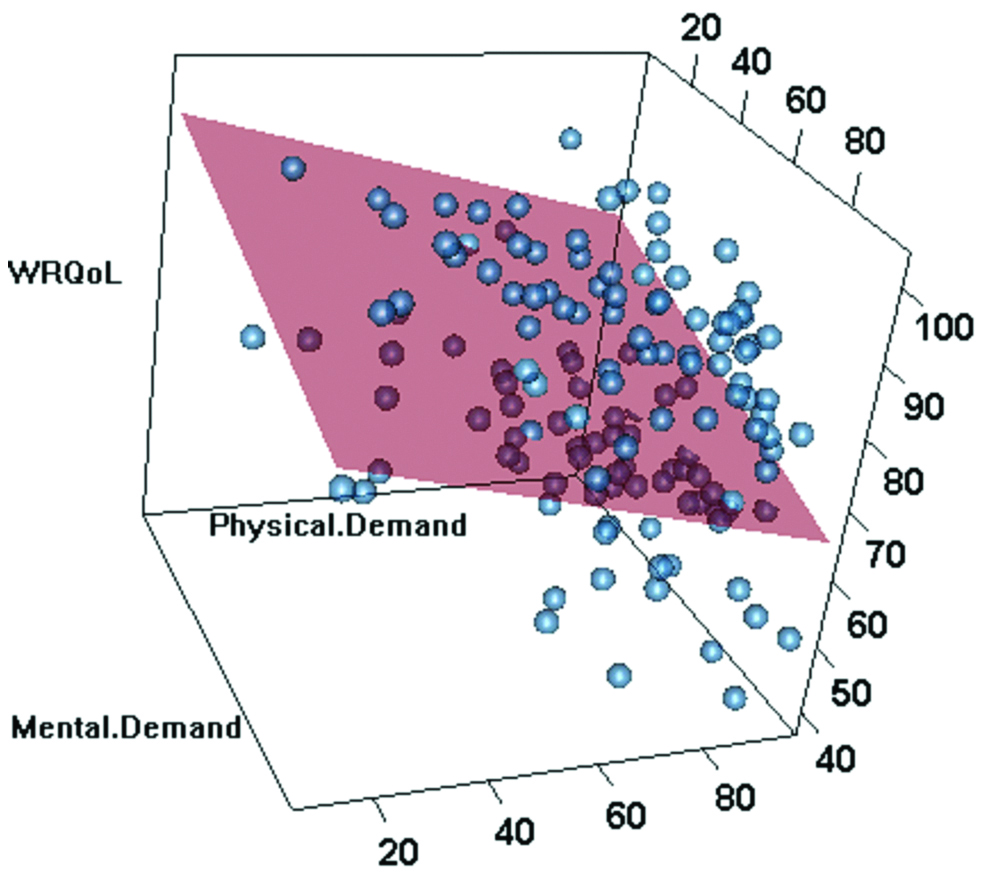
The results of regression analysis showed that the effect of physical component of the workload on the employees’ QWL was -21% (Beta=-0.16, p-value=0.011), and the effect of mental was -19% (Beta=-0.13, p-value=0.03). In other words, both affecting components of the workload variable (physical and mental) had adverse effect on the QWL of employees. This is implicitly shown in [Table/Fig-7].
The relationship between the quality of working life and physical and mental subscales of workload.
Discussion
The present study investigated the effects of background variables and workload parameters on the nurses’ QWL. The findings indicated that in general, the WRQoL was in the lower level among the female nurses, married ones, nurses working in the emergency departments, those with an overtime of over 90 hours, and those who had a second job compared to the effects of other studied variables; that is to say that the difference in mean score of WRQoL was statistically significant in all groups in terms of the studied background variables except gender and BMI. The relationship between the variables of age, work experience, and the number of patients per shift and nurses’ quality of life scores was statistically significant. Also, based on the results of multivariate regression analysis, the variables of overtime hours, the number of patients per shift, age, and the level of workload remained in the regression model and their coefficients of influence were estimated -43%, -23%, -19%, and -15%, respectively.
Although the role of gender on the nurses’ WRQoL score was not statistically significant, the QoL score of female nurses was lower than that of men. Other studies investigated gender differences in the QWL also suggested that men are in more privileged positions in work environments, while women’s commitment to their work is higher [27,28]. Gender differences have been proven in many of the indicators of work quality including the independence, job satisfaction, supervisor support, job security, and balance between work and life. According to previous studies, men are more likely to be paid better than women, get better organisational posts, and have more chance of flexible using of their work time and making decision on their work plan; while women spend more time on working and are more loyal to the organisation than men [27,28]. Female workload score was also higher than of men, although this difference was not statistically significant. Although both female and male nurses experienced a high level of workload, all data showed a more favourable situation for men compared to women. Women are more stressed due to unpaid home-task and have more responsibilities to their family. Studies have shown that women in the workplace have a higher level of norepinephrine than men, reflecting their high volume of workload [29,30].
The results of Pillai’s trace test showed that married nurses had significantly lower QoL than unmarried ones, which could be affected by their higher level of workload resulting in a lower level of job satisfaction. This can be due to many reasons including the current situation of economic pressures in Iran, life responsibilities, and family problems for married people [31], although identifying the root causes of this issue requires more comprehensive studies. Han KT et al., examined the relationship between the QoL and marital status among the cancer patients and supervisors [32]. They observed that the QoL score was higher in single people. However, there are some studies that consider the QoL of married people higher than that of in single people [33,34], this may be due to the more emotional and social support that married people receive from their spouses.
Emergency departments of hospitals are among the most stressful working environments. This can be justified with the difficult work conditions in EDs, including the large number of patients, the need for rapid decision-making, the high volume of workload and psychological pressures, lack of resources (human and materials), and poor support. As a result, the prevalence of burnout among the nurses and doctors working in this department is usually at the moderate to high level [35,36]. Similar to the results of this study, other studies have also shown that the ED staff have lower level of QoL and more workload level [35,37].
Based on the results of some previous studies, long working hours can be associated with the higher workloads, poorer lifestyles, higher levels of stress, higher fatigue, and lower level of QoL [38,39]. Long working hours have a particularly negative effect on the interaction between work and home of employees [40]. Similarly, in the present study, with the increase in the overtime hours, the level of WRQoL decreased and the level of workload increased in nurses. Long working hours has significant effects on lifestyle, including the pattern of sleep, the discipline of everyday life, and meals; and it has been shown that people with longer working hours experience more stress [40]. Consistent with this finding, the results of tests of between-subjects effects showed that nurses without a second job have a higher level of QoL than nurses with a second job.
The results of tests of between-subjects effects showed that the variables of age and work experience of employees have a significant effect on the QWL of employees, so that by an increase in the age and work experience, the WRQoL decreases. These two variables (age and work experience) had a reverse effect on all components of the WRQoL variable. Many studies have shown that mental and physical abilities and capacities of nurses reduce with the increase in their age [41,42]; as a result, this variable, with the effect on job satisfaction, increased work stress, reduced control on work, increased exhausting effort, and frustration, can reduce the WRQoL in this high-stressed job [43].
The QWL and work-related consequences, such as job satisfaction and organisational commitment are among the important issues in the development of human and organisational resources [44].
Limitation
Despite its large sample size, this study had some limitations, including the cross-sectional nature of the study, the complexity of the considered topic, the presence of many influential factors on the level of WRQoL (such as the personal life, hospital laws and policies with regard to the compensation and benefits, interaction with colleagues and supervisors, work environment and working conditions, and the possibility of job growth), and using a questionnaire as a subjective measurement tool (Differences in understanding and interpretation, dishonesty of respondents).
Conclusion
The results indicated the simultaneous effect of the studied variables on the nurses’ WRQoL; among these, the variables of overtime hours, the number of patients per shift, age and workload level was found to affect the work-related quality of life.
Funding: This article is extracted from research project No.96023. The authors would like to acknowledge the financial support of Kermanshah University of Medical Sciences for this research.
*Time worked in addition to one’s normal working hours
**The Iranian toman is a superunit of the official currency of Iran, the Rial
*Work-Related Quality of Life
**Adaptive Weighted Workload
*Significant at the 5% level
*Significant at the 5% level