Serum carbohydrate antigen (CA 19-9) also called sialylated Lewis (a) antigen is a tumour marker elevated in many types of benign and malignant gastrointestinal and hepatobillary cancer including ductal epithelial cancers. In tissues, CA 19-9 exists as an epitope on sialolacto-N fucopentose II ganglioside (glycolipid) and in serum, CA 19-9 antigen is associated with a mucin [1]. This glycolipid is synthesised by the pancreatic and biliary ductal cells and also by epithelium of gastric, colonic, endometrial, and salivary epithelium [2]. It has a high sensitivity and specificity in diagnosing various malignant conditions. In pancreatic cancer it is reported to have a sensitivity of 70-90% and specificity of 68-91%, whereas in cholangio carcinoma sensitivity and specificity is 67.5% and 86.8%, and in Gall Bladder cancer it is around 66% and 90%, respectively. Moreover, sensitivity and specificity is also high in diagnosing Periampullary carcinoma [3-6]. CA19-9 is also elevated in various benign conditions of the hepatobiliary tract which includes Mirizzi syndrome, autoimmune pancreatitis, benign biliary strictures secondary to primary sclerosing cholangitis, and pancreatic exocrine dysfunction in diabetic patients etc [7-9]. This often leads to diagnostic difficulties.
Obstructive jaundice is the most common condition that is associated with significant elevation in serum CA19-9 but it may not be able to differentiate benign and malignant pancreatobiliary cases of Obstructive jaundice. Several studies points to the fact that only by adjusting the serum bilirubin level, the cut-off value of CA19-9 have to be established to distinguish benign and malignant disease [10-14]. To improve diagnosis to achieve a better sensitivity and specificity, authors have suggested to adjust CA19-9 value by dividing it empirically by the serum bilirubin value [11,12] or by inflammatory marker as inflammation contributes to elevating the CA19-9 value. Inflammation can be assessed by monitoring the acute-phase proteins like CRP which rises in response to infection, trauma and malignancy [15].
Hence, our study targeted to investigate the diagnostic utility of Serum Carbohydrate Antigen (CA19-9), CRP, Serum Bilirubin level and their ratios CA19-9/total bilirubin ratio and CA19-9/CRP ratio for a better sensitivity and specificity in differentiating malignant obstructive jaundice from benign obstructive jaundice.
Materials and Methods
A prospective case control study was carried out in the Department of Surgery and the Department of Biochemistry of ESIC Medical College, Joka Kolkata from January to August 2017, on 75 diagnosed cases of obstructive jaundice; taken from admitted patients of Surgery department irrespective of age and sex. They were further divided into two groups, Test Group-I (n=36) which included patients of malignant obstructive jaundice and Test Group-II (n=39) which contained patients of benign obstructive jaundice. The study protocol was approved by Research and Ethical committee, ESIC Medical College, Joka Kolkata vide No 412 (Dean-Joka)/IEC/14-15/Vol 1-14479. Verbal informed consents were obtained from all subjects prior to the start of the study. All included patients were subjected to detailed history taking and laboratory examination.
Taking all aseptic and antiseptic precautions, 5 mL of venous blood was drawn in two clotted vacutainers from the anti cubital veins of the patients; one was used for estimation of CA 19-9 and another for estimation of CRP and total bilirubin. Serum was separated using centrifuge.
Serum CA 19-9 was assessed by chemiluminescent immunometric technique on Ascess 2 immunoassay system (Beckman Coulter Diagnostics, Ltd.,). It utilises the binding of CA 19-9 principles to a specific monoclonal antibodies in an automated two site sandwich enzyme immunoassay and utilises alkaline phosphatase enzyme conjugated to monoclonal antibody, it utilises dioxetane-based chemiluminescent substrate and measures light production from a chemiluminescent reaction with measuring range (0.80-1665 U/mL) and standard cut-off value 37 U/mL as determined by the manufacturer Beckman Coulter Diagnostic.
Serum CRP was assessed at the time of admission by particle-enhanced turbidimetric immunoassay method using latex particles coated with monoclonal anti-CRP antibodies based on principles of agglutination reaction which is measured in 630 nm wavelength using Coral diagnostic kits. The increase in turbidity corresponds to the concentration of CRP in the test specimen and reading of the precipitate done with Beckman Coulter AU 480 FR Chemistry analyser (Beckman Coulter Diagnostics, Ltd.,). The reference range for CRP assay was 0.6 mg/dL.
Serum total bilirubin estimation was done via colorimetric principle using Mod Jendrassik and Grof’s method using Coral Clinical System Kit. Bilirubin reacts with diazotised sulphanilic acid to form a coloured azobilirubin compound; the intensity of colour formed is directly proportional to the amount of bilirubin present in the sample which is measured in 546 nm wavelength in a Beckman Coulter Chemistry Analyser AU480FR. The normal reference value for total bilirubin is upto 1 mg/dL.
CA 19-9/CRP ratio and CA19-9/total bilirubin ratio were calculated.
Since the Statistical data were not normal, descriptive statistics was presented using median and Interquartile Range (IQR). Different groups of study were analysed by applying Non-Parametric Mann-Whitney U test or Wilcoxon rank-sum test. ROC analysis was done to find the predictive value of the biochemical markers. To find out the association and the impact of the markers on disease malignancy, Pearson’s correlation coefficient along with regression analysis was performed. After the biochemical estimations, the results obtained were statistically analysed using statistical software, R version 3.4.0.
Results
The present study covers 75 cases of obstructive jaundice. Majority (80%) of the study population were females. The average age of the study population was 53 years. Males were comparatively (47 years) younger than females (54 years).
Multivariable Fractional Polynomial (MFP) method was used to identify the independent variable having a significant impact in model building [Table/Fig-1]. Accordingly, the variables were incorporated in the study design. Kolmogonor Smirnov test was performed (results not shown) to access the normality assumption for the biochemical parameters. However, the test results suggested that the biochemical parameters were not normal and hence, non-parametric test Mann-Whitney U test or Wilcoxon rank-sum test was performed as shown in [Table/Fig-2] for comparison of biochemical parameters in both groups. All the three parameters were found to be statistically significant.
Multivariable Fractional Polynomial (MFP) method to identify proximate determinants to be included in the model.
| Initial | Final |
|---|
| Variables | Degree of freedom | Select | Alpha | Status |
|---|
| CA19-9 | 4 | 0.2000 | 0.100 | -1.5 |
| Total Bilirubin | 4 | 0.2000 | 0.100 | -2.2 |
| CRP | 4 | 0.2000 | 0.100 | -2 |
Comparison of biochemical parameters in malignant obstructive jaundice group and benign obstructive jaundice group.
| GROUPS | p-value |
|---|
| Benign | Malignant |
|---|
| Median | IQR | Median | IQR |
|---|
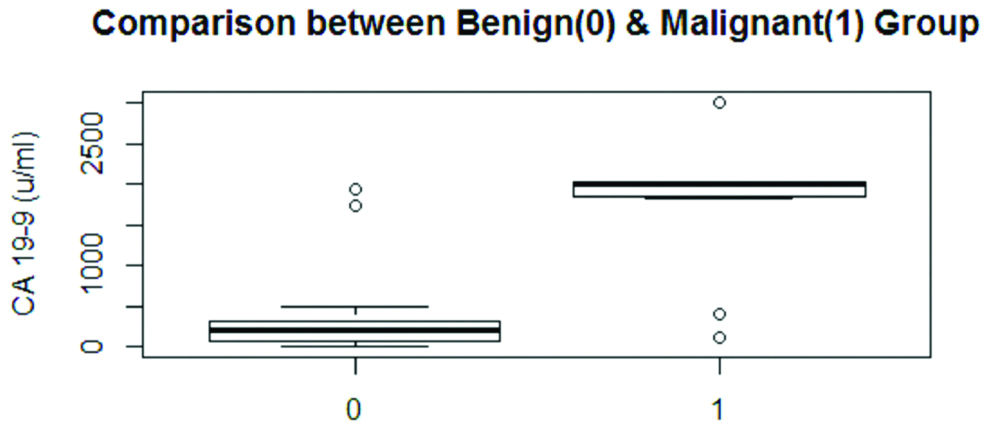
| CA 19-9 | 206 | 237 | 2016 | 162 | 0.000 |
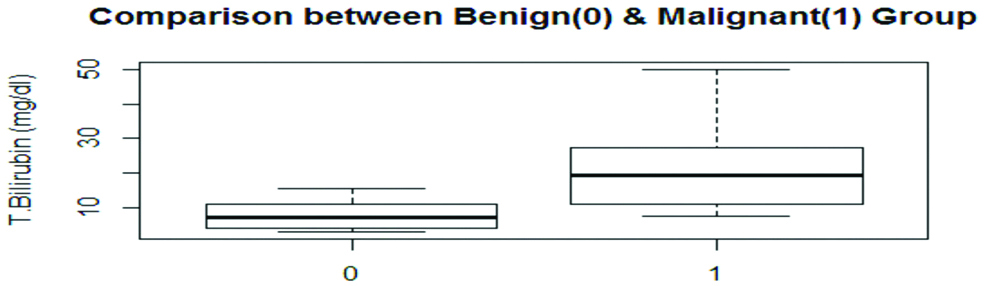
| Bilirubin | 7.4 | 6.9 | 19.4 | 16.10 | 0.000 |
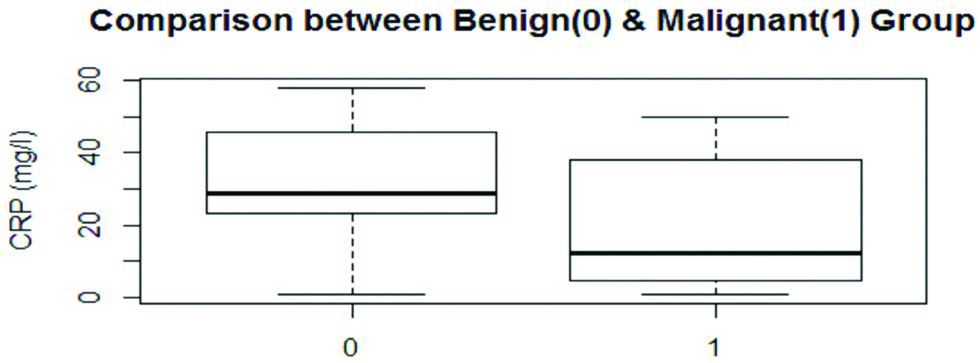
| CRP | 12.35 | 23.30 | 28.7 | 22.7 | 0.0316 |
In [Table/Fig-3a], box-whisker plot for CA19-9 suggested presence of out layers but no influential variable were found for CRP as per [Table/Fig-3b] and total bilirubin as per [Table/Fig-3c], clearly depicting the data of CA19-9 to be skewed. [Table/Fig-4] shows a comparison of the biochemical parameters within the different malignant subgroups. Among the subgroups median values of CA19-9 was highest for carcinoma head of pancreas (2508). CRP came to be highest for periampullary carcinoma (45.8) and for total bilirubin, carcinoma gall bladder was the highest (22.9) as per comparison of median values using non-parametric Kruskalwali test.
Box-Whisker plot of CA19-9 comparison between Benign and Malignant Obstructive Jaundice Groups.
Box-Whisker plot of CRP comparison between Benign and Malignant Obstructive Jaundice Groups.
Box-Wisker plot of Total Bilirubin level comparision between Benign and Malignant Obstructive Jaundice Groups.
Comparison between serum total bilirubin, CRP and CA19-9 median levels in different subgroups of the malignant group at time of admission.
| Malignant Groups | Range | Median | p-value |
|---|
| CA 19-9 u/mL | Colangiocarcinoma | 220.8 | 202.6 | 0.0003 |
| Ca Head Pancreases | 1016 | 2508 |
| Periampullary Ca | 1741 | 3.4 |
| Ca Gall Bladdeer | 1915 | 1890 |
| CRP (mg/dL) | Colangiocarcinoma | 30 | 43 | 0.0460 |
| Ca Head Pancreases | 44.3 | 22.9 |
| Periampullary Ca | 52.3 | 45.8 |
| Ca Gall Bladdeer | 37 | 17.9 |
| Total Bilirubin (mg/dL) | Colangiocarcinoma | 10.7 | 8.5 | 0.0245 |
| Ca Head Pancreases | 14.9 | 19.7 |
| Periampullary Ca | 8.2 | 11.1 |
| Ca Gall Bladdeer | 16.5 | 22.9 |
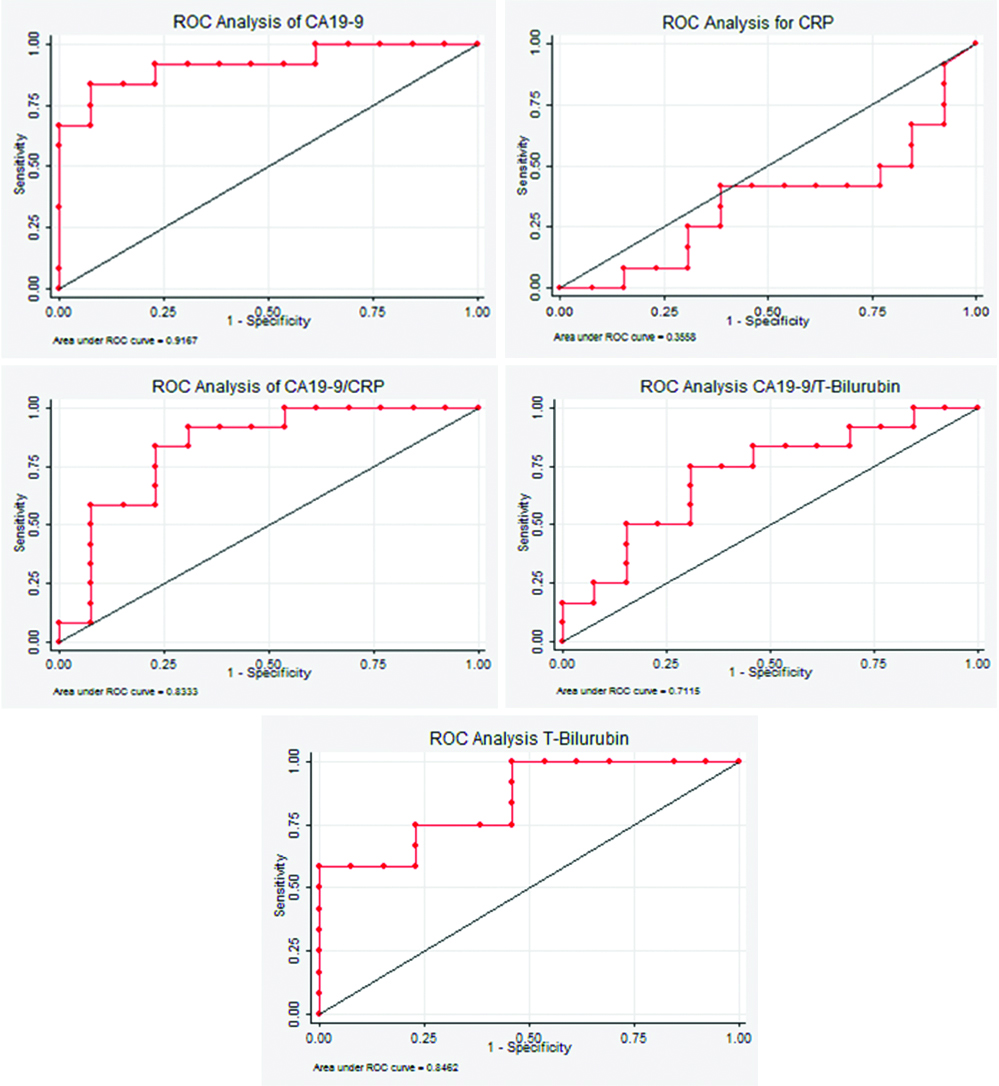
Sensitivity, specificity, positive predictive value and negative predictive value of the biochemical parameters and their ratio are given in [Table/Fig-5]. The diagnostic power of the biochemical parameter was accessed using various screening tools [Table/Fig-5]. CA19-9 alone has the highest sensitivity value of 91.67 at a cut-off point of 410 U/mL, whereas CRP reported the lowest in both sensitivity and specificity. Similar findings were reported in ROC analysis and Area under ROC curve (AUC) of the biochemical parameters and their ratio as per [Table/Fig-6]. [Table/Fig-7] gives a Logistic Regression Analysis with biochemical parameters as independent variable and malignancy as dependent variable. Total bilirubin was found to be the most significant independent factor having an impact on malignancy.
Sensitivity, specificity, Positive Predictive Value (PPV), And Negative Predictive Value (NPV) for different CA19-9 cut-off values.
| Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|
| CA19-9 cut-off 410 (U/ mL) | 91.67 | 76.92 | 79.5 | 96.7 | 86.6 |
| CRP cut-off 33.5 (mg/dL) | 41.6 | 61.5 | 50.0 | 53.0 | 52 |
| Total Bilirubin cut-off 11.4 (mg/dL) | 75 | 76.92 | 75 | 76.9 | 76 |
| CA19-9/CRP cut-off 40.56 | 83.33 | 76.92 | 76.9 | 83.3 | 80 |
| CA19-9/Bilirubin cut-off 73.80 | 75 | 69 | 0.69 | 0.75 | 72 |
ROC analysis of CA19.9, CRP, CA19.9/CRP, CA19.9/Total Bilirubin and Total Bilirubin respectively also showing Area under ROC curve (AUC).
Logistic regression analysis of CA19-9, CRP, Total Bilirubin, CA19-9/CRP and CA19-9/Total Bilirubin.
| Independent Biochemical Parameters | Coefficient | Std Error | 95% Confidence Interval | p-value |
|---|
| CA19-9 | 0.01 | 0.002942 | (-0.00, 0.01) | 0.06 |
| Total Bilirubin | 0.66 | 0.2917806 | (0.91, 1.23) | 0.02 |
| CRP | -0.03 | 0.0322164 | (-0.095,0.31) | 0.32 |
| Pseudo R2=0.8034 |
Discussion
CA19-9 is a non-specific marker of malignant condition of HBT as it is elevated in various benign conditions [7-9]. However, the present study found CA19-9 as a significant predictor and a useful tool for detection of malignant jaundice as is observed in study by La Greca G et al., and Devbrata R et al., [15,16]. Sayed MM et al., in their study have observed when CA19-9 cut-off value was pushed up from 37 (U/mL) to 100 (U/mL) the sensitivity decreased (64%) while the specificity increased (64%) [17]. Similarly, in another independent study, La Greca G et al., [15] observed when CA19-9 cut-off value was pushed up from 32 (U/mL) to 100 (U/mL) the sensitivity decreased from 82.3 to 68.6 while the specificity increased from 45 to 64.7. The present study also has similar findings, increasing CA19-9 cut-off decreases sensitivity however specificity improves. The present study as per ROC analysis finds 410.7 as an optimum cut-off point at which one can observe maximum sensitivity (91.67%) and specificity (84%).
Inflammation can have a significant impact over CA19-9 and have a role in malignant obstructive jaundice [15]. Study by Padillo FJ et al., suggested that due to increase in endotoxin level in biliary tract obstruction, acute phase proteins like CRP is significantly elevated in malignant and benign obstructive jaundice [18]. Morley JJ et al., suggested that inflammation due to invasion of tumour in malignancy may be a cause of rise in CRP [19]. Again, Szkandera J et al., in his study has correlated CRP with poor clinical outcome in patients with Pancreatic cancer and recommends CRP as a marker of hepatobiliary tract. However, the diagnostic role of CRP as a test for the detection of pancreato-biliary malignancy remains poorly defined and controversial, because the utility of CRP has several limitations as it is non-specific inflammatory marker, many benign conditions of the hepatobiliary tract has an acclerated elevation of CRP [20]. This study finds CRP to be significantly elevated in malignant obstructive jaundice compared to benign obstructive jaundice with levels highest for Periampullary carcinoma followed by carcinoma head of pancreas but it also shows CRP to be a poor screening tool in detection of pancreatobiliary malignancy as seen in ROC analysis, however, when a ratio of CRP i.e., (CA19-9/CRP) is taken, it turns out to be a better indicator for pancreatobiliary malignancy as seen from the area under ROC curve (AUC=0.83) and can be used as a screening tool. This result is in conformity with the findings of a study from La Greca G et al., and Sayed MM et al., [15,17]. La Greca G et al., in their study evaluated CA19-9 values by adjusting CRP and total bilirubin to predict malignancy in obstructive jaundice [15]. In this study, we have considered the ratio of CA19-9 with CRP and total bilirubin to increase the reliability, specificity and sensitivity in detection of pancreatobiliary malignancy. We have also statistically considered Multivariable Fractional Polynomial (MFP) method and have found this independent variable to have a significant impact in model building.
In the current study, the serum total bilirubin level was significantly higher in malignant obstructive jaundice compared to benign obstructive jaundice group with highest for Carcinoma Gall Bladder among the malignant group. This agrees with the study done by Garcea G et al., and Liu W et al., [21,22]. Liu W et al., in their study found Total Bilirubin to have minimal differential diagnostic power (AUC=0.590) whereas CA19-9 and the ratio with bilirubin having stronger differential diagnostic power (AUC=0.815 and AUC=0.889, respectively) [22]. This study also has similar findings in respect of CA 19-9 (AUC=0.91) but has contrasting results in terms of Total Bilirubin (AUC=0.84) and CA19-9/total bilirubin ratio (AUC=0.71). Total Bilirubin at a cut-off value of 11.4 mg/dL shows a sensitivity and specificity of 75 and 76 respectively whereas the specificity for the ratio is even lower (69). Thus, the present study does not support such findings. Using ROC analysis and Logistic Regression Analysis the present study finds Total Bilirubin, alone as a single most significant independent factor having an impact on malignancy.
Limitation
Small sample size and the study being conducted in only one centre may be considered as the limitation of this study.
Conclusion
The present study proposes that CA19-9 at a cut-off value of 410 has a better sensitivity and specificity compared to CA19-9/CRP ratio and CA19-9/total bilirubin ratio. Also, one of the major finding of the study is when CRP adjusted for CA19-9 i.e., CA19-9/CRP ratio proves to be a better marker that can be used along with CA 19-9 in differentiating between the malignant and benign obstructive jaundice.