Non-communicable diseases like hypertension, diabetes, hyperlipidemia are most common disease increasing the co-morbidity. Non-communicable diseases need early detection and management. Lung diseases are some of the medical conditions that affect the world population. Some of the common lung diseases include asthma, chronic obstructive pulmonary disease, bronchitis, bronchiectasis, etc., Cardiovascular disease are at top notch being one of the cause of individual mortality with combination of foresaid co-morbid conditions. Cross-sectional imaging has been increasingly used in recent years for cardiac and chest evaluation as multiplanar imaging gives excellent image characterization. Suppressing the signal from flowing blood while enhancing the tissue fluid signal in T2STIR imaging sequence made its usefulness in cardiac MRI [1].
Study demonstrate the relevance of the isotropic 3D T2 Turbo-Spin-Echo (TSE) sequence with Short-Term Inversion Recovery (STIR) and variable flip angle RF excitations (SPACE: Sampling Perfection with Application optimised Contrasts using different flip angle Evolutions) for high-resolution brachial plexus imaging. Study on 3D STIR SPACE in brachial plexus imaging demonstrated that this sequence not only replaces 2D STIR sequence but also better in delineating the nerve anatomy and pathology [2]. Studies preferred to obtain heavily T2W 3D-SPACE images for the indications mentioned by Hingwala D et al., [3]. Entire brain or spinal cord MRI scanning can be done with single acquisition of T2 STIR SPACE Sequence without significant artifacts and in lesser time as compared to other heavily T2 Weighted sequences [4]. In dyspneic patients like, suspected pulmonary embolism in antenatal mothers, renal failure patients and suspected congenital heart diseases, though contrast GRE is used [5], fast MRI sequence like T2-Weighted Short Inversion Time Inversion Recovery (3D-T2-STIR) gated sequence can be used. With this view this study was done with an aim to evaluate the value of 3-Dimensional T2-Weighted Short Inversion Time Inversion Recovery (3D-T2-STIR) gated sequence in cardiac and chest MR imaging.
Materials and Methods
A cross-sectional study was conducted from October 2015 to January 2017 in which 41 patients with chest and cardiac diseases including pregnant and renal failure patients were studied. The study protocol was approved by the local human experiments and ethics committee. Informed written consent was acquired from every subject after explaining the details of this study. Sample size calculation was done based on the assumption that the extent of agreement will be strong (kappa value 0.7) between the reviewers for the evaluation of diagnostic image quality of 3D-T2-SPACE STIR sequence in comparison with routine MRI sequences. For 80% power and 5% alpha error, the minimum required sample size was 36. Assuming 10% of patients will refuse to participate in the study, the sample size was increased to 41. Patients came for cardiac and chest MR imaging was performed on 3-T MR system (SKYRA-SQ Engine; Siemens,) using 18 channel phased array body coil and the neck coil. In our institute, the MR imaging protocol commenced with a localizer using Trufi (steady-state free precession) sequence. HASTE Axial and Coronal sections of 10 mm thickness were acquired from aortic arch level to inferior vena cava and hepatic veins level below diaphragm. Functional imaging was done by acquiring Cine trufi, Cine Flash (GRE) and Cine phase-contrast sequences. The routine MRI sequences includes coronal and axial scans using haste (Half Fourier Acquisition Single shot TurbospinEcho imaging), multi-slice 2D true fast imaging with steady-state precession (TrueFISP or TRUFI) and Cine Trufi (steady-state free precession). Our sequence of interest includes T2-weighted SPACE STIR respiratory-gated imaging. Both routine and SPACE STIR sequences were compared.
The acquisition time for 3D-T2-STIR Sequence was usually 5 minute 12 seconds and the parameters are as follows: TR=2200 ms TE=101 ms, flip angle=150 degrees, TI=220 ms, Echo Train Length:101, Slice thickness: 4 mm, Slices oversampling=80%, slice per slab=56, Field Of View (FOV)=380×380 mm, matrix size=256×256, number of acquisitions=1.4, bandwidth=651 Hz/pixel. The acquisition time for every scan was usually 5 minute 12 seconds. A sensor for respiratory-triggered acquisition is also positioned at the start of each examination. The images were obtained in addition to routine cardiac or chest MRI sequences. Multiplanar reformation from 3D-T2-STIR SPACE data sets was done via Siemens workstation. Two separate observers with expertise in cardiovascular and chest imaging scored the image qualities of 3D-T2-SPACE STIR sequences for diagnosis in a blinded fashion using a three point scale scoring system visually as good, fair and poor. The image qualities of 3D-T2-SPACE STIR sequences are compared with routine MRI sequences such as Haste, 2D Trufi and cine Trufi sequences, the diagnostic abilities for both runs were scored by the experienced radiologists as good, fair and poor [6]. Good quality images define good anatomical delineation with adequate signal intensity which aids in definite diagnosis. Fair quality images define images with no artefacts but moderate signal intensity which is inadequate for definite diagnosis. Poor quality images define images with artefacts and poor signal intensity such that diagnosis could not made [7]. Presence of artifacts, scan time consumption of 3D-T2-SPACE STIR sequences and routine MRI sequences were also done.
Statistical Analysis
The extent of agreement between the reviewers for the evaluation of diagnostic image quality of 3D-T2-SPACE STIR sequence in comparison with routine MRI sequences was calculated with Kappa statistics. Kappa values those between 0 and 0.40, poor agreement; those between 0.41 and 0.75, good agreement; and those between 0.76 and 1.00, excellent agreement [8]. Descriptive statistics calculated for background variables. Data analysis was done using SPSS 15.0 version.
Results
A total of 41 patients with chest and cardiac diseases with age ranging from 13 to 77 years (mean-34.2 years and SD=14.8 years) were included in the study. In this study, 17 female patients and 24 male patients were included. Among them, 15 patients had chest findings, 26 had CVS and with unremarkable findings.
The image qualities of 3D-T2-SPACE STIR sequences as observed by two radiologists in blinded fashion is given in [Table/Fig-1] as frequency percentages. Both the radiologists gave the opinion that only one image was of poor quality. As per one radiologist, 73.2% of the image sequences were of good quality and as per second radiologist 65.9% of the sequences were of good quality.
The image qualities of 3D-T2-SPACE STIR sequences as observed by two radiologists.
| Quality | Radiologist 1 | Radiologist 2 |
|---|
| Fair | 10 (24.4%) | 13 (31.7%) |
| Good | 30 (73.2%) | 27 (65.9%) |
| Poor | 1 (2.4%) | 1 (2.4%) |
The level of agreement between the two radiologists in their observation on the image qualities of 3D-T2-SPACE STIR sequences were given as kappa statistics. Kappa value is 0.723 which shows that there is excellent agreement between two radiologists.
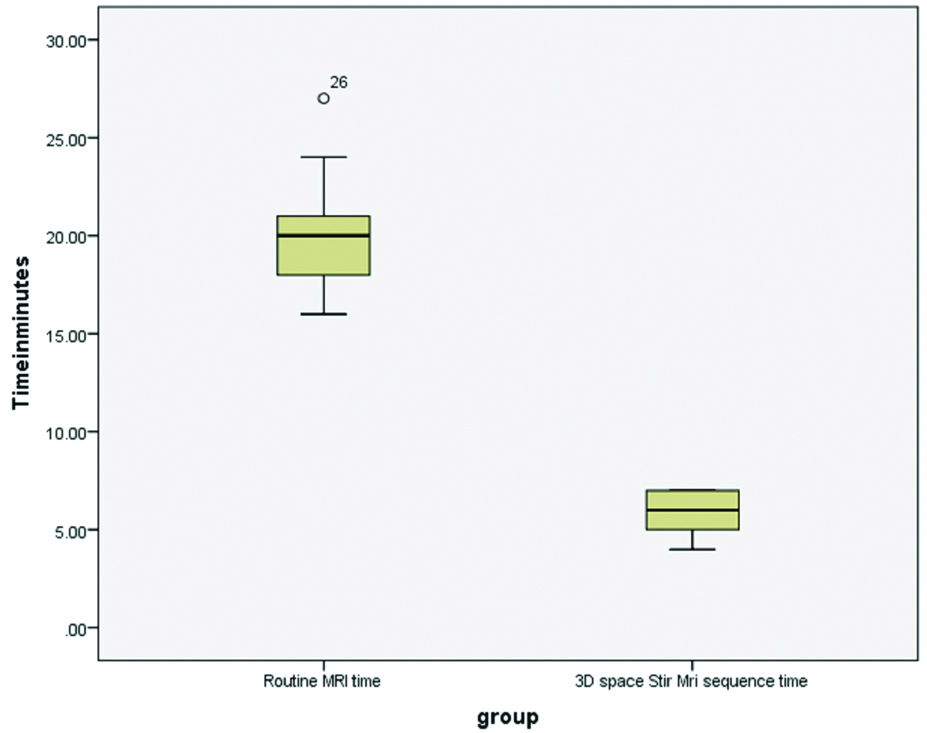
The mean duration of time taken for routine MRI scan was 20.2 minutes (SD=2.4 minutes) and time taken for 3D Space Stir MRI Sequence was 5.8 minutes (SD=1.03 min). This difference was tested by unpaired t-test and found to be statistically highly significant (p=0.000) [Table/Fig-2].
Time taken for routine MRI and 3D Space Stir MRI Sequence.
Discussion
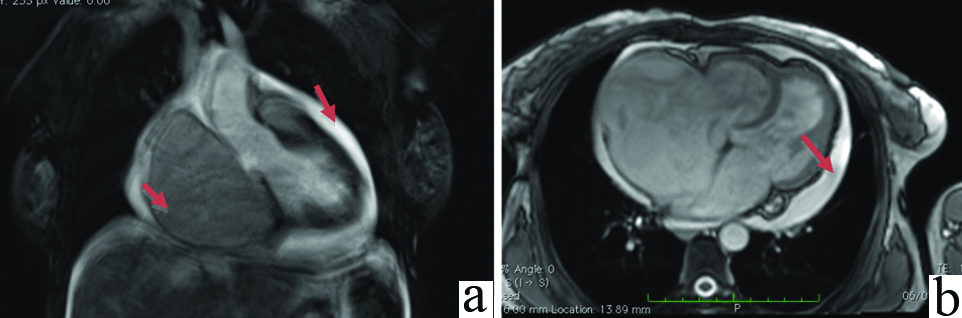
In this study, 3D T2 SPACE STIR sequences demonstrated good image quality which is statistically significant as shown by the excellent level of agreement between the two radiologists by Kappa value of 0.723. Both the anatomical structures and pathologies are visualized in this sequence as shown in the [Table/Fig-3,4,5,6,7,8,9,10,11,12 and 13]. In [Table/Fig-3], T2 SPACE STIR MR images of good quality demonstrating hypo intense thrombus in right and left distal pulmonary arteries extending into the segmental arteries of antenatal female with breathlessness. Aneurysmal dilatation of right atrium and pericardial effusion is demonstrated in T2 SPACE STIR MR image with good image quality similar to routine TRUFI sequences in [Table/Fig-4].
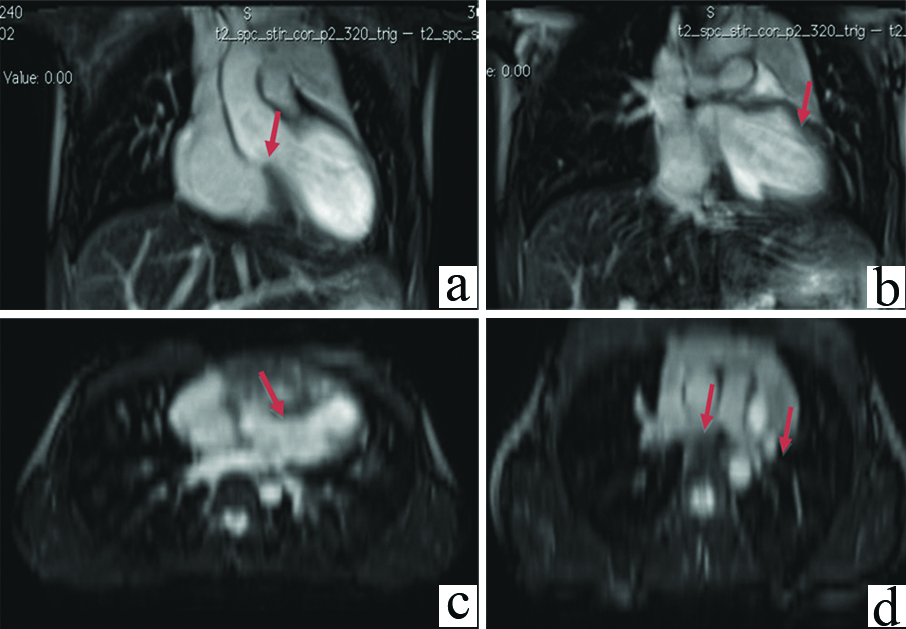
Pulmonary thromboembolism. A 28-year-old female antenatal patient who has dyspnea, chest pain: (a) Axial and (b) coronal T2 SPACE STIR MR images shows hypointense thrombus (red arrows) in right and left distal pulmonary arteries extending into the segmental arteries.
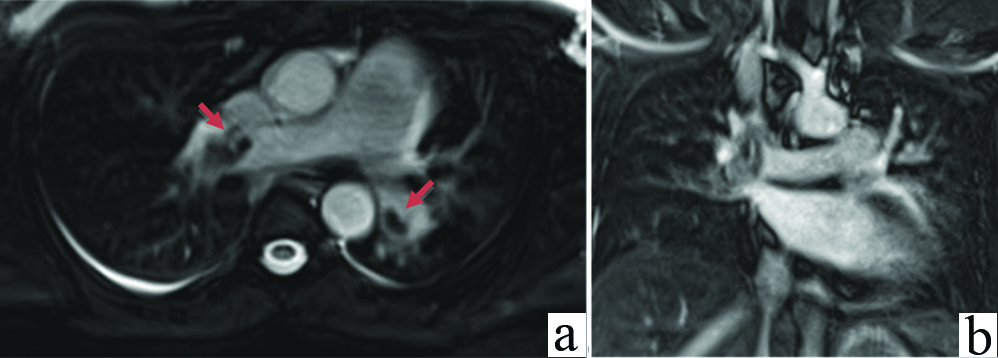
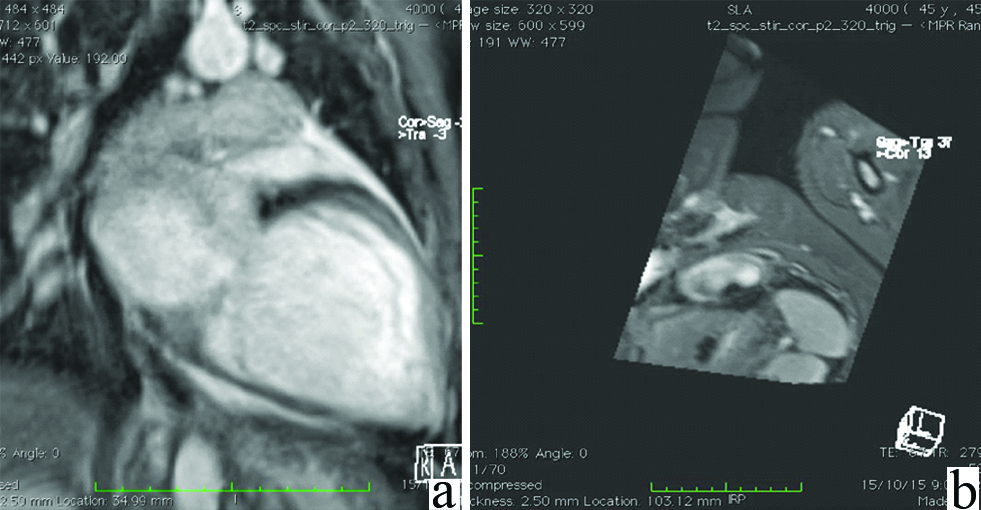
A 46-year-old male who has dyspnea, chest pain shows: (a) coronal T2 SPACE STIR; and (b) axial TRUFI shows aneurysmal dilatation of right atrium and pericardial effusion (red arrows).
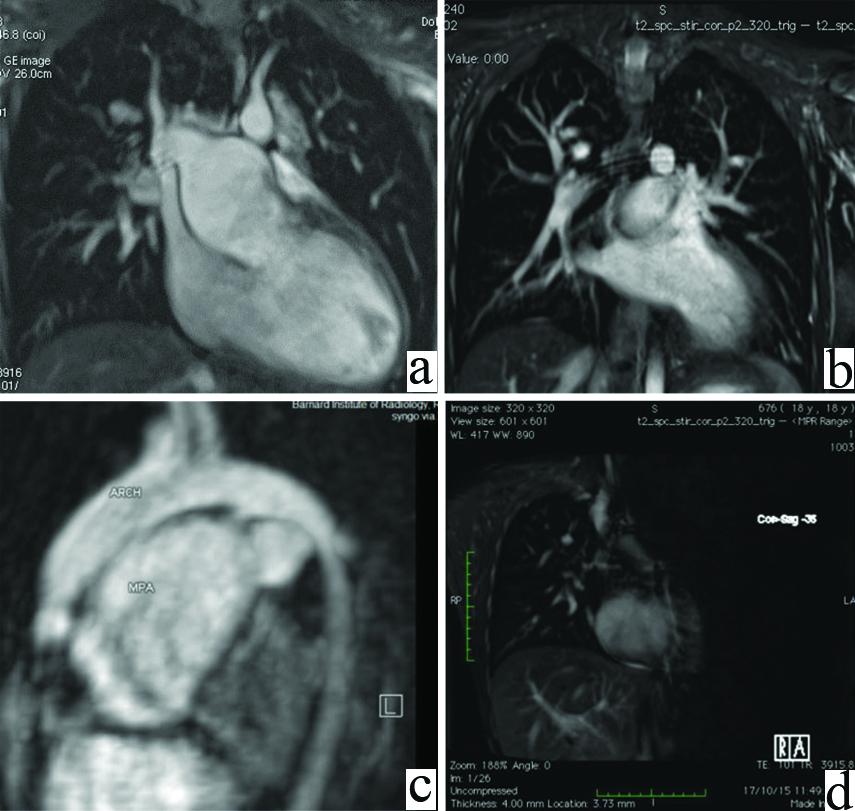
Common Ventricle with TGA. An 18-year-old male who has dyspnea, chest pain. (a,b) Coronal T2 SPACE STIR and (c) reformatted sagittal images shows Common Ventricle- Double inlet left ventricle with transposition of great arteries and tubular right ventricle. Pulmonary Stenosis with Significantly Dilated Main Pulmonary Artery (d) T2SPACE STIR oblique coronal and axial reformatted images in movie formats showing Double Inlet Left Ventricle With Tubular Right Ventricle.
Tetralogy of fallot. A 14-year-old male, (a,b) coronal and axial (c,d) reformatted T2 SPACE STIR images shows overriding of aorta, right ventricular hypertrophy, VSD, and hypoplastic right and left pulmonary arteries respectively.
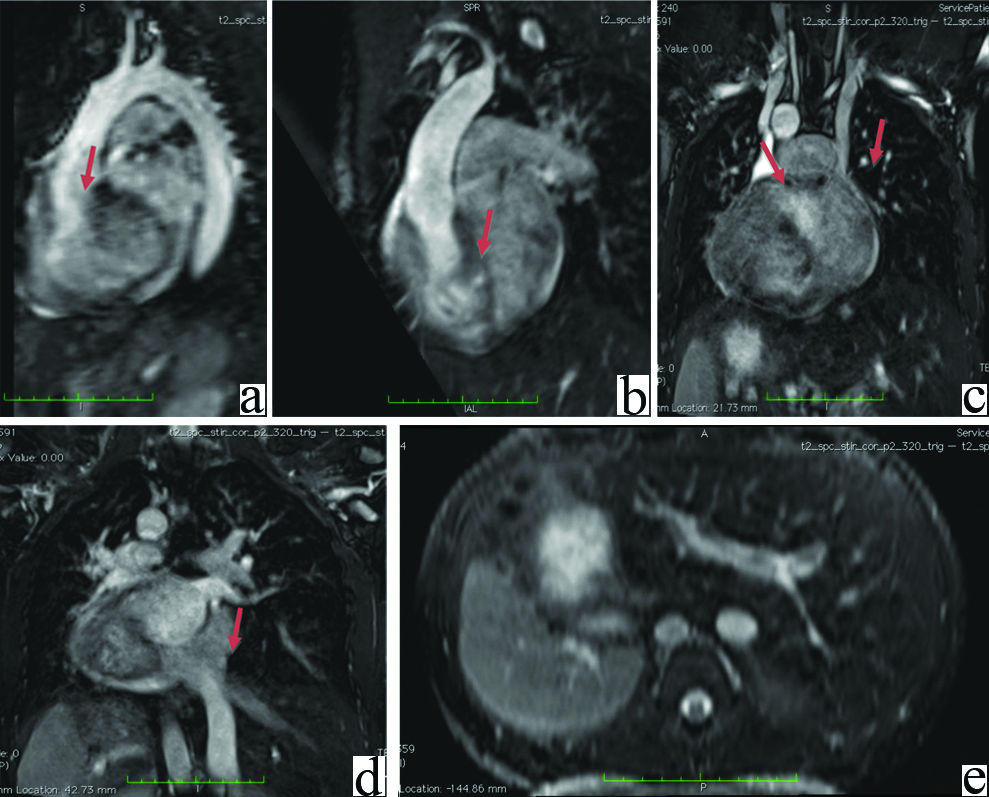
Situs inversus totalis with corrected transposition of great vessels, COR triatrium, right aortic arch and double SVC.
A 3D T2 SPACE STIR (a&b) oblique reformatted image and, (c&d) coronal shows origin of aorta from morphological right ventricle, Double Svc–Right sided SVC drains into Right Sided left Atrium, Left sided SVC drains into Left Sided Right Atrium with IVC and (e) Axial images demonstrating situsi nversus totalis
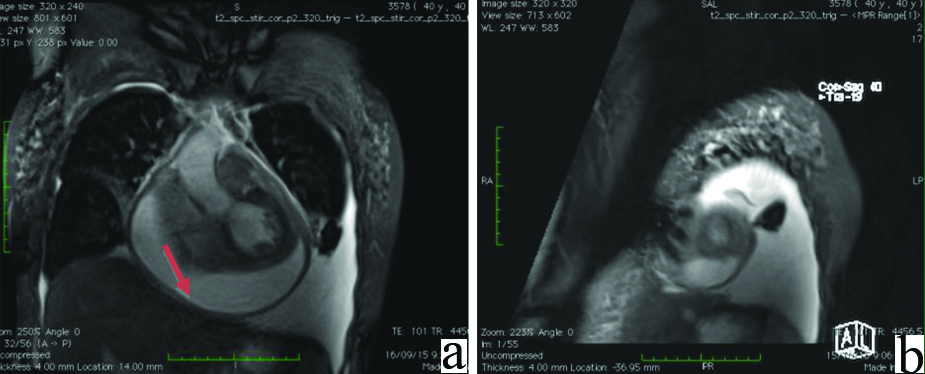
Constrictive pericarditis. A 40-year-old male with chest pain, a) coronal T2 SPACE STIR image and b) 3D SPACE STIR oblique short axis reformatted images in movie format shows pericardial effusion with diffuse mild pericardial thickening of 4 mm with paradoxical septum.
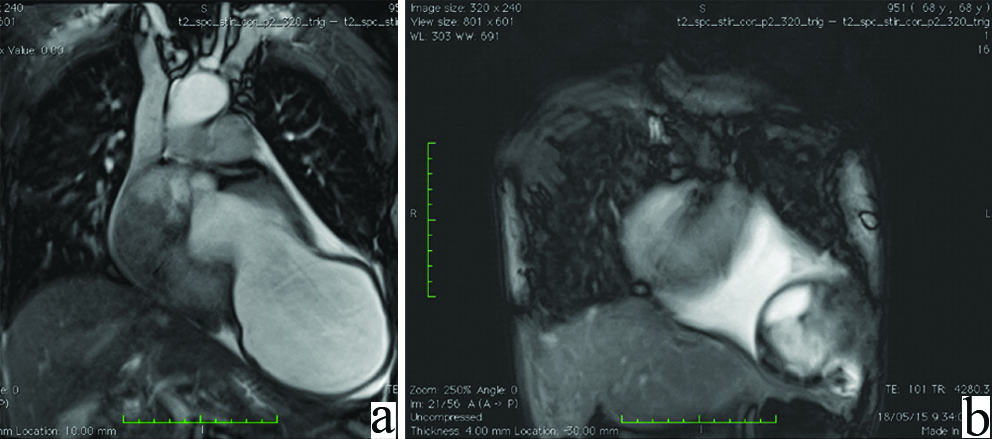
Left ventricle aneurysm with clot. A 64-year-old male: (a) coronal T2 SPACE STIR image and (b) movie format shows Large left ventricle apical aneurysm with small clot, Significant hypokinesia of left ventricle and Minimal Bilateral pleural effusion.
Dilated-cardiomyopathy.
A 3D T2 SPACE STIR: (a) oblique reformatted image and (b) reformatted short axis images in movie format shows dilated left ventricle showing global hypokinesia.
Known case of CA left breast with lung METS.
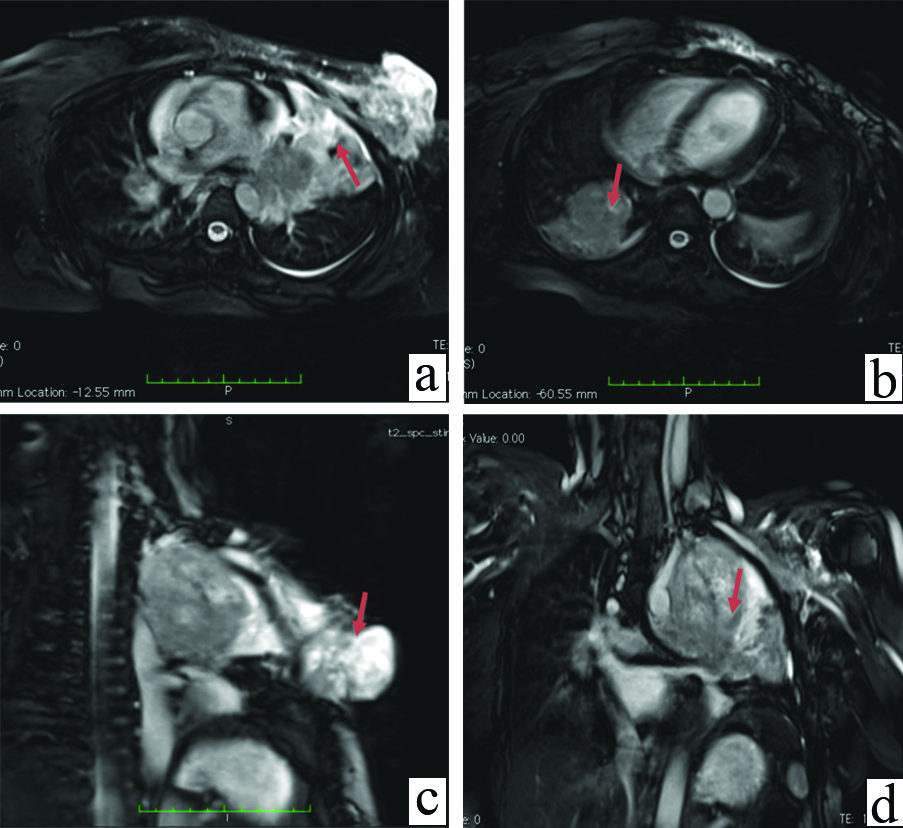
A 3D T2 SPACE STIR (a&b) Axial, (c&d) oblique reformatted image and coronal images shows left breast mass invading the pectoral muscles consistent with carcinoma and left upper lobe lung mass suggestive of metastases (red arrows).
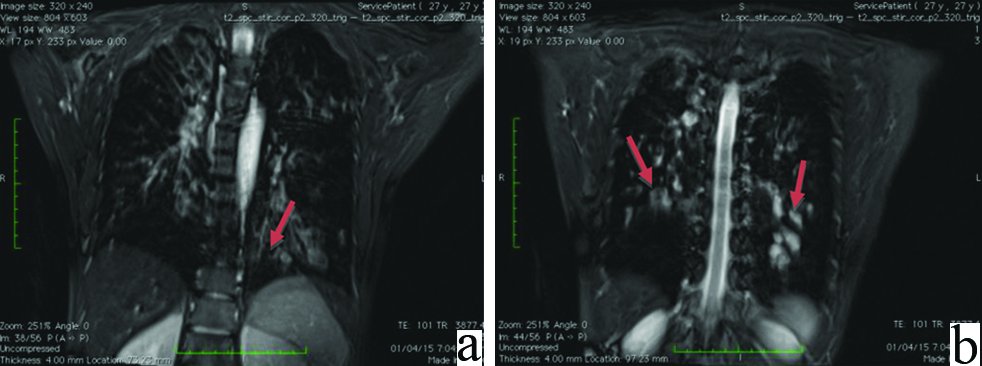
Bronchiectasis. A 27-year-old female antenatal patient who has dyspnea, cough. Coronal T2 STIR SPACE images (a & b) shows bronchiectasis, peribronchial wall thickening and mucoid plugging (red arrow) in both lower lobes.
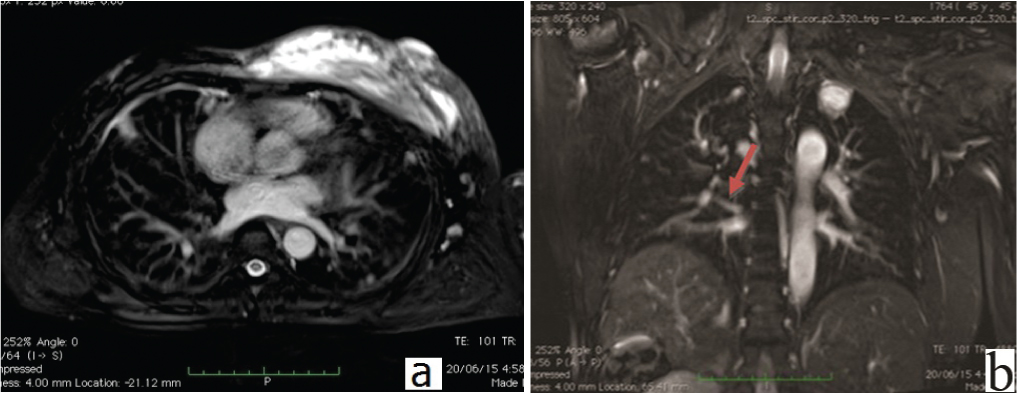
Pulmonary tuberculosis. A 45-year-old renal failure male who had cough, chest wall swelling. Axial (a) and coronal (b) T2 SPACE stir images shows hyper intense collection in left anterior chest wall (red arrow) and few random hyper intense nodules (red arrow) in both lung fields suggestive of active infection.
Isotropic 3D reconstructed images can be obtained in any plane similar to CT, which was not possible with earlier 2D MRI sequences. Space STIR MRI Sequence is a single sequence from which multiplanar reconstructions of any required orientation is done by post processing. Thus by obtaining images in any plane even after the MRI examination, it provides a useful tool for radiologist. To our knowledge, studies on 3D Space STIR MRI technique was done in brachial plexus [2], neuroimaging [3,4], and abdominal [9], pelvis [10], body trunk MR imaging [11] but not in cardiovascular and chest imaging. This study reflects our initial clinical experiences with imaging cardiovascular and chest patients. Multichamber views of the heart can also be easily obtained as demonstrated in [Table/Fig-6,7], depicting the features of Tetralogy of Fallot and Corrected Transposition of Great Vessels, CorTriatrium, Right Aortic Arch and Double SVC respectively. Morphological anatomy of great vessels, cardiac chambers and pericardium can thus be assessed with good resolution. This sequence also helps in the evaluation of pericarditis, left ventricular thrombi, dilated cardiomyopathy, etc. as shown in [Table/Fig-8,9 and 10]. Apart from cardiac conditions, chest pathologies such as bronchiectasis, metastases, chest wall masses also diagnosed with this sequence as shown in [Table/Fig-11,12 and 13]. Results of our study shows time duration taken for routine MRI scan is 20.2 minutes and for 3D Space Stir MRI Sequence is 5.8 minutes which is in accordance with Nicole Proscia et al., [10]. Thus, statistically highly significant time differences between time taken for routine MRI scan and 3D Space STIR MRI Sequences helps the dyspneic or fragile patients whom MRI could not be done for long time, this T2 STIR sequence aids in diagnosis with short time.
Limitation
The average time duration depends upon the respiratory and cardiac status of the patient, since it is done under gating. Hence the image resolution may not be the same in all cases. Another limitation is the lack of a reference test in our subjects which reflects the concern of radiation.
Conclusion
A 3D SPACE STIR MRI sequence gives better image quality which aids in diagnosis of cardiopulmonary pathology. A 3D SPACE STIR MRI also takes approximately four times lesser than the conventional sequences so the patient who cannot lay down for prolonged time in gantry can also be benefitted. It was also beneficial in patients with renal failure and pregnant patients where contrast studies and CT is contraindicated, 3D SPACE STIR T2 imaging adds value in diagnosing pulmonary thromboembolism, congenital heart disease with very less sequence acquisition time.