Inferior Accessory Ossicle of Anterior Arch of Atlas: Case Report with 3D Visualisation
Rahul Dev1, Pankaj Sharma2, Yasrab Khan3
1 Assistant Professor, Department of Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
2 Associate Professor, Department of Radiodiagnosis and Imaging, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
3 Senior Resident, Department of Radiodiagnosis, Delhi State Cancer Institute, Dilshad Garden, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rahul Dev, Flat no-5/1, Fifth Floor, Building No. 57, AIIMS Rishikesh Residential complex, Rishikesh, Uttarakhand-249203, India.
E-mail: rdev8283@gmail.com
Inferior accessory ossicle of anterior arch of atlas is a rare, albeit normal variant in relation to the cervical spine, invariably detected incidentally while investigating for other unrelated condition. Its existence should always be kept in mind while evaluating any bony fragment in relation to atlas axis vertebrae so as to avoid unnecessary investigation in suspicion of other sinister aetiology. The presence of well-cortical margins, constant size and shape over a course of time, constant position in close relation to anterior atlas arch, normal appearing pre-paravertebral soft tissue are indicators of its presence. We present a case of this anatomical variant detected incidentally in an old man investigated for oral malignancy.
Atlas, Accessory, Ossicle, Sesamoid
Case Report
Although the inferior accessory ossicle of the anterior arch of atlas is a normal variant, it is a very rare finding with only few cases reported in literature till date. It is important to be familiar with this skeletal variant, as it can be mistaken for other entities like previous traumatic, infective, or degenerative changes and unnecessary investigations or treatment can be avoided. In our case, this ossicle was found as an incidental finding while evaluating a dissimilar pathology. We illustrate it on MDCT (Multidetector Computed Tomography) with a first-time depiction on three-dimensional volume-rendered images. A 38-year-old man, a known case of carcinoma base of the tongue, was referred to our department for the evaluation of the extent of lesion on radiological imaging. The patient had no history of pain in neck, craniocervical trauma, pyrexia, or recent upper respiratory tract ailment. On examination, there was no evidence of restriction in neck mobility and he had unremarkable laboratory parameters including White Blood Cell (WBC) and C-Reactive Protein (CRP) count. The patient was evaluated with MDCT, and axial scans were obtained with coronal and sagittal reconstruction. On soft-tissue window, the images showed a hyperdense focus with inconspicuous superior margin seen to lie just below the anterior atlas arch with no evidence of any prevertebral soft tissue swelling [Table/Fig-1]. Bone window images revealed a well-defined triangular-shaped bony spicule with distinct corticated margin [Table/Fig-2]. The bony spicule was seen to be positioned upside down with the base directed superiorly articulating with the inferior margin of anterior atlas arch with a clear space between the two and the apex directed inferiorly. There was neither any evidence of associated fractures involving the cervical vertebrae nor any osteoarthritic changes [Table/Fig-3]. The morphology of the ossicle remained unremarkable during the course of time while the patient was undergoing appropriate treatment.
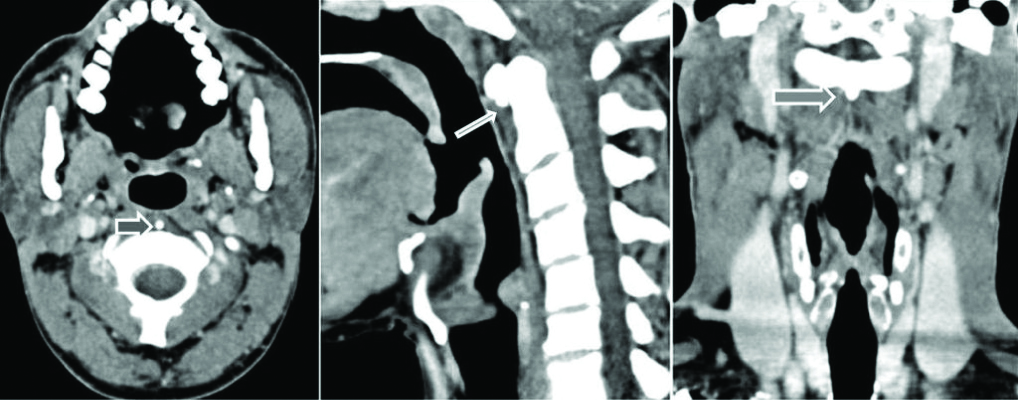
Images on soft tissue window reveal a hyperdense focus (black and white arrows) below the anterior arch of atlas with inconspicuous superior margin and no prevertebral soft tissue swelling.
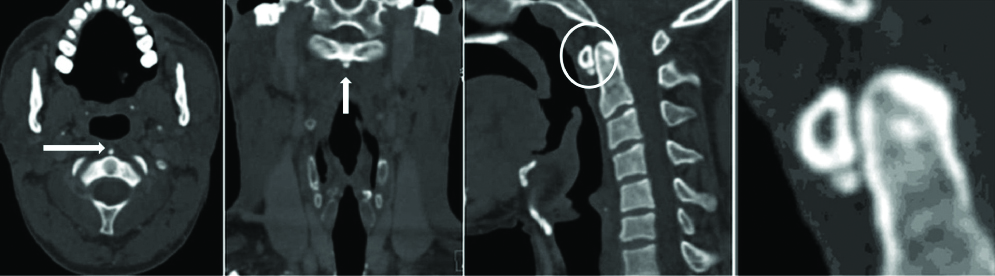
Bone Window images reveal well defined ossicle (white arrows and white circle) inferior to anterior arch of atlas separated from it by a clear space (magnified image).
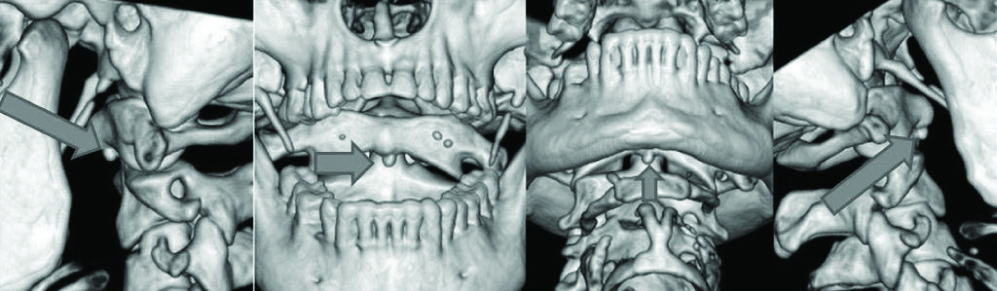
Three dimensional volume rendered image shows a conspicuous visualisation of the ossicle (thick black arrows) having smooth outline.
Discussion
The first description about this skeletal variant can be traced down to “Borderlands of normal and early pathologic findings” by Kohler A et al., which was published in 1956 [1]. However, the first exact description of this entity in terms of its development, the probable site of origin, location, morphology, and nomenclature was given by Keats TE in 1967 [2]. Farman AG et al., described the anatomical variations involving atlas in terms of superior articular processes, arches, and ossicles, with three patients having accessory ossicles above the posterior arch of the atlas [3]. Wysocki J et al., described the variants of all cervical vertebrae with particular emphasis on the occurrence of accessory bony processes arising from the posterior arch, lateral masses, or transverse processes in a considerable number of cases [4]. The developmental basis of the atlas was mentioned in 1981 by Cone RO et al., [5]. It was reported that during the early weeks of the embryonic period, paraxial mesoderm develops into sclerotomes with, in turn, a fusion of adjacent portions of the sclerotomes giving rise to the vertebral bodies, with the fourth occipital and first cervical sclerotomes being designated origins of the primitive atlas. Furthermore, the primitive atlas was attributed to be the origin of arch anomalies. As far as diagnostic dilemma is considered, this entity is to be differentiated from other inflammatory, traumatic, or degenerative pathologies. Haun CL elaborated four cases of calcific retropharyngeal tendinitis, which presents acutely and is associated with neck pain and restricted neck mobility [6]. It was also pointed out that this pathology shows amorphous calcification that dissolves rapidly in due course of time. Similar findings were also described by Bladt O et al., with additional imaging findings of fluid collection in retropharyngeal space, loss of lordosis and recent upper respiratory ailment [7]. The inferior accessory ossicle of the atlas is defined by its sharp cortical outline, definite shape, location just below the anterior arch and articulation with the inferior margin of the atlas and no evidence of adjacent soft-tissue swelling, as mentioned in a recent similar article by Naji MF et al., [8]. Another article cited by Whang CS et al., illustrated the ossicle with additional important remark regarding constant position of ossicle during neck movement as depicted in flexion extension radiographs [9]. An important facet arises in the setting of trauma where the fracture fragment morphology is being described as jagged margins devoid of shell outline superiorly and associated soft-tissue tumescence by Rao SK et al., [10]. The importance of this existence was further emphasised in a study conducted by Nunez Jr DB et al., depicting that nearly half of the undetected cervical spine fractures were reminisce to first two vertebrae [11].
Conclusion
Inferior accessory ossicle of anterior arch of atlas is a rare, albeit normal variant invariably seen as an incidental finding. Its presence is to be kept in mind to avoid unnecessary investigations. No clinical or radiological evidence of trauma adds to confident diagnosis of the same.
[1]. Kohler A, Zimmer EA, Borderlands of the Normal and Early Pathologic in Skeletal Roentgenology 1956 85Tenth editionNew YorkGrune & Stratton Inc:206 [Google Scholar]
[2]. Keats TE, The inferior accessory ossicle of the anterior arch of the atlasAm J Roentgenol 1967 101(4):834-36.10.2214/ajr.101.4.834 [Google Scholar] [CrossRef]
[3]. Farman AG, Nortje CJ, Joubert J, Radiographic profile of the first cervical vertebraJournal of Anatomy 1979 128(Pt3):595-600. [Google Scholar]
[4]. Wysocki J, Bubrowski M, Reymond J, Anatomical variants of the cervical vertebrae and the first thoracic vertebra in manFolia Morphol 2003 62(4):357-63. [Google Scholar]
[5]. Cone RO, Flournoy J, Macpherson RI, The craniocervical junctionRadioGraphics 1981 1(2):1-37.10.1148/radiographics.1.2.1 [Google Scholar] [CrossRef]
[6]. Haun CL, Retropharyngeal TendinitisAm J Roentgenol 1978 130:1137-40.10.2214/ajr.130.6.1137 [Google Scholar] [CrossRef]
[7]. Bladt O, Vanhoenacker P, Bevernage Ch, Van OM, Van HL, Haenens PD, Acute Calcific Prevertebral TendinitisJBR-BTR 2008 91:158-59. [Google Scholar]
[8]. Naji MF, Bhat R, The typical appearance of the inferior accessory ossicle of the anterior arch of the atlasSurg Radiol Anat 2009 31:69-71.10.1007/s00276-008-0393-718651090 [Google Scholar] [CrossRef] [PubMed]
[9]. Whang CS, Chung PH, Suh KJ, Kang S, Kim JP, Kim YS, Inferior accessory ossicle of the anterior arch of the atlasJ Korean Orthop Assoc 2010 45(3):234-37.10.4055/jkoa.2010.45.3.234 [Google Scholar] [CrossRef]
[10]. Rao SK, Wasyliw C, Nunez DB Jr, Spectrum of imaging findings in hyperextension injuries of the neckRadiographics 2005 25:1239-54.10.1148/rg.25504516216160109 [Google Scholar] [CrossRef] [PubMed]
[11]. Nunez Jr DB, Zuluaga A, Fuentes-Bernardo DA, Rivas LA, Becerra JL, Cervical spine trauma: how much more do we learn by routinely using helical CTRadiographics 1996 16:1307-18.10.1148/radiographics.16.6.89465378946537 [Google Scholar] [CrossRef] [PubMed]