A Rare Massive Pulmonary Chondroid Hamartoma
Nazneen Abdul Kader1, Minnu Khadeeja2, PP Sathi3
1 Senior Resident, Department of Pathology, Government Medical College, Kozhikode, Kerala, India.
2 Junior Resident, Department of Pathology, Government Medical College, Kozhikode, Kerala, India.
3 Professor and Head, Department of Pathology, Government Medical College, Kozhikode, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nazneen Abdul Kader, Senior Resident, Department of Pathology, Government Medical College, Kozhikode-673008, Kerala, India.
E-mail: neenu_eeman@yahoo.com
Hamartomas are disorganised but benign masses composed of cells indigenous to the involved site. They are the tumourous lesion consisting of anomalously arranged tissues that are components of the normal lung, such as cartilage, fat, smooth muscle, and tubules lined by bronchial or bronchiolar epithelium, which may be entrapped. Hamartoma is the most common benign tumour of the lung, accounting for 8% of pulmonary neoplasms. Here is a case of giant pulmonary chondroid hamartoma.
Benign lung tumour, Lung neoplasm, Solitary lung lesion
Case Report
A 53-year-old male patient presented with severe progressive exertional dyspnoea and cough for one year. The cough was non purulent and was associated with throbbing pain in left chest. He was not on any medication and did not have any history of previous illnesses. On examination, he had pallor. Vitals were stable. A mass was palpated in the left hypochondrium, the upper border of which was not discernible. The mass roughly measured 7cm; the medial and lower borders were well made out. The mass was firm, nontender, bosselated, ballotable, moving with respiration and was dull on percussion. His routine blood investigations were normal. X-ray showed a well circumscribed mass, with calcifications in the left lung, pushing the heart to opposite side [Table/Fig-1a]. CT thorax showed a non-enhancing lesion in the left hemithorax with fat density areas and chunk calcifications, with absent fat plane between the lesion and left ventricle [Table/Fig-1b]. The lesion was confined to the hemithorax with no infiltration to the adjacent organs. MRI ruled out pericardial infiltration [Table/Fig-1c].
a) X-ray showing a well circumscribed mass with irregular white ‘popcorn’ calcifications, in the left lung; b) CT thorax showing a lesion with fat density areas and chunk calcifications; c) MRI ruled out pericardial infiltration d) Grossly, a well circumscribed grey white, gritty mass measuring 12×10×11 cm.
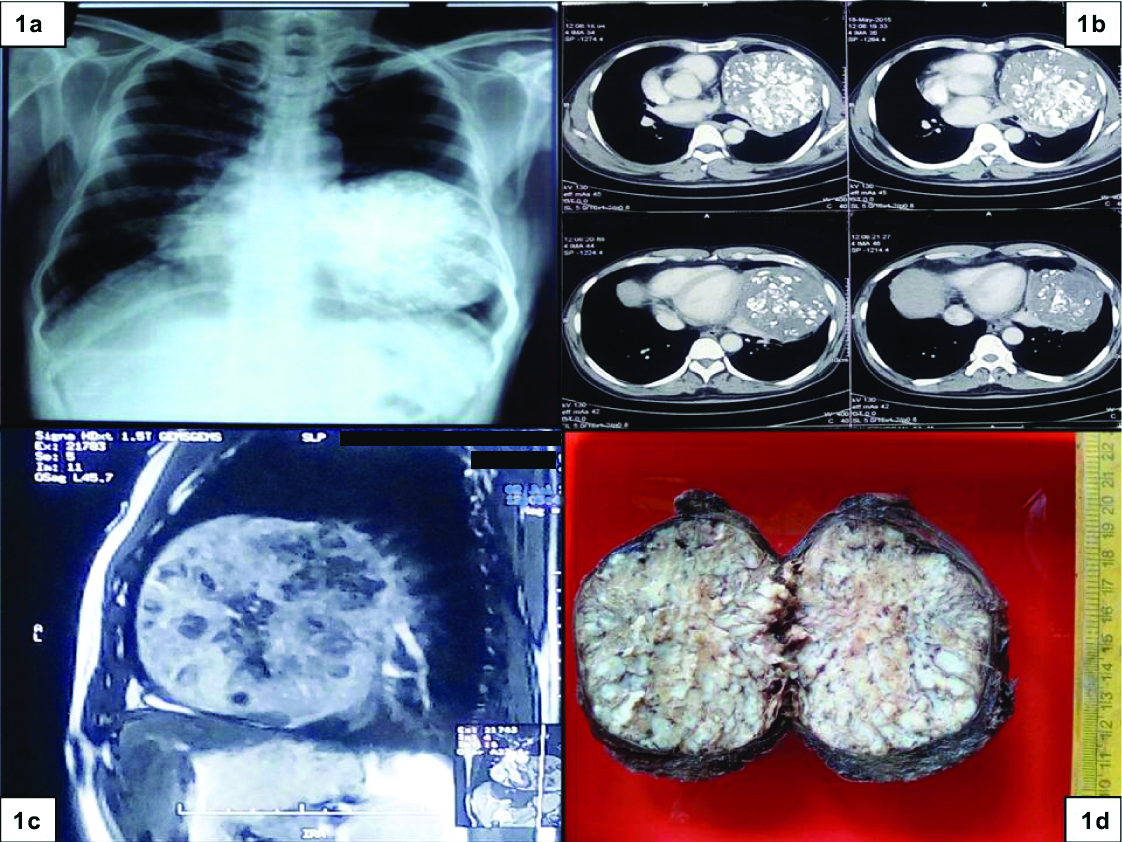
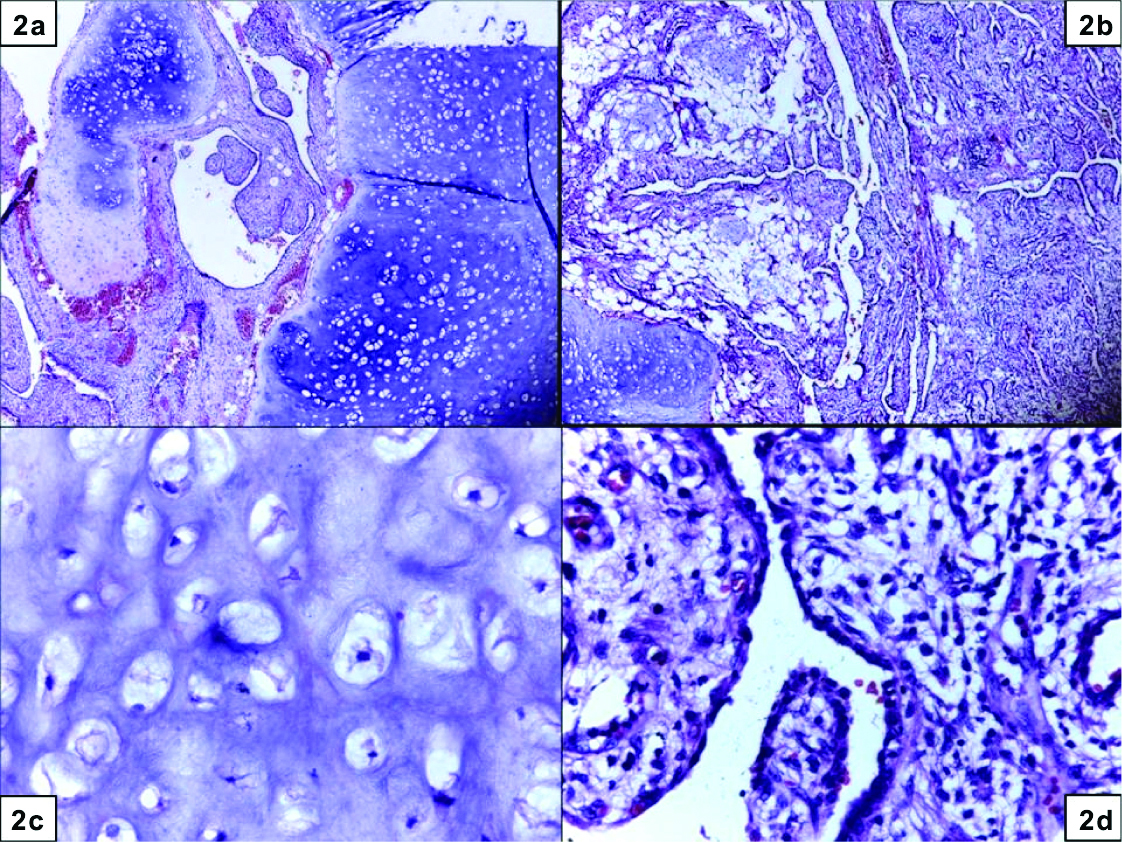
With the provisional diagnosis of pulmonary hamartoma, surgeon proceeded with left upper lobectomy. We received enlarged lobe of lung. On cut section, a well circumscribed, grey white, gritty mass measuring 12×10×11 cm was seen, not reaching up to the pleural margin [Table/Fig-1d]. The adjacent lung and bronchus were unremarkable. Microscopy showed lobules of mature cartilage [Table/Fig-2a,c], separated by adipose tissue [Table/Fig-2b] and non-ciliated cuboidal epithelium [Table/Fig-2d].The epithelial cells show TTF1 positivity.
H&E stained microscopy showed lobules of mature cartilage (10X); a) separated by adipose tissue (5X) b) mature benign cartilage (40X); c) and non-ciliated cuboidal epithelium with benign nuclear features (40X) d).
After the surgery, the patient is asymptomatic and doing well for the past two years.
Discussion
The term hamartoma refers to a disordered nodular collection of benign tissue normally present in other organs [1]. Pulmonary chondroid hamartoma, also known as chondroid adenoma, chondroma, and benign mesenchymoma generally occurs in adults and is more common in males [2]. Most patients with hamartoma are older than 40 years, and the male-to-female ratio is about 1:2 [3]. Hamartomas are usually located in a peripheral parenchymal location [4]. Pulmonary hamartomas can be divided into parenchymal (90%) and endobronchial (10%) types [4]. Hamartoma occurs mostly as a solitary nodule [3]. Most patients are asymptomatic, and the lesion is often found on X-ray during a routine checkup [3]. The lesion is characterised by “popcorn” calcification on radiographic examination in one third of cases [1].
Grossly, these hamartomata are lobulated, firm masses that “shell out” from the surrounding parenchyma. The cut surface shows glistening nodules of cartilage, with specks of dystrophic calcification or bone, separated by ill-defined clefts.
Microscopically, these tumours are composed of lobulated masses of mature cartilage surrounded by fat, smooth muscle, bone, and fibrovascular tissue. Clefts are lined by ciliated or nonciliated respiratory epithelium [4]. The diagnosis is made with the characteristic growth pattern and on finding at least two benign mesenchymal tissues in the lesion. The presence of only one mesenchymal tissue type raises the possibility of lipoma, leiomyoma, or chondroma [2]. Cytogenetically, pulmonary hamartoma shows rearrangements of chromosome 6p21 or chromosome 12q14-15 (involving HMGA1 or HMGA2 genes respectively), supporting the neoplastic nature of this process [2].
Usually these tumours grow slowly; malignant transformation is extremely rare [4]. Multiple pulmonary chondroid hamartoma are rare and represent Cowden syndrome or Carney triad. Cowden syndrome is characterised by multiple benign tumours of internal organs, mucocutaneous lesions, and increased risk for breast, thyroid, urogenital and digestive tract cancers. Carney triad is characterised by the association of gastrointestinal stromal tumours, pulmonary chondroid hamartoma and extra-adrenal paraganglioma [2].
The differential diagnoses to be considered are lipoma, carcinoid tumour, solitary metastasis to lung. The largest pulmonary chondroid hamartoma published to the best of authors’ knowledge measures 20 cm [5]. No other case larger than current lesion was found in the literature.
Conclusion
It is very important to keep the possibility of hamartoma in mind, while dealing with solitary pulmonary tumours and to distinguish them from malignancy.
[1]. Van den Bosch JM, Wagenaar SS, Corrin B, Elbers JR, Knaepen PJ, Westermann CJ, Mesenchymoma of the lung (so-called hamartoma): a review of 154 parenchymal and endobronchial casesThorax 1987 42:790-93.10.1136/thx.42.10.7903321538 [Google Scholar] [CrossRef] [PubMed]
[2]. Tumours of lungs and pleura, Rosai and Ackerman’s surgical pathology10th edition:385-86. [Google Scholar]
[3]. Masayuki Noguchi, Yukio Shimosato, Pulmonary neoplasmsSternberg’s diagnostic surgical pathology5th edition:1085 [Google Scholar]
[4]. Nicholson AG, Tomashefski JF Jr, Popper H, HamartomaWHO classification-Tumours of the Lung, Pleura, Thymus and Heart 2004 :113-114. [Google Scholar]
[5]. Lio E, Aisner DL, Askin FB, Kwak JJ, Giant pulmonary chondroid hamartoma: imaging and pathology correlation of a rare tumour demonstrated with bone scintigraphy and 18F-FDG PET/CTClin Nucl Med 2015 40(1):79-81.10.1097/RLU.000000000000059925275419 [Google Scholar] [CrossRef] [PubMed]