Anterior Knee Pain (AKP) or Patella Femoral Pain Syndrome (PFPS) is defined by mild aching pain localised around peripatellar area which aggravate by physical activities like climbing stairs, squatting, jumping, running and/or by sitting with the knees flexed for prolonged periods of time [1]. It accounts for 25% of all knee pain encountered in sports medicine clinics [1]. It is commonest diagnoses among young, physically active populations, affects 25% athletes, with >70% of them between age of 16 and 25-year-old. This respond well to physiotherapy but has high incidence of relapse in two-thirds which leads to activity modification and long medical treatment [2].
The main anatomical structures responsible for AKP are subchondral bone, synovium, retinaculum, skin, muscle/tendon, and nerve. These structures may be affected by many factors, including systemic disease, but in orthopaedic, the most common reasons for AKP are patellofemoral malalignment, overuse and trauma [3]. A common tool used to assess such patellar malalignment is the Q-angle [4].
Various studies suggest that there is a significant association between AKP and Q-angle [5-9]. Most of the studies done are from western population who have body morphology and physical activities different from Southeast Asian population, and hence its validity in present population is largely unknown. So in this prospective comparative study, authors have tried to find the relationship between AKP and Q-angle and the normal range of Q-angle in Nepalese population.
Materials and Methods
This prospective, comparative study was conducted in Tribhuvan University Teaching Hospital, Institute of Medicine, Maharajgunj, Kathmandu, Nepal from March 2014 to Octber 2015 after approval from Institutional Review Board. The investigation of patients of AKP was done in orthopaedics Outpatient Department (OPD) of the institute. The patients who met the inclusion criteria were then consented to take part in this study. The inclusion criteria was, age 15-35 years with AKP. The patient who had a history of trauma, known ankle, hip, spine pathology, gross knee deformity, previous knee surgery, with ligament laxity, meniscal and ligamentous injury and congenital anomalies of lower extremity were excluded from the study. The member of the control group was selected in the OPD with different unrelated problem in the upper extremity with no history of AKP were taken up for study. They were aged 15-35 years and gave consent to participate in this study.
All possible demographic details like age, gender, occupation, height, weight and Body Mass Index (BMI) were obtained for both case and control group. The Q-angle of knee was measured for all participants by three independent examiners who were unaware of the values obtained by each other, using a universal goniometer in standing position. The anterior superior iliac spine, the centre of the patella and the tibial tubercle was located manually and marked with a removable skin marker pen. The subject was instructed to hold one end of a string at the anterior superior iliac spine. The other end of the string was taped just inferior to the midpoint of the patella, such that the pen mark was still visible. The centre of the goniometer was placed at the midpoint of the patella. One arm of the goniometer was aligned with the string leading to the anterior superior iliac spine, and the other arm of the goniometer was aligned with the tibial tubercle [4]. Three measurements were taken (one time by each examiner) and average of these three was recorded as final measurement.
Statistical Analysis
The collected data were entered in the datasheet for further analysis. SPSS-17 was used for data analysis and interpretation. Authors then correlated the Q-angle of case with the control using Student’s t-test. Authors have also correlated the various demographic parameters with the Q-angle using regression analysis. For all statistical purposes the p<0.05 was taken as significant.
Results
Scrutiny of 142 cases of patients with AKP was done in OPD. After history and clinical examination, 12 had a history of trauma to knee, four had malunited femur fracture, three had fracture of tibia, five patients had deformity at the hip and 18 patients refused to take part in the study. Finally, study was conducted on 100 cases (122 knees) and assigned as Group A. For better comparability, 100 subjects without AKP in control group were taken and assigned as Group B. In Group A there were 48 (48%) male and 52 (52%) female cases, whereas male and female in control group were in equal proportion. As far as laterality is concerned, left to right knee involvement in Group A was 1:1 (60:62). So in order to make the comparing group homogenous, the ratio of right to left knee was taken in the ratio of 1:1 (50:50) in Group B. The mean age was 25.5±5.7 (range 15-35) years versus 25.4±6.1 (range 15-35) years (p=0.9); mean height 162.8 cm versus 164.1 cm; mean weight 62.6 kg versus 63.3 kg; mean BMI 23.5 kg/m2 versus 23.3 kg/m2 in Group A and Group B respectively. The mean duration of pain was 7.1±5.1 (range 2-24) months [Table/Fig-1]. There were 48 students, 24 housewifes, 12 farmer, five defense service holder, four teachers and seven daily wage labourer in Group A.
Showing different demographic variables and Q-angle.
| Characteristics | Group A | Group B | p-value |
|---|
| Age | 25.5 years | 25.4 years | 0.9 |
| Male: Female | 0.9:1 | 1:1 | 0.9 |
| Height | 162.8 cm | 164.1 cm | 0.06 |
| Weight | 62.6 kg | 63.3 kg | 0.9 |
| BMI | 23.5 kg/m2 | 23.3 kg/m2 | 0.3 |
| Q-angle | 17.9° | 14.3° | <0.05* |
BMI: Body mass index; Q-angle: Quadricep angle
*Difference is significant
p-value obtained by unpaired t-test
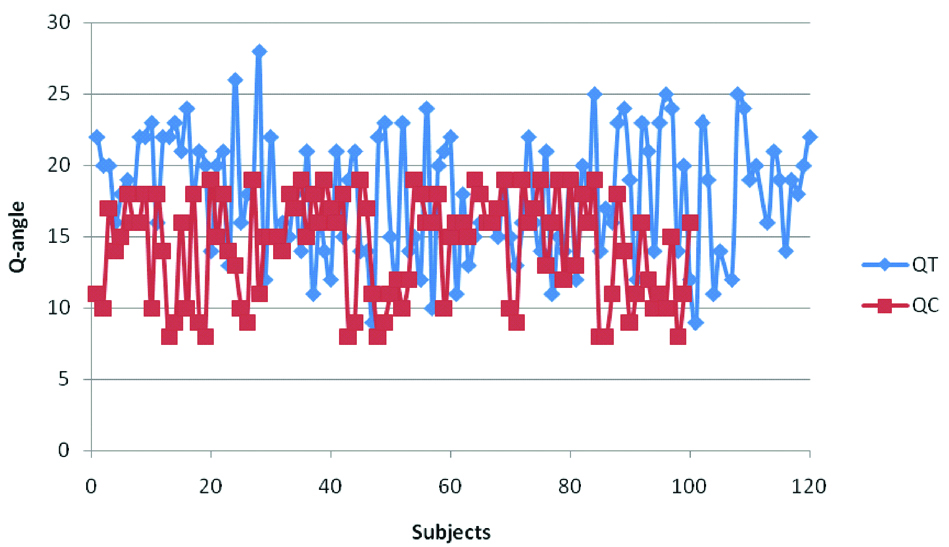
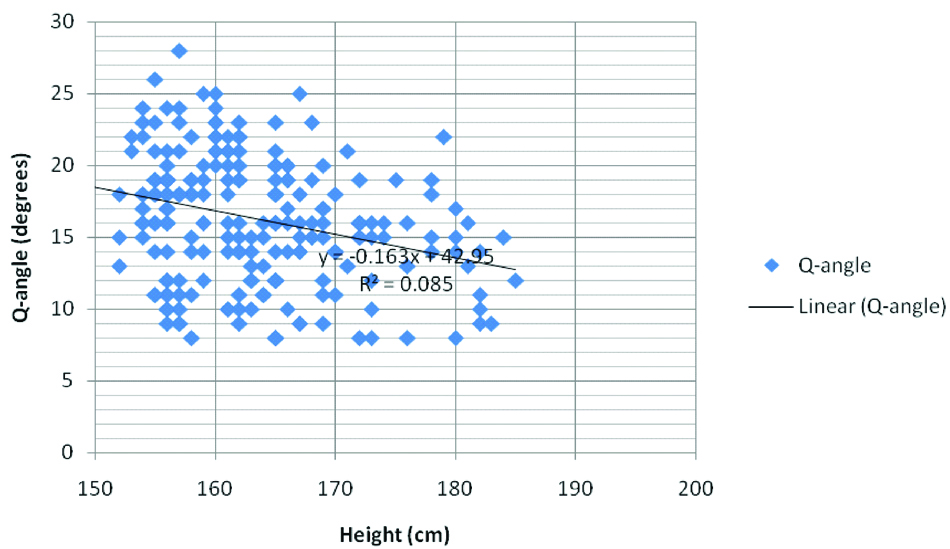
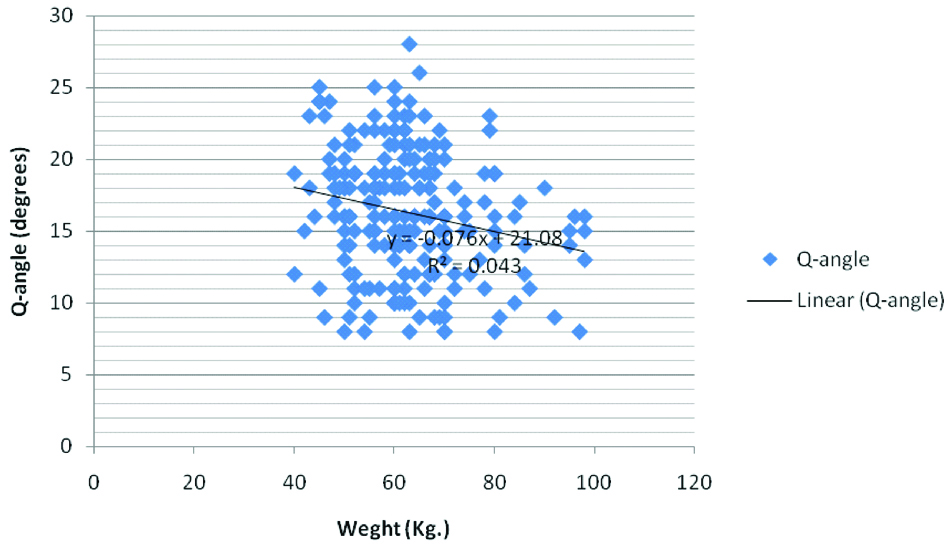
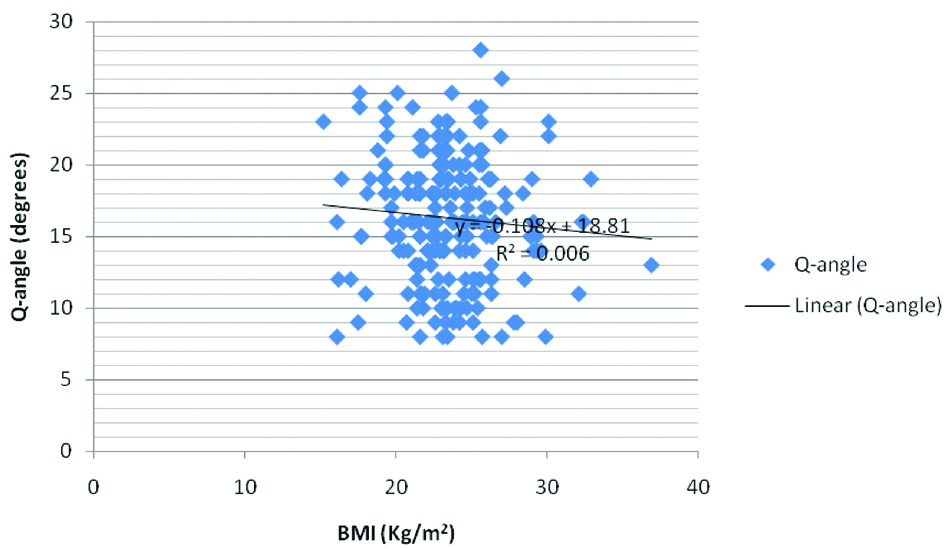
The mean Q-angle was 17.9±4.2 (range 9-28) versus 14.3±3.6 (range 8-19) in Group A and Group B respectively [Table/Fig-1,2]. This difference was found statistically significant (p<0.05). On regression analysis to evaluate the correlation between demographic parameters (height, weight and BMI) and Q-angle was done and there the significant correlation was found between height (r=-0.21; p<0.05) [Table/Fig-3] and weight (r=-0.29; p<0.05) [Table/Fig-4] with Q-angle, however, the subjects of both groups were combined. Authors did not find significant correlation between BMI and Q-angle (r=-0.08; p=0.2) [Table/Fig-5].
Showing distribution of Q-angle in case and control group.
Showing a significant correlation but weak association between Q angle and height (r=-0.2; p<0.05)
Showing a significant correlation and weak association between weight and Q-angle (r=-0.29; p<0.05).
Showing correlation between BMI and Q-angle, which is not significant (r=-0.08; p=0.2).
Discussion
The terms AKP and PFPS are often used interchangeably to describe pain in the anterior part of the knee [10]. “Runner’s knee,” chondromalacia patella, AKP, and patellofemoral syndrome are common synonyms and none then accurately describes the underlying pathology [11]. AKP is common problem experienced by patients requiring visit to the orthopaedic sports clinic. Abnormal patellar alignment is described to be one of the factors that cause such pain. A common tool used to assess such patellar malalignment is the Q-angle [4]. The Q-angle is defined as the acute angle formed by the vector for the combined pull of the quadriceps femoris muscle and the patellar tendon [12]. It is an acute angle between the line connecting the Anterior Superior Iliac Spine (ASIS) and the midpoint of the patella (representing the line of pull of the combined quadriceps femoris musculature) and the line connecting the tibial tubercle with the same reference point on the patella (representing the line of pull of the patellar tendon) [4]. The measurement of that angle can be performed using different methods, such as the radiographic method or clinically through the goniometer, and in different ways, having the patient in supine with knee in total extension and relaxed quadriceps, or contracted, knee 30° of flexion with quadriceps relaxed, sitting with the knee in a 90° flexion and in standing [13]. Averages Q angle in normal subject is about 14° in men and 17° in women [14].
However, author did not find gender-based difference in AKP in present study but the literature reveal incidence of AKP slightly more in female in the ratio of 1.4:1 to 2.2:1 [15-17]. The reason for higher incidence of knee pain in females may be due to increased pelvic width resulting in excessive lateral thrust on the patella, postural and sociological factors such as wearing high heels and sit with legs adducted [7,18]. The probable reason for not getting gender based difference in present study population is the built of the subjects which was almost similar in both the gender with BMI in normal range and females in South Asian society usually do not wear high heels and sit cross legged.
In this study mean age of case group was 25.5 years and control group was 25.4 years. Samuel RW et al., in their study reported similar finding with mean age of 25.1±3.4 years in symptomatic subject [19]. Shultz SJ et al., in their study reported similar finding with mean age 25.6±3.2 years in asymptomatic subject [20]. Caylor D et al., in their studies reported mean age 23 years in case and 24.5 years in control group [4]. The reason of more incidence of AKP in this age group could be because of them being the most active group, more participation in sports and outdoor professional and recreational activities thereby making them more prone to stress and strains and minor repetitive trauma [21,22].
In study by Biedert RM and Warnke K out of 34 cases 15 (44%) had bilateral involvement; The reason for more bilateral involvement in this study may be due to wide range of age group of the patients (11-44 years) [23]. In study by Haim A et al., out of 61 patients 53 (87%) had bilateral involvement [6]. The reason of more bilateral involvement in their study was maybe due to different population (soldiers). In contrast to above mentioned study, authors had only 22% had bilateral knee involvement, probably because of younger sample population, racial and geographical differences.
In this study, average duration of pain was 2 to 24 months with mean duration of 7.1 months. In study of Pekka AK the mean duration of pain was 16 months [24]. In study by Haim A et al., mean duration of pain was 19±4.9 months [6]. The result in present study may be due to severe pain interfering with daily activity (due to the geographic distribution, the social habits of eating food by cross legs on floor, traditional toilets, lacks roads requiring to prolong walking lead to more pain) leading to early medical attention and may be due to samplling size.
In this study mean Q-angle in the case group was 17.9° and in the control group, the angle was 14.3° respectively. These differences in Q-angle was statistically significant and was in line to study done by Aglietti P et al., (18° vs 15°), Haim A et al., (16.8° vs 12.5°), Emami MJ et al., (18° vs 14.9°), Agrawal J et al., (17.8° vs 14.1°), Abdel-aziem AA et al., (17.9° vs 11.9°) [5-9] and different from study by Caylor D et al., (12.4° vs 11.1°), Patil S et al., (11.2° vs 11°) and Turkmen F et al., (12.6° vs 13.6°) [4,18,25].
In this study, Q-angle of the control group (normal population) in men was 12.2° and women were 16.3 respectively and were in line to study done by Agrawal J et al., (12.3° and 15.9°) [8].
A high Q-angle means an abnormal high valgus angle which influences biomechanics patellofemoral articulation by exerting a laterally directed force leading to mal-tracking and excessive pressure on the patellofemoral articulation, consequently resulting in AKP [7]. High Q-angle results in dynamic component of lateral maltracking of patella which can be treated by stretching tight lateral structures (vastuslateralis, iliotibial band), strengthening medial structures {Vastus Medialis Obliquus (VMO)}, knee orthoses for patellar stabilisation, and foot orthoses to correct excessive subtalar pronation [26].
There are many studies which have correlated the demographic variables with Q-angles weight, authors found a significant correlation between height and weight with Q-angle, which is in line with the studies done by Jha A et al., found a correlation between height and Q-angle similar to the finding of Prakash V et al., [27,28]. However, authors did not find significant correlation between Q angle and BMI. Present finding is in contrary to the result of studies done by and Prakash V et al., probably they had more obese patient than our study [28].
Strength
The strengths of the study are the comparative study, focusing on the subjects of South Asian population, which has been studied in scanty. Further, the reference value of Q-angle obtained in the studies done in western population need to be studied in these populations with regard to its validity.
Limitation
There are some limitations like power of study was not calculated, researcher bias because the lead examiner could not be blinded to the patient’s complaints and diagnosis. The sample in this study is from a Southeast Asian country, and its validation in other countries requires further study.
Conclusion
On the basis of this study it can be concluded that the patient with Anterior Knee Pain (AKP) has higher Q-angle as compared to the normal population. The reference value of Q-angle in normal population can be considered as 12.2 in men and 16.3 women. So, individual with lower Q-angle are asymptomatic individual.
BMI: Body mass index; Q-angle: Quadricep angle
*Difference is significant
p-value obtained by unpaired t-test