Hearing impairment is one of the most common but still an under-reported chronic ailment in elderly population [1,2]. The age-related degeneration can also involve stria vascularis, the spiral ganglion [3], the cochlear nerve [4,5] or the central auditory processing of speech [6]. Hearing loss in elderly people is usually bilateral, symmetrical and progressive [7]. With changing demographic profile and increasing life expectancy, it is likely to become a major issue of concern. Hearing impairment has a considerable impact on their lifestyle. Presbycusis is the second most common cause of hearing loss following infective causes like Chronic Suppurative Otitis Media [8]. The prevalence of hearing disability in India is 41% in people over 60 years of age [9]. The prevalence of hearing loss is doubling, every 10 years [1].
There is an increasing need to study the impact of disease on daily activity and behaviour. Hearing difficulty in elderly interferes with communication and has a significant negative effect on the social and emotional aspect of life. Impaired communication causes a low self-esteem and poor self-perception of social skills. The hearing loss further adds to poor social life, impairing their day to day activities.
Hearing disability refers to the difficulties in hearing in a real environment such as hearing in noisy environments [10]. Hearing loss of more than 60 dB in the better ear is generally considered as a disabling hearing loss [11]. As most of the daily activities are dependent on hearing even lesser hearing loss can also interfere with certain activities restraining normal social or emotional well being. Hearing handicap, according to the WHO definition, refers to nonauditory consequences for an individual, such as experiences of emotional distress and restrictions on social engagement, directly due to hearing impairment [12-14]. Hearing impairment is measured using audiometry. However, hearing handicap is a more a complex phenomenon which can be measured using self-reported questionnaire on social and emotional aspects of life. There are various questionnaires to assess the hearing handicap in elderly people and only few of them are standardised. Of these, Hearing handicap Inventory for Elderly (HHIE) has been found to reliable, valid and simple to administer [15]. There is generally a tendency to ignore the hearing loss especially in elderly, which make it an under-reported condition. They neither seek medical advice nor use hearing assistive devices like hearing aid when prescribed leading to significant disability. In general, hearing of the people is assessed ignoring the handicap perceived by the people. Hearing handicap is a pivotal factor in influencing their health-seeking behaviour. Hence identifying people with self-perceived hearing handicap is more crucial that people with hearing impairment alone.
Several studies have demonstrated that hearing loss in elderly has a significant negative effect on quality of life [16,17]. The hearing impairment also affects psychosocial and emotional well being. They feel upset, isolated and frustrated [18]. People with hearing impairment also face significant difficulties in the presence of ambient noise like in restaurants, and in parties [18]. They also experience physical exhaustion on attempts to listen in challenging situations [19]. Not much-published literature is available on hearing handicap in elderly patients with hearing loss in rural population in India. Understanding the changes in social and emotional health of the individuals can help us focus on these aspects of health as well, thereby providing a holistic care for the patient.
Materials and Methods
A cross-sectional study was conducted in Shri Sathya Sai Medical College and Research Institute, Tamil Nadu, India, for a period of two months (June, July 2017). The sample size was calculated from a previous study where the prevalence of hearing handicap in elderly people with hearing loss was 92 % [16]. The precision error was taken as 6% (6 X 92/100) which was 5.5. The sample size was calculated using the formula 4 pq/r2; 4 X 92X 8/(5.5)2=97. So, the sample size was taken as 100.
Subjects
People ≥60 years of age, both sexes and with bilateral symmetrical sensorineural hearing loss were included in the study. People with pre-existing ear disease like Chronic Suppurative Otitis Media, Conductive/mixed hearing loss and patients with cognitive impairment who cannot appropriately respond to questionnaire were excluded from the study. Patients using hearing aid were also not included in the study as the hearing status will improve with the use of hearing aid and the impact cannot be clearly assessed [19].
Data Collection
The study was conducted after clearance from Institutional Ethical Committee in May 2017 prior to collection of data (IEC NO: 2017/375). Patients ≥60 years of age attending the OPD of various departments were explained about the procedure and the purpose of the study. Patients who were willing to participate in the study were included after obtaining an informed written consent.
Patients ≥60 years of age with hearing loss were initially examined-to rule out any underlying external or middle ear conditions like Secretory Otitis Media/Chronic Suppurative Otitis Media. Hearing was initially assessed using tuning fork test. A 512 HZ tuning fork was used to assess hearing. Rinne’s, Weber’s and Absolute Bone Conduction tests were done. Rinne’s test was positive, Weber’s test was centralised and absolute bone conduction was reduced in patients with bilateral symmetrical sensorineural hearing loss [20]. Hearing status was confirmed by doing a pure tone audiometry.
Audiogram was performed using pure tone audiometer-Arphi Model 500 MK III. Audiogram was plotted from the values obtained. Pure tone average was calculated for both ears for 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz. Based on the audiogram, the type of hearing loss was identified. WHO classification was used to calculate the degree of hearing loss [21].
HHIE is a self-assessment questionnaire devised by Weinstein and Ventry. This questionnaire is freely available and was used for the study. The questionnaire has 25 questions with 12 on social or situational aspects and 13 on emotional aspects. Each question has three responses; yes, sometimes and no with 4, 2, 0 point scoring respectively. The total scores were calculated for 100 which include both social and emotional aspects. The maximum social scores was 48 and the emotional scores was 52. The total score of 0 is no handicap and 100 indicating total handicap. A total score of 0-16 was considered as no handicap, 18-42 as considered as mild to moderate handicap and more than 44 was considered as severe handicap. The questionnaire was translated in the regional language (Tamil) and its correct translation was confirmed. The translated Tamil version was retranslated back into English by a third person who was not a part of the study. The retranslated version was in concordance with the original questionnaire. The questions were read and marked by the patients. If the participants were illiterate the questions were read and the responses were marked. After filling the questionnaire the total, social and the emotional scores were calculated.
Statistical Analysis
The collected data were compiled and statistically analysed using Statistical Package for Social Sciences (SPSS) software-version 23.0. The mean and standard deviation was calculated for the total, social and emotional scores. The correlation between the age, sex, employment, literacy, marital status and degree of hearing loss with the severity of handicap scores was statistically studied using chi-square test.
Results
The study sample had 100 patients who visited the present hospital. All the participants were ≥60 years of age. The mean age of presentation was 66.05 years. The age distribution ranged from 60-93 years. The sex distribution was 53% males, 47% females.
The handicap score was calculated from the questionnaire. The mean and the standard deviation for the total scores were 52.72±38.30. The mean and the standard deviation of the social and the emotional sub-scores were 25.94±17.80 and 26.86±20.84 respectively.
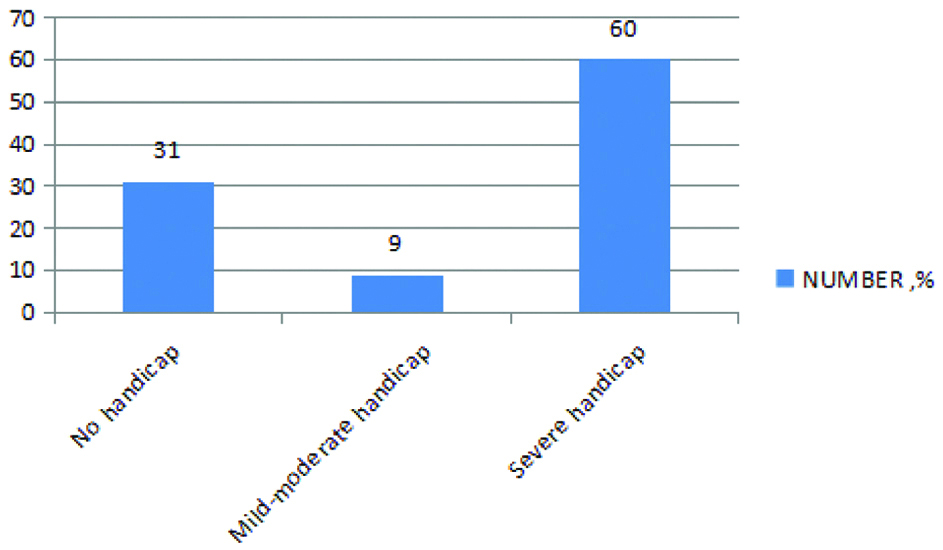
In the study population, 31 (31%) did not perceive any handicap. A total of 69 (69%) of the study population showed some handicap [Table/Fig-1].
Distribution of handicap levels in the study population (N=100).
The degree of hearing loss was correlated with the severity of handicap. Most patients had ‘mild’ (40%) to ‘moderate’ (44%) hearing loss. Most people with mild hearing loss (n=30, 75%) did not perceive any handicap. Most people with moderate hearing loss (n=37, 84.1%) perceived severe handicap. A 14% of the people had severe hearing loss and only 2% had profound hearing loss. All the patients with severe and profound hearing loss perceived severe handicap [Table/Fig-2]. There was statistically significant correlation between degree of hearing loss and the severity of hearing handicap. (p=0.0001). There was no statistically significant relationship between the age, sex, employment status and the severity of handicap scores [Table/Fig-3].
Distribution of study population based on degree of hearing loss and handicap scores.
| Degree of Hearing Loss | N | No Handicap | Mild to Moderate Handicap | Severe Handicap | |
|---|
| Mild | 40 | 30 (75%) | 3 (7.5%) | 7 (17.5%) | χ2=67.771df=6p=0.0001 |
| Moderate | 44 | 1 (2.3%) | 6 (13.6%) | 37 (84.1%) |
| Severe | 14 | 0 | 0 | 14 (100%) |
| Profound | 2 | 0 | 0 | 2 (100%) |
Chi-square test
Distribution of study population based on the demographic details.
| No Handicap | Mild to Moderate Handicap | Severe Handicap | p-value |
|---|
| Age |
| 60-70 years | 27 (33.7%) | 7 (8.8%) | 46 (57.5%) | χ2=2.596df=4p=0.624 |
| 71-80 years | 3 (20%) | 1 (6.7%) | 11 (73.3%) |
| 80 and above | 1 (20%) | 1 (20%) | 3 (60%) |
| Sex |
| Female | 18 (33.96%) | 5 (9.4%) | 30 (56.6%) | χ2=0.610df=4p=0.788 |
| Male | 13 (27.7%) | 4 (8.5%) | 30 (63.8%) |
| Employment |
| Employed (N=25) | 8 (32%) | 0 | 17 (68%) | χ2=3.301df=2p=0.198 |
| Dependent (N=75) | 23 (30.7%) | 9 (12%) | 43 (57.3%) |
| Education Status |
| Literate, N=43 | 20 (46.5%) | 5 (11.6%) | 18 (41.9%) | χ2=10.534df=2p=0.001 |
| Illiterate, N=57 | 11 (19.3%) | 4 (7%) | 42 (73.7%) |
| Marital Status |
| Living with spouse, N=45 | 2 (48.9%) | 6 (13.3%) | 17 (37.8%) | χ2=64.809df=9p=0.0001 |
| Living alone (single/widowed), N=55 | 9 (16.4%) | 3 (5.5%) | 43 (78.1%) |
Chi-square test
People who could read and write in any language were taken as literates. People who could not read or write were considered as illiterate. As the study was done in a rural population most patients were illiterate (n=57, 57%). There was statistically significant association between the education status and the severity of handicap scores (p=0.001). People who were living alone had a higher level of auditory handicap than people who were living with spouse (p=0.0001).
Discussion
This study was conducted among 100 subjects who were 60 years and above with hearing loss. The mean age of presentation was 66.02 years. The study group had 53% females and 47% males. Based on the scores obtained from the questionnaire the handicap scores were calculated. The mean total score, emotional and social sub-scores were 52.7, 26.86 and 25.94 respectively. The hearing loss in these individuals causes communication difficulties which interfere with day to day activities. These people have less social activities, poor social relations and emotional disturbances as indicated by high social, emotional and total scores. Similar high scores were documented in study by Shrestha KK et al., and Iwasaki S et al., [16,24]. However, lower scores were documented in study by Moser S et al., [25].
Among people with hearing loss of varying degree, about 31% of people did not perceive any handicap. This could be because of mild hearing loss in most of the patients. This is in accordance with findings by de Araújo PG et al., and Moser S et al., [18,25]. Chang HP et al., in their study documented higher percentage (78.6%) of people with hearing loss without any perceived handicap [23]. This could be because this was a study on the community dwellers where most people could have been asymptomatic due to minimal or mild hearing loss. However, in study by Shrestha KK et al., only 7.1% had no handicap [16]. This could be because the study was done on population visiting ENT department and most people come for consultation only when they perceive their problem.
As the severity of hearing loss increases, the perceived handicap also increases. All patients with severe and profound hearing loss had severe handicap. There was high statistical significance for the same. The higher the hearing loss, the more it impairs their social and emotional life. Similar results were reported by Shrestha et al., Chang HP et al., Iwasaki S et al., Moser S et al., Tatović M et al., [16,23-26]. This is further supported in study by Manchaiah V [27], where self-predicted handicap scores were significant predictors of participation restriction and health-related quality of life.
With increasing age, the degree of hearing loss increases. As seen in [Table/Fig-3], with increasing age the proportion of people with severe handicap was also increasing up to 80 years of age. There was no statistical significance between age and severity of handicap. This could be because of the number of people were less with increasing age (5% in more than 80 years of age). As it was a hospital-based study, people >80 years of age who visited the hospital were less, probably due to physical limitations. This finding finds support from study by Moser S et al., [25]. However, in study done by Chang HP et al., there was increasing handicap with increasing age [23]. This could be because more population was screened at the community level and were good number of patients in all the age groups.
There was no gender difference in determining handicap levels in elderly people. This finding is consistent with findings of study by Shrestha KK et al., Chang HP et al., Moser S et al., [16,23,25]. Other studies by Iwasaki S et al., showed more hearing loss in males [24]. This could probably be because men are exposed more to industrial and environmental noise. However, in study by de Araújo PG females had greater handicap than males [18]. This could be because females have more emotional liability than males impairing their emotional health.
The employment status of the people did not show any association with handicap scores. This could be because people included in the study were ≥60 years of age and most of them were dependent on the family members. The type of work was not taken into consideration. As the study was done in a rural population, the nature of work might not require significant social interaction.
There was significant association between education status and handicap severity. The handicap scores were more among illiterate patients. The understanding of the hearing loss and the measures to prevent and avoid damage due to noise could have been better in an educated patient. The social and emotional adjustments are also probably better in a literate. Similar findings were reported in study by Dalton DS et al., [17].
The perceived hearing handicap by people with hearing loss was more in people living alone than among those living with spouse. This could be because people alone have to meet their daily needs on their own. They would require more communication with others in comparison with people living with spouse. This finding is akin to findings in study by Chang HP et al., [23].
Identifying factors associated with hearing handicap like illiteracy and people who live alone can help us in identifying people in need for further audiological workup. These people can be motivated for rehabilitation which might help them to decrease the handicap.
Limitation
The hearing handicap assessed in the study is only a self-perceived handicap score based on the response given for the standard questionnaire. The handicap scores obtained are subjective. There is no objective way of assessing hearing handicap. There might be some under-reporting as the hearing loss in elderly people is of insidious onset and the person might take some significant time before realising the hearing loss. Likewise, there is a possibility of over-reporting of the auditory handicap in elderly people especially if they are living alone or dependant on their family members. Moreover, the aftermath of hearing loss on the psychological and the functional facets was not assessed in the study.
Conclusion
From the findings of the present study, it can be concluded that hearing impairment in elderly is associated with hearing handicap. The severity of hearing loss correlates with the severity of hearing handicap. There is no significant association between age, sex and employment status of the individual with the severity of handicap. There is significant association between the education status and whether they are living alone with the handicap scores.
The study prompts few recommendations; Early identification of hearing loss by the first contact physicians and referral to higher centre for further evaluation, creating awareness among the people about the availability of hearing assistive devices and for the policymakers to allocate appropriate financial resources for rehabilitation of the people with hearing handicap.
Chi-square test
Chi-square test