Primary Lymphoma of the Soft Tissue: A Pathologist’s Perspective
Madhusmita Jena1
1 Professor, Department of Pathology, East Point College of Medical Science, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Madhusmita Jena, 11C4, Krishna Nagar Apt, Annasandrapalya, HAL Post, Bangalore-560017, Karnataka, India.
E-mail: jena_madhusmita@hotmail.com
Primary lymphoma of the soft tissue is rare accounting for 0.1% of the cases. A case of Non Hodgkin lymphoma of the soft tissue presented as multiple swellings in the upper extremity diagnosed clinically & radiologically as neurofibroma. A Fine Needle Aspiration Cytology (FNAC) performed on the swellings showed cytologic features of a lymphoproliferative lesion which was confirmed subsequently on histopathology and immuno-histochemistry. This case is reported to highlight and recognize this entity at a rare anatomic site and to bring out an awareness among cytopathologists and radiologists of this rare lesion which may avoid errors in diagnosis.
Cytodiagnosis, Extremity, Neurofibroma, Non Hodgkins lymphoma
Case Report
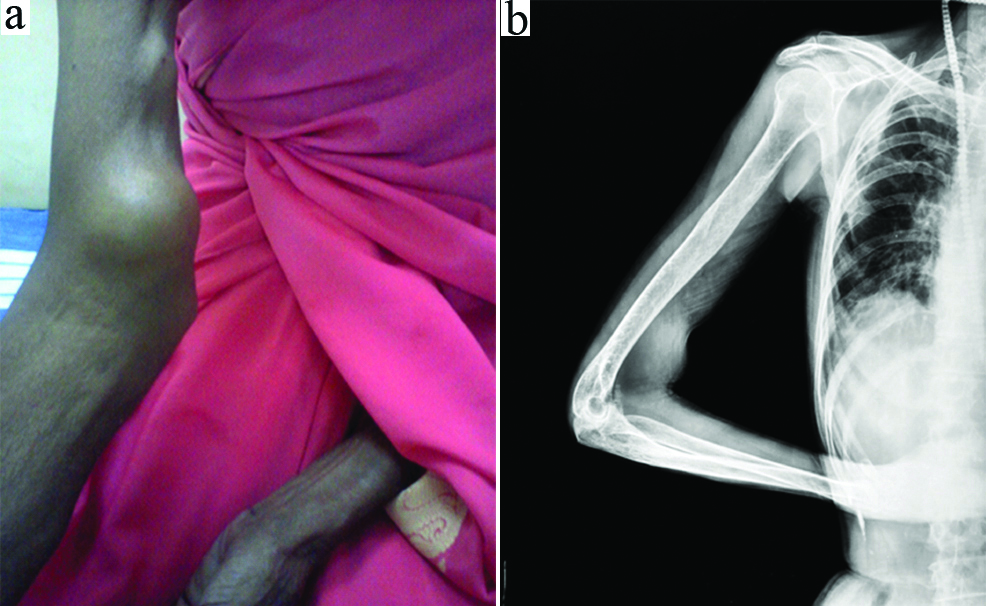
A 60-year-old lady presented with multiple subcutaneous swellings in the right arm since one month [Table/Fig-1a]. These swellings were insidious in onset and had progressed to the size of 4 cm. She also complained of pain and weakness in the right hand and fingers. There was no other significant positive history. The patient was seronegative for HIV (Human Immune Deficiency Virus). She was well preserved with normal general physical examination. Local examination revealed three subcutaneous swellings on right arm close to the median nerve with the largest one measuring 4×6 cm. A provisional diagnosis of neurofibroma was suggested. An X-Ray performed on the forearm showed a soft tissue mass not involving the bone [Table/Fig-1b]. Ultrasonogram of the abdomen was normal. There were no enlargement of draining axillary lymph nodes. FNAC was performed on the forearm swelling and followed by an excision biopsy for histopathologic confirmation. Aspirated smears were stained with Haematoxylin and Eosin stain, Giemsa stains. Special stains like Periodic Acid-Schiff Stain (PAS) was also done.
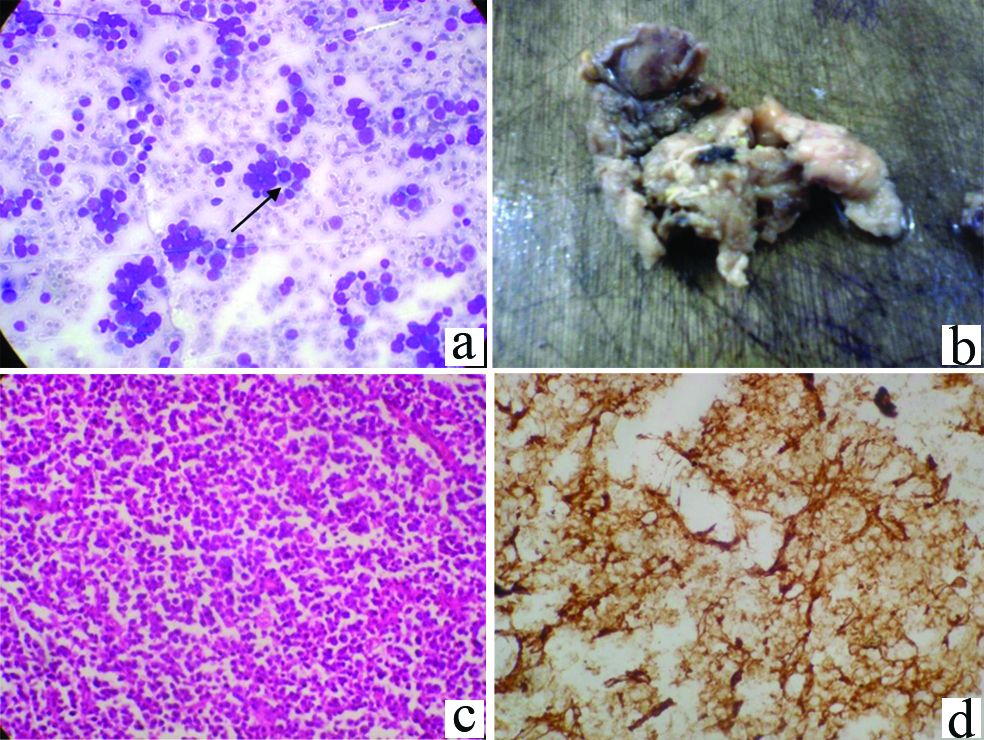
FNAC findings: Aspirated smears showed a high cellularity composed of a mixed population of round small cells and large cells which looked like lymphoid cells. These cells showed moderately enlarged nuclei with nucleoli, few atypical mitoses and moderate amount of cytoplasm [Table/Fig-2a]. No nuclear convolutions or multinucleation of the cells were noted. Also, the cells showed focal clustering giving a rosette like appearance. A PAS stain done on the smears showed a weak cytoplasmic positivity in some of the atypical cells. A diagnosis of round cell tumour of the soft tissue favouring towards a lymphoproliferative lesion was suggested.
a) Showing two soft tissue masses in the right upper extremity. b) X-ray showing the mass is in the soft tissue without any bone involvement.
a) Smears showing cells with high *N:C ratio, nucleoli, mitosis, focal clustering of cells with rosette like appearance with an atypical mitosis shown by an arrow (Giemsa stain 40X). b) Showing multiple irregular soft tissue pieces with the larger one measuring 8×3×2.5 cm. c) Diffuse infiltrate of monotonous population of lymphoid cells with a moderately enlarged nucleus showing prominent nucleoli and occasional mitosis (H&E 10X). d) Membrane positivity for CD20 marker on IHC (10X).
N:C= Neucleocytoplasmic Ratio
Histopathology
The soft tissue mass was excised and sent for histopathology. The specimen received was multiple irregular soft tissue mass with the largest tissue bit measuring 8×3×2.5 cm [Table/Fig-2b]. Microscopic examination showed lesional tissue with a diffuse infiltrate of monotonous population of lymphoid cells with a moderately enlarged nucleus showing prominent nucleoli and occasional mitosis [Table/Fig-2c]. The lymphoid cells were seen infiltrating into adjacent fat, muscle tissue with a focus of perineural involvement.
On Immunohistochemistry (IHC), the tumour cells were diffusely positive for LCA (Leucocyte Common Antigen) and CD20 and negative for cytokeratin [Table/Fig-2d].
The patient was referred to regional cancer centre for further treatment with chemotherapy.
Discussion
Primary Non Hodgkins lymphoma localised in the soft tissue is uncommon accounting for 0.1% of the cases [1,2]. They manifest as soft tissue masses with a higher incidence in lower extremity followed by upper extemity and Gluteal region [3-5,7]. The occurence is more common with B cell type Non Hogkins lymphoma especially DLBCL (Diffuse large B cell Lymphoma) type than Hodgkin’s lymphoma [2,5]. The soft tissue lymphomas mainly affect the patients in their sixth to seventh decade which was seen in this case [6]. As per literature the B cell type Non Hodgkins Lymphoma are indolent except the DLBCL type and the lymphomas associated with HIV which have an aggressive course [1,4].
Although the diagnosis of lymphoma should be based on the histological examination, there are cases in which the biopsy specimens are difficult to acquire and therefore FNAC becomes an acceptable alternative diagnostic procedure with excellent accuracy [3]. The other round cell malignant tumours of the soft tissue such as Extraskeletal Ewing’s/PNET (Primitive Neuroectodermal Tumour), rhabdomyosarcoma, liposarcoma, synoviosarcoma and metastatic carcinoma may mimic the lymphoma on cytomorphology [8,9].
Smears from Atypical Ewing’s Sarcoma show small, medium, large cells with occasional prominent nucleoli, more cellular cohesion, moulding and clustering. A weak positivity on PAS stain did not help in favouring a diagnosis towards Ewing’s sarcoma. Similarly, PNET is characterised by round to more elongated tumour cells with deeply stained nuclei with more cell cohesion, clustering and pseudorosette of Wright-Homer type [8].
Rhabdomyosarcoma smears show clusters and dispersed pleomorhic tumour cells with scanty to abundant cytoplasm and the nuclei have coarse chromatin with more prominent nucleoli [8]. In the present case the cells were not pleormorphic. Also, the background showed mature lymphocytes.
Synovial sarcoma show high cellularity composed of a mixture branching tissue fragments and dispersed cells. The cells are small to medium sized spindly, round or oval. The nuclei are ovoid, rounded or fusiform with bland chromatin and inconspicuous nucleoli. Acinar structures are seen in biphasic synovial sarcoma [9].
A metastatic carcinoma was howevever ruled out based on clinical history, imaging studies and absence of epithelial cells.
So after excluding all the differentials based on the cytomorphology, the diagnosis was narrowed to Non-hodgkin lymphoma of the soft tissue which could be either a B cell or T cell type. Cytologically a peripheral T cell lymphoma shows atypical lymphoid cells with convoluted nuclei, anisonucleosis and sometimes multinucleation which was not evident in the case [10]. Hence in the present case on cytology, a T cell lymphoma was less favoured over a B cell lymphoma which is more common in the soft tissue [2,5]. Keeping this in mind, an IHC panel of LCA, CD20, cytokeratin were considered which would help in typing the lymphoma on histopathology. A negative cytokeratin ruled out an epithelial neoplasm. LCA and CD 20 positivity confirmed a B cell type NHL of the soft tissue. Based on the FNAC, histopathology, IHC findings a final diagnosis of NHL of B cell type was made.
As per the literature the Lymphomas of the soft tissue like other extra nodal lymphoma should not be excised and they should be treated by chemotherapy and radiotherapy [11].
In this case an excision was done to confirm the cytological diagnosis. After the surgical excision the patient was given chemotherapy with a regular follow-up.
Conclusion
The occurence of primary Non Hodgkin lymphoma in the soft tissue is very rare and can be mimicked by many other lesions on cytology which can be confirmed on histology with immunohistochemistry and thereby guide the clinicians towards a proper management.
[1]. Corti M, Villafane MF, Bistmans A, Campitelli A, Soft tissue masses as presentation of non Hodgkin’s Lymphoma in AIDS patientsAn Bras Dermatol 2013 88:631-34.10.1590/abd1806-4841.2013213824068141 [Google Scholar] [CrossRef] [PubMed]
[2]. Derenzini E, Casadei B, Pelligrini C, Argnani L, Pileri S, Zinzani PL, Non-Hodgkin lymphoma presenting as soft tissue masses: a single center experience and meta analysis of the published seriesClinical Lymphoma, Myeloma and Leukaemia 2012 13:258-65.10.1016/j.clml.2012.10.00323246162 [Google Scholar] [CrossRef] [PubMed]
[3]. Gao YH, Xu Q, Wei G, Liu HS, Primary Giant lymphoma of the right thigh: A case report and brief review of the literatureOncol Lett 2012 4:1023-26.10.3892/ol.2012.84823162644 [Google Scholar] [CrossRef] [PubMed]
[4]. Salomao DR, Nascimento A G, Liyod RV, Chen MG, Haberman TM, Strickler J, lymphoma in Soft tissue: A clinicopathological study on 19 casesHuman Pathol 1996 27:253-57.10.1016/S0046-8177(96)90065-9 [Google Scholar] [CrossRef]
[5]. Rosai D, Ackerman M, Soft tissuesIn: Rosai and Ackermans Surgical Pathology 2004 9th edElsevier:2314-4. [Google Scholar]
[6]. Bracke P, Vanhoenacker F, De Schepper AM, Soft tissue lymphomaIn: Arthur M De Schepper’s Imaging of Soft tissue Tumour 2001 2nd edNew YorkSpringer:427-32.10.1007/978-3-662-07856-3_23 [Google Scholar] [CrossRef]
[7]. Bela abidia B, Sellami S, Hamdaoui Essadki B, Primary malignant non Hodgkin skeletal muscle lymphoma: a case reportRev Chir Orthop Reparatrice Appar Mot 2002 88:518-21.French [Google Scholar]
[8]. Khan AR, FNAC of Ewing Sarcoma family of tumour, skeletal and extraskeletal. A study of 21 casesJk-Practitioner 2003 10:309-13. [Google Scholar]
[9]. Ackerman M, Domanski HA, The complex cytological features of synovial sarcoma in fine needle aspirates, an analysis of four illustrious casesCytopathology 2007 18:234-40.10.1111/j.1365-2303.2007.00458.x17559565 [Google Scholar] [CrossRef] [PubMed]
[10]. Van Heerde P, Miliauskas J, Lymph nodesIn: Svante R Orell’s fine needle aspiration cytology 2005 4th edElsevier:100-14. [Google Scholar]
[11]. Knowles B, Sepell JW, Extra-nodal Lymphoma presenting as a mimic of soft tissue sarcomaANZ J Surg 2003 73:26-30.10.1046/j.1445-2197.2003.02613.x12534734 [Google Scholar] [CrossRef] [PubMed]