Foreign Body in Rectum: Case Management and Review of Literature
Mahim Koshariya1, Abhishek Shitole2, Anshul Siroliya3, Mayank Soni4, Sheikh Behram5
1 Professor, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
2 Resident, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
3 Senior Resident, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
4 Resident, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
5 Resident, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mahim Koshariya, Professor, Department of General Surgery, Gandhi Medical College and Hamidia Hospital, Bhopal-462001, Madhya Pradesh, India.
E-mail: mahimk2000@yahoo.co.uk
General surgeons not so often encounter rectal foreign body; but its incidence is now increasing. Males are the common victim in both child and adult age group. Management can be challenging for the treating surgeon. Diagnosis can be made on clinical grounds and confirmed by radiological investigations. Various approaches have been described in literature but owing its wide spectrum of presentation and heterogeneity of foreign bodies, no single procedure can be considered as the gold standard. We hereby present a case of rectal foreign body in a young male with a history of assault.
Extraction, Impacted foreign body, Rectum
Case Report
A 30-year-old male presented to the Emergency department complaining of pain in abdomen and bleeding per rectum with alleged history of forced insertion of foreign body in his rectum. On examination patient’s vitals were stable, on palpation abdomen was soft with mild tenderness. On per rectal examination, foreign body was palpable.
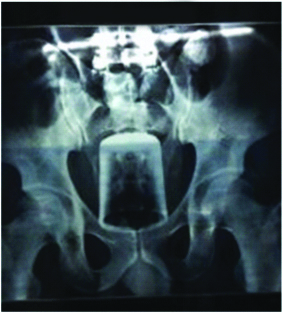
X-ray of abdomen revealed radio-opaque shadow in pelvic region of beverage glass [Table/Fig-1]. USG abdomen showed linear hyper-echogenic structure of size 11×5 cm (approximately) in the rectum with dilatation of rectal lumen.
X-ray pelvis showing foreign body.
After informed consent, patient was taken to the operating room for retrieval of the foreign body under general anaesthesia. Initially manual extraction was attempted per rectally in lithotomy position. Since the foreign body was impacted snugly, it could not be extracted. Then attempts were made by gliding the foley’s catheter past the foreign body and pulling it towards the anal canal after inflating the balloon, but it resulted in failure. Then patient was taken to supine position for exploratory laparotomy. Transanal extraction was attempted by applying mechanical pressure over sigmoid colon and rectum but failed [Table/Fig-2]. Then a sigmoid enterostomy was made and foreign body (beverage glass) was retrieved along with fecolith [Table/Fig-3]. Enterostomy defect was closed in two layers (inner layer by vicryl and outer layer by silk). Right pelvic drain was kept and abdomen was closed. On 3rd postoperative day patient’s drain was removed and oral sips were allowed. Patient was discharge on 7th postoperative day.
Foreign body (tumbler) after pushed up in sigmoid colon before sigmoid enterostomy.

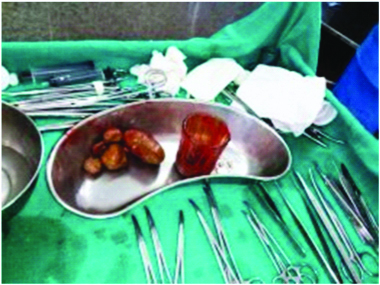
Extracted foreign body (glass tumbler) along with fecoliths.
Discussion
Rectal foreign bodies though they are infrequent, are no longer considered as clinical queerness in and it appears that their incidence is increasing specifically in urban population [1,2].
Various types of objects have been reported in the literature (ranging from fruit and vegetable, cosmetic containers, cans and bottles, batteries, light bulb or sex toys) and in some instances cause is not ascertained (Munchausen syndrome by proxy) [3,4].
Detail clinical history and physical examination are essential for the diagnosis and management. Patient may present asymptomatically to florid peritonitis which depends upon the type of rectal foreign bodies, method of insertion, duration and presence of non-professional intervention to remove these bodies. Most common presentation is complaining of anal/abdominal pain and bleeding per anal in 66.7% of cases [5]. Careful abdominal examination should perform to elicit signs of peritonitis and to palpate object per abdomen.
In the present case major symptom was pain in abdomen which was also the chief complain in other cases reported by Nayaka T et al., Cheereth RG et al., [6,7]. Bleeding per rectum was also reported by Nayaka T et al., which was also present in the case [6]. Rectal foreign body are mostly palpable per rectally as was with the present case and other cases reported by Cheereth RG et al., Kasotakis G et al., [7,8].
Eftaiha M et al., classified foreign bodies in rectum as high lying or low lying depending on its relation with rectosigmoid junction [9]. Kingsley A et al., reported that foreign bodies in low or mid rectum upto 10 cm level is often removed trans anally while those above 10 cm may require laparotomy for retrieval [10]. Plain X-ray abdomen and pelvis erect view is mandatory to determine the presence, number, shape, size location direction of foreign bodies and associated complication like perforation and obstruction. If X-ray cannot reveal the foreign body than newer technique like CT with 3D reconstruction can also provide the information regarding nature and orientation of foreign body can be used.
An attempt at manual retrieval of the foreign body is always narrated as first step. Transanal extraction of foreign body should be done under direct vision and after adequate relaxation of anal sphincter by general or spinal anaesthesia. Foreign body may be grasped and extracted manually following recto-sigmoid axis. Lithotomy is the most feasible position. Gliding a Foley’s catheter past the foreign body and inflating the balloon above may help to pull the rectal foreign body towards anal canal [11,12]. Endoscopy is also being used where foreign body is located high in the rectum or even colon. Other techniques include vacuum extractor device, using plaster of paris and obstetric forceps. Single incision laproscopic surgery can also be used to extract rectal foreign body. Laparotomy is the last option if all the other methods failed [12].
Conclusion
Rectal foreign bodies pose a great challenge for the treating doctors as they usually present late, with wide spectrum of presentation, diverse complications and with heterogeneity of objects. Because of this wide ranging spectrum no single procedure is described for retrieval.
[1]. Goldberg JE, Steele SR, Rectal foreign bodiesSurg Clin North Am 2010 90(1):173-84.10.1016/j.suc.2009.10.00420109641 [Google Scholar] [CrossRef] [PubMed]
[2]. Lake JP, Essani R, Petrone P, Kaiser AM, Asensio J, Beart RW, Management of retained colorectal foreign bodies: predictors of operative interventionDis Colon Rectum 2004 47(10):1694-98.[PubMed]10.1007/s10350-004-0676-415540301 [Google Scholar] [CrossRef] [PubMed]
[3]. Khan SA, Davey CA, Khan SA, Trigwell PJ, Chintapatla S, Munchausen’s syndrome presenting as rectal foreign body insertion: a case reportCases J 2008 1(1):243[PMC free article] [PubMed]10.1186/1757-1626-1-24318925957 [Google Scholar] [CrossRef] [PubMed]
[4]. Khan MK, Ahmad M, Hanif SA, Haq AS, Torture by introducing foreign object in rectum: a case reportIndian Journal of Forensic Medicine and Pathology 2013 6(2):105-08. [Google Scholar]
[5]. Busch DB, Starling JR, Rectal foreign bodies: case reports and a comprehensive review of the world’s literatureSurgery 1986 100(3):512-19. [Google Scholar]
[6]. Nayaka T, Gupta R, A case of an unusual foreign body of rectum: presentation and managementIOSR Journal of Dental and Medical Sciences 2013 3(4):14-16.10.9790/0853-0341416 [Google Scholar] [CrossRef]
[7]. Cheereth RG, Ninan AG, Rectal foreign body: a case reportInt Surg J 2017 4(3):1119-22.10.18203/2349-2902.isj20170874 [Google Scholar] [CrossRef]
[8]. Kasotakis G, Roediger L, Mittal S, Rectal foreign bodies: A case report and review of the literatureInternational Journal of Surgery Case Reports 2012 3(3):111-15.10.1016/j.ijscr.2011.11.00722288061 [Google Scholar] [CrossRef] [PubMed]
[9]. Eftaiha M, Hambrick E, Abcarian H, Principles of management of colorectal foreign bodiesArch Surg 1977 112(6):691-95.10.1001/archsurg.1977.01370060023003871246 [Google Scholar] [CrossRef] [PubMed]
[10]. Kingsley A, Abcarian H, Colorectal foreign bodies’ management updateDis Colon Rectum 1985 28(12):941-44.10.1007/BF025543124064854 [Google Scholar] [CrossRef] [PubMed]
[11]. Manimaran N, Shorafa M, Eccersley J, Blow as well as pull: an innovative technique for dealing with a rectal foreign bodyColorectal Dis 2009 11(3):325-26.10.1111/j.1463-1318.2008.01653.x18662236 [Google Scholar] [CrossRef] [PubMed]
[12]. Safioleas M, Stamatakos M, Safioleas C, Chatziconstantinou C, Papachristodoulou A, The management of patients with retained foreign bodies in the rectum: from surgeon with respectActa Chir Belg 2009 109(3):352-55.10.1080/00015458.2009.1168043819943592 [Google Scholar] [CrossRef] [PubMed]