Osseous Metaplasia in Adenocarcinoma
Phiza Aggarwal1, RPS Punia2, Robin Kaushik3, Manveen Kaur4, Deepak Aggarwal5
1 Assistant Professor, Department of Pathology, Government Medical College and Hospital, Chandigarh, India.
2 Professor, Department of Pathology, Government Medical College and Hospital, Chandigarh, India.
3 Professor, Department of General Surgery, Government Medical College and Hospital, Chandigarh, India.
4 Senior Resident, Department of Pathology, Government Medical College and Hospital, Chandigarh, India.
5 Associate Professor, Department of Pulmonary Medicine, Government Medical College and Hospital, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Phiza Aggarwal, Assistant Professor, Department of Pathology, Level-3, Block-E, Government College and Hospital, Sector-32, Chandigarh, UT, India.
E-mail: drphiza@hotmail.com
Osseous Metaplasia (OM) or heterotopic ossification is a rare phenomenon with unknown aetiology that is characterised by the formation of mature bone elements in the stroma of different tumors. Awareness of this condition is important to avoid diagnostic confusion with carcinosarcoma and local bone invasions that have different lines of treatment and prognosis. Here, authors report two cases of heterotopic ossification in adenocarcinoma of sigmoid colon and lung and provide salient features that could help to detect the condition.
Heterotopic ossification, Malignancy, Tumor
Case Report
Case 1
A 48-year-old male presented with acute onset abdominal distension, pain and obstipation for five days. X-ray abdomen showed multiple air-fluid levels suggestive of intestinal obstruction. A provisional diagnosis of acute intestinal obstruction secondary to an underlying Tumor was made. Routine investigations were normal except for serum Carcinoembryonic Antigen (CEA) levels, that were mildly raised (3.19 ng/mL). The patient underwent emergency exploratory laparotomy in which a large fungating mass was seen completely obstructing sigmoid colon along with paracolic lymphadenopathy. The patient underwent left-sided hemicolectomy with an end colostomy.
On gross examination, resected specimen, 30.5×4.0 cm in size, showed an ulceroproliferative firm to hard growth measuring 6.0×5.0×4.0 cm [Table/Fig-1]. Microscopic examination showed a Tumor in the sigmoid colon arranged in a complex glandular and focal cribriform pattern, exhibiting moderate nuclear anaplasia. The background showed abundant extracellular mucin. Laminated bony trabeculae of varying thickness rimmed by cuboidal to polygonal uninucleate bland looking osteoblasts were diffusely seen in the stroma in close proximity to the Tumor [Table/Fig-2]. The bony trabeculae, however, did not enclose any marrow elements. Focal areas of calcification were also evident in the necrotic areas of the Tumor suggestive of dystrophic calcification. Histopathological diagnosis of moderately differentiated adenocarcinoma, mucin-secreting type with OM was made. Eleven lymph nodes resected from the specimen were free of Tumor and did not show any evidence of ossification.
(Case 1): The resected specimen showing Tumor (black arrow) in sigmoid colon.

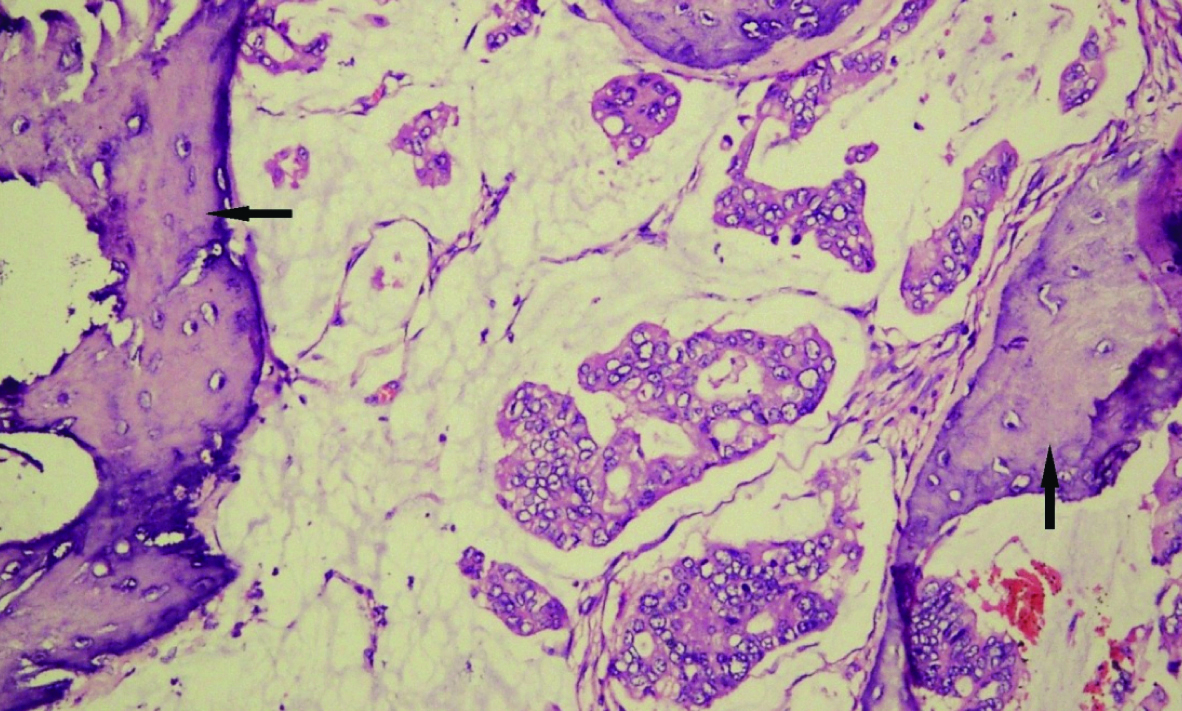
(Case 1): Section shows glandular Tumor with osseous metaplasia (black arrow) in a mucinous background (H&E, x400).
Case 2
A 42-year-old male presented with cough, chest pain and dyspnea for 2-3 months and haemoptysis for the last two weeks. X-ray chest PA view presented an ill-defined opacity in the right hilar and parahilar region along with cardiomegaly [Table/Fig-3]. Contrast Enhanced Computed Tomography (CECT) thorax showed a small mass in the right bronchus intermedius along with sub-segmental collapse of the superior segment of right lower lobe [Table/Fig-4]. Considering a middle-aged and non-smoker, a provisional diagnosis of subacute infection, like tuberculosis, was made. Patient underwent flexible bronchoscopy which showed an endo-bronchial growth in the right bronchus intermedius. Endo-bronchial biopsy showed a Tumor arising from the overlying dysplastic bronchial mucosa and comprising of malignant cells arranged in sheets and focal glandular pattern. Interspersed within the Tumor was seen an irregularly deposited osteoid lined by bland osteoblasts [Table/Fig-5]. The bony trabeculae were lying in close proximity to the Tumor without any evidence of Tumor invasion. The histopathological diagnosis of adenocarcinoma lung with heterotopic ossification was made. The patient underwent systemic chemotherapy which resulted in a partial decrease in the size of the Tumor.
(Case 2): X-ray chest PA view showing an ill-defined opacity in the right hilar and parahilar region.

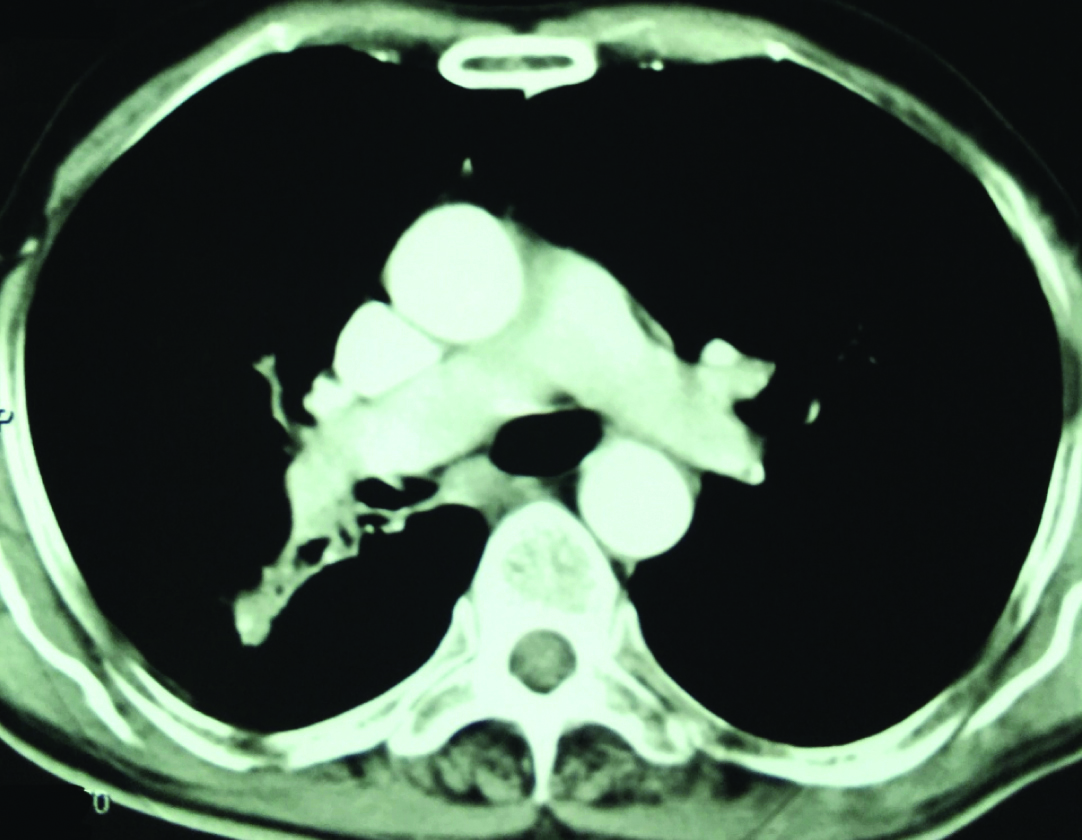
(Case 2): Contrast Enhanced Computed Tomography (CECT) thorax showing a small mass in the right bronchus intermedius along with sub-segmental collapse of superior segment of right lower lobe.
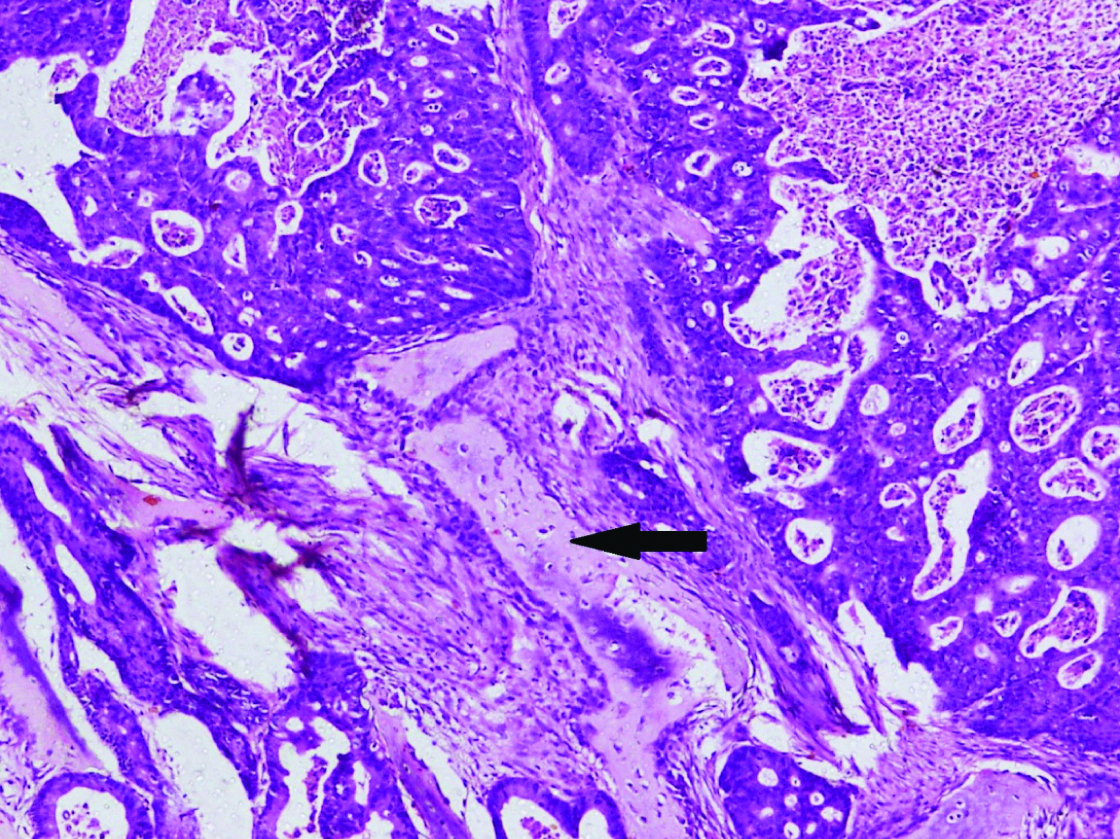
(Case 2): Section shows metaplastic bone (black arrow) in adenocarcinoma lung. (H&E, x400).
Discussion
Osseous Metaplasia (OM), also known as heterotopic bone formation, is an incidental histopathological entity that is usually found in association with different malignant and benign neoplasms. It is an uncommon phenomenon with an estimated overall incidence of 0.4% in malignant Tumors [1]. It has been reported to occur in Tumors, particularly adenocarcinomas, of different organs including gastrointestinal tract, lungs, breast, thyroid and pancreas [2-4]. Besides malignancies, ossification has also been observed in benign colonic polyps, mucoceles of appendix and gastric carcinoid.
In the Gastro-intestinal tract, OM has been described in carcinomas of caecum, colon and rectum. Isolated colonic involvement seems to be rare as compared to rectum with very few cases reported in literature [5]. Among the lung carcinomas, heterotopic ossification has been predominantly seen in mucin-secreting adenocarinoma. In a retrospective analysis of 2269 surgically resected primary lung carcinomas, 33 cases of OM were found, out of which 24 (72%) had histopathological diagnosis of adenocarcinomas. Out of 33 patients, 15 had IntraTumoral Heterotopic Ossification (IHO), defined as ossification within the Tumor and 18 patients had extra-Tumoral OM (defined by ossification at a position at least 1 cm distant from the Tumor nest) [3]. The present case report also had lung adenocarcinoma with intra-Tumoral heterotopic ossification. However, the patient was quite young as compared to the previously reported cases in one study [6].
Till date, no clear aetiology has been elucidated for the histogenesis of this entity, however, different hypotheses have been proposed to explain the underlying mechanisms. Osseous metaplasia can develop secondary to ischaemia, necrosis, or inflammation in and around the Tumor. According to one hypothesis, Tumor cells synthesize certain biochemical messengers that stimulate uncommitted mesenchymal stromal cells into specific osteoblasts. This phenomenon of ‘Osteobast like transformation’ is considered a form of Epithelial-Mesenchymal Transition (EMT). Bone Morphogenic Protein (BMP), osteonectin, osteocalcin and osteopontin are the important factors that are upregulated in the Tumor cells causing metaplasia of the pleuripotent stromal cells [7]. Imai N et al., studied the immunohistochemical expression of BMP and observed that BMP-5 and BMP-6 were highly expressed in the cytoplasm of Tumor cells adjacent to ectopic bone tissue islands [8]. Another hypothesis suggests the role of mucin extravasated from the mucin-secreting adenocarcinomas that have a stimulatory effect on osteogenesis [9]. The colonic carcinoma in the present case report also showed large areas of extracellular mucin that could have contributed to bone formation.
In the differential diagnosis, the osteoid stromal response needs to be differentiated from true sarcomatous differentiation that is characterised by aggressive course and poor prognosis [10]. The carcinosarcomas are biphasic Tumors with both carcinomatous and sarcoma likes elements. The sarcoma counterpart may exhibit osteosarcomatous, chondrosarcomatous or liposarcomatous differentiation whereas heterotopic ossification presents with benign bone formation. In addition, whenever mature bone fragments are found in the malignant Tumors, bony invasion by the adjacent Tumor should be excluded by means of clinico-radiological correlation before labelling it as osseous metaplasia [11]. In the present case report, osseous metaplasia were diagnosed by histopathological evaluation supported by clinico-radiological correlation. The location of lesions away from normal bones excluded the bony invasion in both the cases. Immunohistochemical analysis for different markers might have helped in consolidating the diagnosis, but were not done due to financial issues.
There is no conclusive data on the prognostic implications of osteoid metaplasia in different Tumors [3]. Per se, OM is an indolent pathology that is unlikely to affect the overall prognosis of the disease due to its presence. Usually, presence of OM does not affect the management strategy, and the treatment involves the treatment of the underlying malignancy.
Conclusion
Osseous metaplasia is an indolent yet an important diagnostic entity. The present cases highlight the need to be aware of this uncommon histopathological finding to avoid diagnostic dilemma. Its incidental detection should be systematically evaluated to rule out other diagnostic mimics particularly carcinosarcoma and local bone invasion of the Tumor.
[1]. Dukes CE, Ossification in rectal cancer: (Section of Surgery: Sub-Section of Proctology)Proc R Soc Med 1939 32(11):1489-94.10.1177/003591573903201153 [Google Scholar] [CrossRef]
[2]. Byard RW, Thomas MJ, Osseous metaplasia within Tumors. A review of 11 casesAnn Pathol 1988 8(1):64-66. [Google Scholar]
[3]. Kuribayashi H, Tsuta K, Mizutani E, Maeshima AM, Yoshida Y, Gemma A, Clinicopathological analysis of primary lung carcinoma with heterotopic ossificationLung Cancer 2009 64(2):160-65.10.1016/j.lungcan.2008.08.00718819725 [Google Scholar] [CrossRef] [PubMed]
[4]. Shimazaki J, Takemura A, Nishida K, Kajiyama H, Shimoda M, Suzuki S, Heterotopic ossification in rectal carcinoma: report of a case and review of the literatureCase Rep Oncol 2016 9(3):698-704.10.1159/00045229727920705 [Google Scholar] [CrossRef] [PubMed]
[5]. Liu X, Xu J, Chen L, Colorectal carcinoma with osseous metaplasiaOncotarget 2017 8(39):65407-13.10.18632/oncotarget.18577 [Google Scholar] [CrossRef]
[6]. Kim GY, Kim J, Kim TS, Han J, Pulmonary adenocarcinoma with heterotopic ossificationJ Korean Med Sci 2009 24(3):504-10.10.3346/jkms.2009.24.3.50419543517 [Google Scholar] [CrossRef] [PubMed]
[7]. Noh BJ, Kim YW, Park YK, A rare colon cancer with ossification: pathogenetic analysis of bone formationAnn Clin Lab Sci 2016 46(4):428-32. [Google Scholar]
[8]. Imai N, Iwai A, Hatakeyama S, Matsuzaki K, Kitagawa Y, Kato S, Expression of bone morphogenetic proteins in colon carcinoma with heterotopic ossificationPathol Int 2001 51(8):643-48.10.1046/j.1440-1827.2001.01243.x11564221 [Google Scholar] [CrossRef] [PubMed]
[9]. Haque S, Eisen RN, West AB, Heterotopic bone formation in the gastrointestinal tractArch Pathol Lab Med 1996 120(7):666-70. [Google Scholar]
[10]. Weidner N, Zekan P, Carcinosarcoma of the colon. Report of a unique case with light and immunohistochemical studiesCancer 1986 58(5):1126-30.10.1002/1097-0142(19860901)58:5<1126::AID-CNCR2820580525>3.0.CO;2-Q [Google Scholar] [CrossRef]
[11]. Agnihotri S, Sarma N, Jeebun N, Srivastava R, Osseous metaplasia in adenocarcinomo of the rectum: a case reportThe Internet Journal of Gastroenterology 2007 7(1):1-4.10.5580/479 [Google Scholar] [CrossRef]