Introduction
Glenohumeral Internal Rotation Deficit (GIRD) indicates a 15° or greater loss of internal rotation of the throwing shoulder compared with the non-dominant shoulder.
Aim
To estimate the prevalence of GIRD in collegiate overhead sports player and determine whether GIRD is associated with scapular dyskinesia and rotator cuff strength ratio.
Materials and Methods
The present study was a Cross-sectional study. A total of 127 collegiate athletes were assessed for passive range of motion, external to internal rotation strength ratio (ER/IR ratio) and scapular dyskinesia for the throwing and non-throwing shoulder. Internal and external rotation of shoulder was measured using an inclinometer with the subject in prone and arm abducted to 90°. Scapular dyskinesia was measured using Lateral Scapula Slide test (LSST) and external to internal rotator strength was measured using a held hand isometric dynamometer. Chi-square test was used to find the association between GIRD and scapular dyskinesia and rotator cuff strength ratio.
Results
Prevalence of GIRD (n=37) was found to be 29.1%. GIRD was not found to be associated with Scapular dyskinesia (p=0.237) and ER/IR strength ratio (p=0.411).
Conclusion
Prevalence of GIRD in collegiate athletes playing overhead sports was found to be 29.1% and there was no association of GIRD with scapular dyskinesia, rotator cuff strength ratio.
Internal external rotators, Overhead athlete, Throwing adaptations, Throwing athlete, Throwing shoulder
Introduction
The nature of sports which collegiate athletes play is similar to elite athletes, however, they differ in terms of the amount of participation, practice, and training. This difference can play a significant role in the difference of injury profile of these two groups [1,2]. Overhead sporting activities entails the synchronisation of large forces from lower to upper extremitie generating velocities required for throwing activities [3]. The repetitive throwing action causes large mechanical stress on the glenohumeral and elbow joints of the athletes due to the torque and distraction involved [3]. These continuous stresses have been assumed to cause chronic degenerative changes in athletes [2]. There has been increased incidence of shoulder injuries among collegiate non-professional athletes involved in overhead throwing activities. GIRD is one such common condition seen in overhead throwing athletes, causing decrease in internal rotation of the throwing shoulder as compared to contralateral shoulder [4]. GIRD has also been suggested to cause many scapulars as well as shoulder complex variations, predisposing the young athletic shoulder for more injuries [4].
Scapular dyskinesia is defined as a visible alteration in motion and position of scapula with respect to the thoracic cage [5]. There have been studies suggesting these alterations such as protraction, anterior tilting and decreased upward rotation in the baseball players which can lead to abnormal functioning of the shoulder complex [6]. Even though the scapular dyskinesia pattern has been labelled in association with GIRD in elite athletes, the nature of its association has not been clarified in the non-professional collegiate athletes [6]. Collegiate athletes as compared to the elite population are exposed to different levels of stress on the shoulder joint and thus might differ in the incidence, type, and magnitude of injury warranting the need to identify if those factors identified in elite players are prevalent in collegiate players also [7].
Electromyography (EMG) analysis has shown that adequate rotator cuff muscle group strength is required during throwing as they produce eccentric activity, especially for shoulder external rotators during follow through phase of throwing [8]. Therefore, athletes should have adequate internal and external shoulder rotator muscle strength [8]. The studies have suggested that rotator cuff strength is associated with glenohumeral joint adaptations and protection [9]. Such adaptations and protective mechanism have been seen in athletes with GIRD [9].
There is a dearth of the literature regarding the prevalence of GIRD and how it affects Scapular dyskinesia and rotator cuff strength ratio in collegiate overhead athletes. Thus, the present study aimed to find out the prevalence of GIRD and its association with scapular dyskinesia and rotator cuff strength ratio.
Materials and Methods
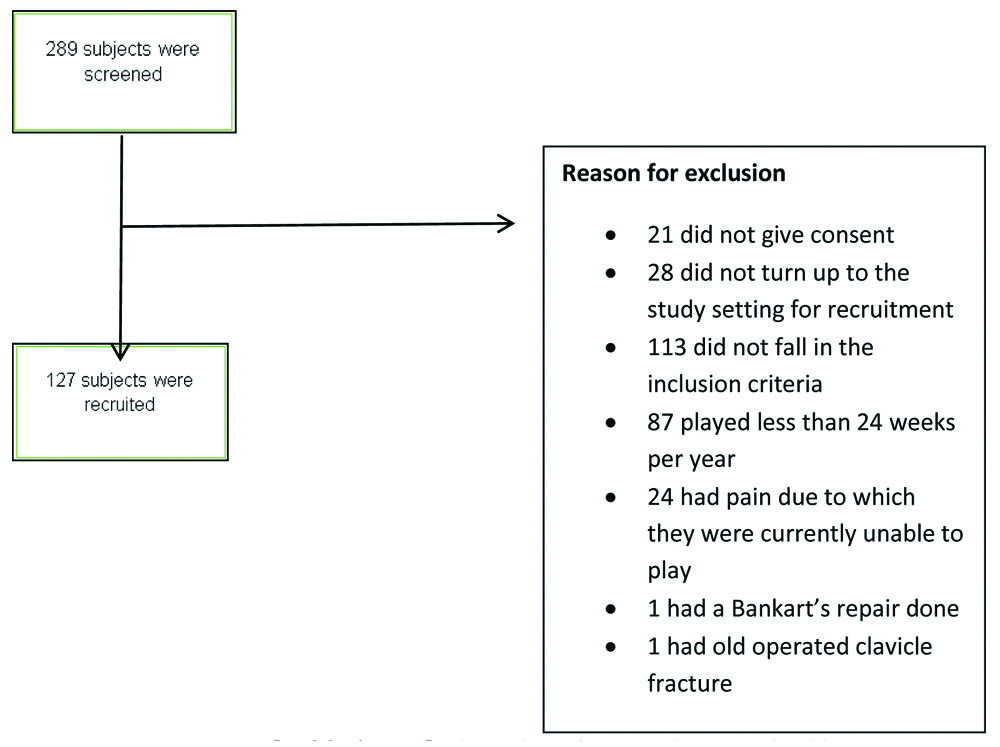
In the present cross-sectional study design, conducted for a total of two years from July 2015 to July 2017 at the Manipal Academy of Higher Education, a total of 289 collegiate recreational athletes aged between 17 to 30 years of either gender were screened. Subjects involved in overhead throwing activities for a minimum of at least 24 weeks a year were included in the study. A total of 289 subjects were screened, recruitment flowchart has been shown in [Table/Fig-1]. Out of total subjects screened 127 subjects (males n=110 and female=17) were included in the study as based on exclusion and inclusion criteria. Participants were excluded if they had a prior history of orthopaedic surgery or fractures in the upper limbs and/or cervical region as well as systemic diseases and/or metabolic disorders. Sample size was calculated using formula N=(Z-α/2)2p.q/(p.d)2, level of significance (α) was kept at 5%, p was based on prevalence of GIRD, ‘q=1-p’ and ‘d’ is margin of error: 0.2. Study approval was sought from Institutional Ethics Committee of the university (IEC 102/2016). Subject information sheet was given to the participants and informed consent was taken. Demographics of the subject were recorded and shoulder girdle musculoskeletal evaluation which included scapular internal and external range of motion, shoulder internal and external rotation strength ratio, forward head posture analysis, scapular position, scapula-thoracic ration and scapular upward rotation was done.
Flow chart for recruitment of subjects.
Shoulder Internal and External Rotation Measurement
Shoulder internal and external rotation was measured using standard procedures with OTRMAX Circular Aluminum Case gravitational inclinometer [10]. For measurement of shoulder internal rotation, the elbow was at 90° in flexion with forearm fully pronated. Elbow should be in the patient’s side for maintaining shoulder in neutral. Inclinometer was placed along the shaft of the radius, perpendicular to the movement plane [10]. For shoulder external rotation, the elbow was kept at 90° flexion, forearm fully pronated and inclinometer was placed perpendicular to the movement along the shaft of ulna [10].
Lateral Scapular Slide Test (LSST)
LSST was done to measure scapular dyskinesia [11]. In LSST measurements are taken from the spine of scapulae to T2/T3, Inferior angle of scapulae to T7/T9 and superior angle of the scapulae to T2 [11]. The measurements are taken in three positions, (A) sitting/standing with arms resting on the side, (B) Hands on the waist, Thumbs Posteriorly (45 abductions), (C) 90° abduction and maximal internal rotation [11]. The measurement should not vary more than 1 to 1.5 cm, more the 1.5 cm difference significant. LSST has ICC of 0.83 to 0.96, which means, it can provide more objective measurement of scapular position than observation [11].
Rotator Cuff Strength
Rotator cuff strength was assessed by standard procedures using Chatillon MSE100 hand-held dynamometer [12]. The subject was in sitting position and with arm supported at 90° of abduction and neutral rotation. The subject performed glenohumeral external and internal rotation against the hand-held dynamometer [12]. Readings were compared with the normative values.
Statistical Analysis
Data were analysed using SPSS version 15.0. Tests for normality were done using chi-square test. Normally distributed data were represented as mean and standard deviation. The level of significance was kept at p≤0.05. Chi-square test was used to find the association between GIRD, scapular dyskinesia, ER/IR strength ratio, forward head and forward shoulder posture and past injury.
Results
The demographic data of the subjects are shown in [Table/Fig-2]. Mean age (years) of the subjects was 21.75±2.65. There were n=110 (86.61%) male subjects and n=17 (13.38%) females. Number of days per year subjects played overhead sports were 246.66±32.76. The prevalence of GIRD among collegiate overhead athletes was found to be 29.1%. Out of total participants, 37 athletes had GIRD. There was no clinical significance shown between GIRD and scapular dyskinesia (p=0.237), GIRD and rotator cuff strength (p=0.411) as shown in [Table/Fig-3], chi-square test was used for statistical analysis. the association between GIRD and ER/IR strength ratio and past injury using chi-square test are shown in [Table/Fig-4]. The percentage of recreational athletes playing various sports are shown in [Table/Fig-5].
Demographics of the participants.
| Demographic data expressed as (Mean±SD) (n=127) |
|---|
| Age in years | 21.75±2.65 |
|---|
| Males | 110 |
| Females | 17 |
| No. of days played per year | 246.66±32.76 |
| Past injury | 49 (38.58%) |
Association between GIRD, scapular dyskinesia, ER/IR strength ratio using chi-square test.
| Variable | p-value |
|---|
| GIRD and scapular dyskinesia | 0.237 |
| GIRD and ER/IR strength ratio | 0.411 |
Association between GIRD and ER/IR strength ratio and past injury using chi-square test.
| Variable | Mean | p-value |
|---|
| GIRD and scapular dyskinesia | 1.409 | 0.237 |
| GIRD and ER/IR strength ratio | 0.677 | 0.411 |
| GIRD and past injury | 5.274 | 0.022 |
| GIRD and FSP* | 2.129 | 0.211 |
| GIRD and FHP# | 1.929 | 0.587 |
| ER/IR strength ratio and past injury | 3.457 | 0.046 |
*forward shoulder posture, #forward head posture
Percentage of recreational athletes playing various sports.
| Sports played | Percentage of people playing |
|---|
| Cricket | 60 (47.2%) |
| Baseball | 1 (0.8%) |
| Basketball | 34 (26.8%) |
| Throw ball | 8 (6.3%) |
| Volleyball | 15 (11.8%) |
| Badminton | 59 (48.5%) |
| Lawn tennis | 8 (6.3%) |
| Squash | 2 (1.6%) |
Discussion
The study focused on determining the prevalence of GIRD and its association with scapular dyskinesia, External And Internal Rotators (ER/IR) strength ratio, forward shoulder and forward head posture and scapula upward rotation in collegiate athletes playing overhead sports. This study showed that no association exists between GIRD, scapular dyskinesia, ER/IR strength ratio in collegiate athletes playing overhead sports.
The presence of GIRD did not show a significant association with the presence of decreased ER/IR strength ratio these findings differ to a study done on elite and adolescent baseball players [13,14]. These studies measured the eccentric ER to concentric IR strength ratios, present study, on the other hand, evaluated the isometric ER to isometric IR strength ratio giving rise to a different result. Studies have also found that there can be acute changes in the shoulder rotation range and ER/IR strength ratios even after a single sports session, thus these results could have been affected by the time interval between the last game and testing [13,14]. Most of the studies have shown association between strength and GIRD however the studies have evaluated strength profile in elite athletes. This present study population was recreational athletes. These studies have evaluated isokinetic strength, isometric strength and some studies have done strength evaluation after a warm-up session. However, warm-up session was not included in the present study, therefore most of the studies have different result from this study [14].
There is an increased load on the rotator cuff muscles during the act of throwing. Internal rotators need to contract concentrically to propel the throwing or hitting arm forward while External rotators are subjected to high eccentric loads in order to counteract the force of internal rotators and to stabilise the humeral head in the glenoid [13,14]. Due to repeated trauma and eccentric load, external rotators are prone to get injured and weaker [15,16]. Therefore a balance between external to internal rotator strength is necessary. When there is an imbalance between these muscle group that is weaker external rotators and stronger internal rotators the throwing athlete is more prone to injuries [15,17,18]. The result of present study has been similar to that in the literature, demonstrating a significant association between decreased ER/IR strength ratio and presence of injury in collegiate athletes involved in overhead sports [19].
The results of the study pertaining to the association of GIRD with scapular dyskinesia and ER/IR strength ratio have not been consistent with other studies where they found an association with GIRD, this might be because of the subject’s characteristics [20]. Subjects in most of the studies were elite throwing athletes who differ in the number of levels of training, participation and practice [21-23]. Other than that the acute response of the shoulder musculature, range of motion differences could be possible reasons for the variation in the findings [21].
The findings of the study are different from the study done by Borich MR et al., they found a significant relationship between scapular positioning and GIRD [24]. This can be because the population involved in the study were elite athletes, whose frequency of participating in the sports was much higher than present study population, therefore, the number of overuse injuries will be much higher [25].
The group of participants included in the study were homogeneous with respect to demographic characteristic except for the unequal number of male and female athletes (110:17). 38.58% of athletes had a history of past injury which resulted in loss of playing days.
The primary objective was to find the prevalence of GIRD and its association with scapular dyskinesia and rotator cuff strength ratio in collegiate athletes. The prevalence of GIRD (29.1%) found in the present study is consistent with those found in the elite athletes playing overhead sports [26,27]. The presence of scapular dyskinesia was found to be 33%, however, there was no association between GIRD and scapular dyskinesia, which differ from the findings in the literature [17,28]. Various other soft tissue mechanisms such as tightness of pectoralis major and biceps other than GIRD or posterior capsule tightness can result in scapular dyskinesia [29].
Limitation
The results of the study provided information regarding the prevalence of Glenohumeral Internal Rotation Deficit and its association with Scapular Dyskinesia and Rotator Cuff strength ratio in collegiate athletes playing overhead sports, limitation must be acknowledged. The cross-sectional evaluation of the players was done. It would be beneficial to evaluate players in a longitudinal study, and however, it is difficult due to their academic paths and geographical mobility.
Conclusion
Prevalence of Glenohumeral Internal Rotation Deficit in collegiate athletes playing overhead sports was found to be 29.1% and there was no association of GIRD with scapular dyskinesia, rotator cuff strength ratio.
*forward shoulder posture, #forward head posture
[1]. Hilibrand MJ, Hammoud S, Bishop M, Woods D, Fredrick RW, Dodson CC, Common injuries and ailments of the female athlete; pathophysiology, treatment and preventionThe Physician and sportsmedicine 2015 43:403-11.10.1080/00913847.2015.109285626458108 [Google Scholar] [CrossRef] [PubMed]
[2]. Lubiatowski P, Kaczmarek PK, Slezak M, Dlugosz J, Breborowicz M, Dudzinski W, Problems of the glenohumeral joint in overhead sports-literature review. Part II-pathology and pathophysiologyPolish Orthopedics and Traumatology 2014 79:59-66. [Google Scholar]
[3]. Kaczmarek PK, Lubiatowski P, Cisowski P, Grygorowicz M, Lepski M, Dlugosz J, Shoulder problems in overhead sports. Part I-biomechanics of throwingPolish Orthopedics and Traumatology 2014 79:50-58. [Google Scholar]
[4]. Whiteley R, Oceguera M, GIRD, TRROM, and humeral torsion-based classification of shoulder risk in throwing athletes are not in agreement and should not be used interchangeablyJournal of Science and Medicine in Sport 2016 19:816-19.10.1016/j.jsams.2015.12.51926861672 [Google Scholar] [CrossRef] [PubMed]
[5]. Carbone S, Postacchini R, Gumina S, Scapular dyskinesis and SICK syndrome in patients with a chronic type III acromioclavicular dislocationResults of rehabilitation. Knee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA 2015 23:1473-80.10.1007/s00167-014-2844-524458335 [Google Scholar] [CrossRef] [PubMed]
[6]. Almeida GPL, Silveira PF, Rosseto NP, Barbosa G, Ejnisman B, Cohen M, Glenohumeral range of motion in handball players with and without throwing-related shoulder painJournal of Shoulder and Elbow Surgery 2013 22:602-07.10.1016/j.jse.2012.08.02723177170 [Google Scholar] [CrossRef] [PubMed]
[7]. Lemoyne J, Poulin C, Richer N, Bussieres A, Analysing injuries among university-level athletes: prevalence, patterns and risk factorsJ Can Chiropr Assoc 2017 61(2):88-95. [Google Scholar]
[8]. Seroyer ST, Nho SJ, Bach BR, Bush-Joseph CA, Nicholson GP, Romeo AA, The kinetic chain in overhand pitching: its potential role for performance enhancement and injury preventionSports Health 2010 2(2):135-46.10.1177/194173811036265623015931 [Google Scholar] [CrossRef] [PubMed]
[9]. Chalmers PN, Wimmer MA, Verma NN, Cole BJ, Romeo AA, Cvetanovich GL, The Relationship Between Pitching Mechanics and Injury: A Review of Current ConceptsSports Health 2017 9(3):216-221.10.1177/194173811668654528107113 [Google Scholar] [CrossRef] [PubMed]
[10]. Green S, Buchbinder R, Forbes A, Bellamy N, A standardized protocol for measurement of range of movement of the shoulder using the Plurimeter-V inclinometer and assessment of its intrarater and interrater reliabilityArthritis care and research: the official journal of the Arthritis Health Professions Association 1998 11:43-52.10.1002/art.17901101089534493 [Google Scholar] [CrossRef] [PubMed]
[11]. Shadmehr A, Azarsa MH, Jalaie S, Inter- and intrarater reliability of modified lateral scapular slide test in healthy athletic menBioMed research international 2014 2014:38414910.1155/2014/38414924900963 [Google Scholar] [CrossRef] [PubMed]
[12]. Cools AMJ, Vanderstukken F, Vereecken F, Duprez M, Heyman K, Goethals N, Eccentric and isometric shoulder rotator cuff strength testing using a hand-held dynamometer: reference values for overhead athletesKnee Surgery, Sports Traumatology, Arthroscopy: Official Journal of the ESSKA 2016 24:3838-47.10.1007/s00167-015-3755-926294055 [Google Scholar] [CrossRef] [PubMed]
[13]. Trakis JE, McHugh MP, Caracciolo PA, Busciacco L, Mullaney M, Nicholas SJ, Muscle strength and range of motion in adolescent pitchers with throwing-related pain: implications for injury preventionThe American Journal of Sports Medicine 2008 36:2173-78.10.1177/036354650831904918596197 [Google Scholar] [CrossRef] [PubMed]
[14]. Hurd WJ, Kaplan KM, Eiattrache NS, Jobe FW, Morrey BF, Kaufman KR, A profile of glenohumeral internal and external rotation motion in the uninjured high school baseball pitcher, part I: motionJournal of Athletic Training 2011 46:282-88.10.4085/1062-6050-46.3.28221669098 [Google Scholar] [CrossRef] [PubMed]
[15]. Mlynarek RA, Lee S, Bedi A, Shoulder Injuries in the Overhead Throwing AthleteHand Clinics 2017 33:19-34.10.1016/j.hcl.2016.08.01427886835 [Google Scholar] [CrossRef] [PubMed]
[16]. Saccol MF, Gracitelli GC, da Silva RT, Laurino CFdS, Fleury AM, Andrade MdS, Shoulder functional ratio in elite junior tennis playersPhysical therapy in sport: official journal of the Association of Chartered Physiotherapists in Sports Medicine 2010 11:8-11.10.1016/j.ptsp.2009.11.00220129117 [Google Scholar] [CrossRef] [PubMed]
[17]. Reinold MM, Gill TJ, Current concepts in the evaluation and treatment of the shoulder in overhead-throwing athletes, part 1: physical characteristics and clinical examinationSports Health 2010 2:39-50.10.1177/194173810933854823015922 [Google Scholar] [CrossRef] [PubMed]
[18]. Stanley A, McGann R, Hall J, McKenna L, Briffa NK, Shoulder strength and range of motion in female amateur-league tennis playersThe Journal of orthopaedic and sports physical therapy 2004 34:402-9.10.2519/jospt.2004.34.7.40215296368 [Google Scholar] [CrossRef] [PubMed]
[19]. Shanley E, Thigpen C, Throwing injuries in the adolescent athleteInternational Journal of Sports Physical Therapy 2013 8:630-40. [Google Scholar]
[20]. Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM, Glenohumeral range of motion deficits and posterior shoulder tightness in throwers with pathologic internal impingementAm J Sports Med 2006 34(3):385-91.10.1177/036354650528180416303877 [Google Scholar] [CrossRef] [PubMed]
[21]. Kibler WB, Sciascia A, Thomas SJ, Glenohumeral internal rotation deficit: pathogenesis and response to acute throwingSports Med Arthrosc Rev 2012 20(1):34-08.10.1097/JSA.0b013e318244853e22311291 [Google Scholar] [CrossRef] [PubMed]
[22]. Gissis I, Papadopoulos C, Kalapotharakos VI, Sotiropoulos A, Komsis G, Manolopoulos E, Strength and speed characteristics of elite, subelite, and recreational young soccer playersRes Sports Med 2006 14(3):205-14.10.1080/1543862060085476916967772 [Google Scholar] [CrossRef] [PubMed]
[23]. Chrisman SP, O’Kane JW, Polissar NL, Tencer AF, Mack CD, Levy MR, Strength and jump biomechanics of elite and recreational female youth soccer playersJ Athl Train 2012 47(6):609-615.10.4085/1062-6050-47.6.0123182007 [Google Scholar] [CrossRef] [PubMed]
[24]. Borich MR, Bright JM, Lorello DJ, Cieminski CJ, Buisman T, Ludewig PM, Scapular angular positioning at end range internal rotation in cases of glenohumeral internal rotation deficitJ Orthop Sports Phys Ther 2006 36(12):926-34.10.2519/jospt.2006.224117193870 [Google Scholar] [CrossRef] [PubMed]
[25]. Wijdicks CA, Rosenbach BS, Flanagan TR, Bower GE, Newman KE, Clanton TO, Injuries in elite and recreational snowboardersBr J Sports Med 2014 48(1):11-07.10.1136/bjsports-2013-09301924282020 [Google Scholar] [CrossRef] [PubMed]
[26]. Tokish JM, Curtin MS, Kim Y-K, Hawkins RJ, Torry MR, Glenohumeral internal rotation deficit in the asymptomatic professional pitcher and its relationship to humeral retroversionJournal of Sports Science & Medicine 2008 7:78-83. [Google Scholar]
[27]. Chant CB, Litchfield R, Griffin S, Thain LMF, Humeral head retroversion in competitive baseball players and its relationship to glenohumeral rotation range of motionThe Journal of Orthopaedic and Sports Physical Therapy 2007 37:514-20.10.2519/jospt.2007.244917939610 [Google Scholar] [CrossRef] [PubMed]
[28]. Olsen SJn, Fleisig GS, Dun S, Loftice J, Andrews JR, Risk factors for shoulder and elbow injuries in adolescent baseball pitchersThe American Journal of Sports Medicine 2006 34:905-12.10.1177/036354650528418816452269 [Google Scholar] [CrossRef] [PubMed]
[29]. McKenna L, Straker L, Smith A, Cunningham J, Differences in scapular and humeral head position between swimmers and non-swimmersScandinavian Journal of Medicine & Science in Sports 2011 21:206-14.10.1111/j.1600-0838.2009.01039.x20030781 [Google Scholar] [CrossRef] [PubMed]