It has been six decades since the implantation of the first Permanent Pacemaker (PPM). Arne Larsson, the first patient who underwent PPM implantation in 1958, went on receiving 26 different pacemakers for the next 43 years of his life and died at the age of 86 [1]. Nevertheless, PPMs have changed significantly since the first implant, from asynchronous single chamber devices to rate responsive dual/multi chamber devices. The PPMs have become more sophisticated and complex instruments. The initial mercury-iodide and nickel-cadmium batteries have been replaced by the use of lithium powered batteries which has increased the life of PPMs as long as 15 years while the former ones had life span of approximately 2.5 years [2]. The PPMs have evolved in terms of battery endurance, software and programme, lead performance, implantation techniques and size. Recently leadless pacemakers have been available in size similar to a large capsule which can be remotely monitored [2]. The cost of the pacemaker implantation depends on several factors like; the technology used in the pacemaker, incision location and type of incision, patient’s general health. The cost of device alone varies from 45,000 to 3,00,000 INR. Pacemakers have become a routine treatment for cardiac conductive disorders [3]. There has been a steep upswing in pacemaker implantation in last few decades due to widening of the indication for pacemaker implantation and availability of newer technology [4]. Currently, worldwide there are more than 3 million people with a pacemaker or other cardiac rhythm management device and each year >700,000 new pacemakers are implanted [2,5].
Materials and Methods
A total of 1551 patients who underwent PPM implantation between December 1999 and February 2014 were included in this single centre, retrospective study. The study was performed at a tertiary care hospital located in India. There were no exclusion criteria; the patients who underwent first PPM implantation at our centre during the specified study period were included in this study. Before the discharge of patient from the hospital, data release consent was taken from each patient, which has been the practice of associated hospitals, irrespective of any study to be conducted in the future and the study protocol was approved by Institutional Ethics Committee.
Data analysis was based upon patient’s age, gender, indication of pacemaker implantation (complete heart block, sick sinus syndrome, syncope, cardiomyopathy, pulse generator replacement), surgical parameters (type of pocket, access site, pacing lead and fixation of pacing lead), modes of pacing (single chamber/dual chamber and DDD/DDDR/AAIR/VDD/VVI/VVIR), the pacing parameters (impedance and threshold), and financial assistance (self paid, state/central government health schemes, private insurance, donated).
Continuous variables were presented as mean±Standard Deviation (SD) and categorical variables as counts and percentages. All the data were analysed using the Statistical Package for Social Sciences Software (Version 15.0, SPSS; Chicago, IL, USA).
Results
The age distribution of patients who underwent PPM implantation ranged from 2 to 97 years, the mean age of the population was 60.1±16.7 years. Of the total population 881 (56.8%) were males. Patients aged between 51-70 years procured 782 (50.4%) PPMs, PPM implantation as per age distribution of patients is given in [Table/Fig-1]. The mean age of males and females were 60.7±17.0 and 59.4±16.3 years, respectively.
Basic characteristics of patients.
| Characteristics | Patients (N=1551) |
|---|
| Average age (mean±SD, years) | 60.1±16.7 |
| Male, n (%) | 881 (56.8%) |
| Age |
| 2-20, n (%) | 54 (3.5%) |
| 21-50, n (%) | 325 (21%) |
| 51-70, n (%) | 782 (50.4%) |
| 71-97, n (%) | 390 (25.1%) |
SD: Standard deviation
Degenerative complete heart block, the prime indication for pacemaker implantation, comprised of 1059 (68.3%) patients; followed by sick sinus syndrome affecting 140 (9.0%) patients. Other indications for pacemaker implantation are given in [Table/Fig-2].
Indications for pacemaker implantation.
| Indication | Patients (N=1551) |
|---|
| Degenerative complete heart block, n (%) | 1059 (68.3%) |
| 2:1 AV block, n (%) | 121 (7.8%) |
| High grade AV block, n (%) | 26 (1.7%) |
| Congenital complete heart block, n (%) | 62 (4.0%) |
| Post-operative complete heart block, n (%) | 11 (0.7%) |
| Sick sinus syndrome, n (%) | 140 (9.0%) |
| Pulse generator replacement, n (%) | 125 (8.0%) |
| Hypertrophic cardiomyopathy, n (%) | 2 (0.1%) |
| Neurocardiogenic syncope, n (%) | 5 (0.3%) |
AV: Atrioventricular
In 1485 (95.7%) patients, the pacemaker was implanted in pre-pectoral vicinity. The access sites were cephalic vein and thoracic axillary vein in 679 (43.8%) and 872 (56.2%) patients, respectively. Most of the patients acquired bipolar pacing leads and the fixation of pacing leads were active and passive in 335 (21.6%) and 1216 (78.4%) patients, respectively. [Table/Fig-3] illustrates various surgical parameters like access sites, pacing leads and its fixation, pocket for implantation. The impedance values were between 500-1000 Ω in 1437 (92.6%) patients and the threshold of pacing was less than 1 volt in 1488 (95.9%) patients.
Surgical parameters during pacemaker implantation.
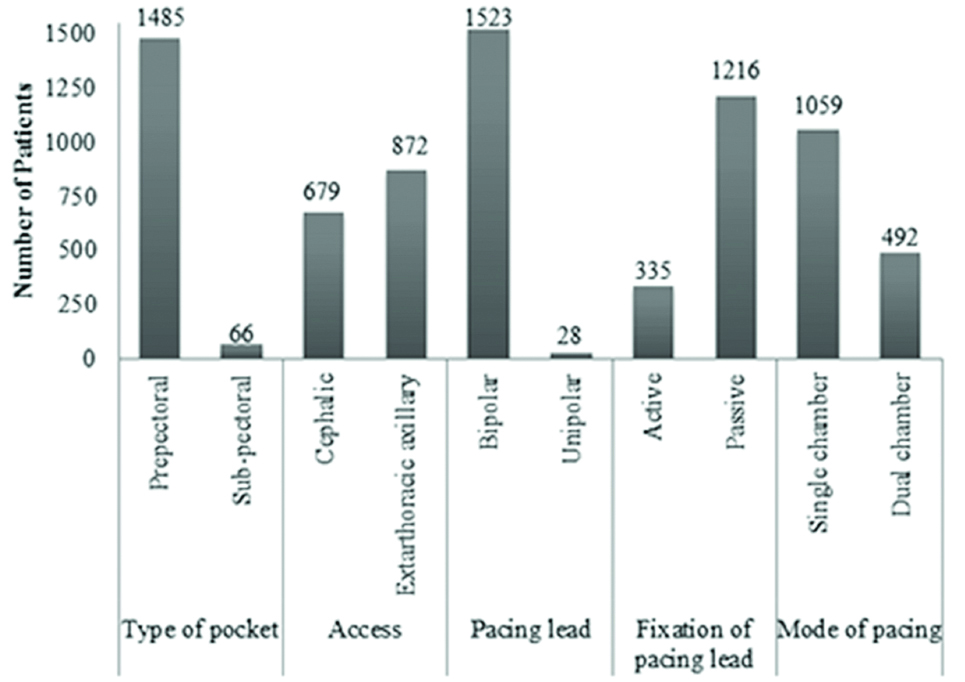
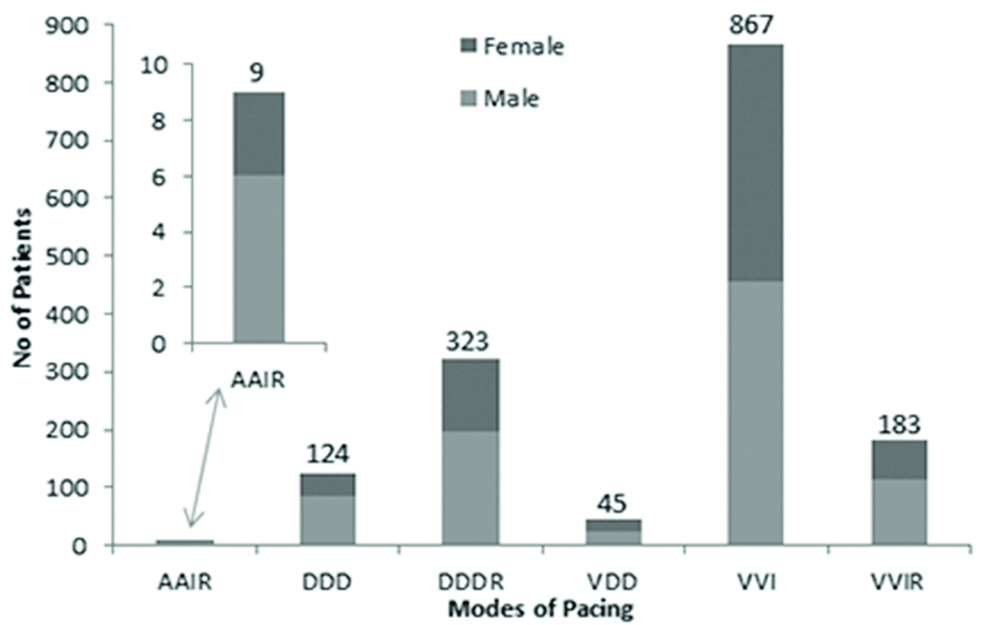
Single chamber and dual chamber pacemaking devices were implanted in 1059 (68.3%) and 492 (31.7%) patients, respectively. The VVI pacemakers were implanted in 867 (55.9%) patients, where 456 (51.8%) male population and 411 (61.3%) female population acquired the VVI pacemaker. Further modes of pacing are provided in [Table/Fig-4].
Mode of pacing in population.
The patients were also analysed as per their financial assistance. Eight hundred and twenty patients (52.9%) were self-paid. State government health scheme provided aid to 301 (19.4%) of patients. Further financial insights are given in [Table/Fig-5].
Financial assistance for pacemaker implantation.
| Financial Assistance | Patients (N=1551) |
|---|
| Self-paid, n (%) | 820 (52.9%) |
| State government health scheme, n (%) | 301 (19.4%) |
| Central government health scheme, n (%) | 270 (17.4%) |
| Private insurance, n (%) | 45 (2.9%) |
| Explanted/Donated, n (%) | 115 (7.4%) |
Discussion
In the present study, of the total population who underwent pacemaker implantation, number of male patients were higher than the females (56.8% vs. 43.2%), these number were similar to a single centre study conducted in Northern Greece where 54% of patients were male [7]. These data were also identical to the 11th world survey for cardiac devices where male population was predominantly higher than the female (68% vs. 32%) [6]. The mean age of population in our study was 60.1 years, these outcomes are identical to a study published in 2017 [8], conducted in Poland, where the mean age was 63.5 years but findings are contradictory to other registries and world survey where mean age ranged from 65 to 80 years for PPM implantation [9-13]. There was not much difference between the age of men and women (60.7 and 59.4 years, respectively), in the 11th world survey conflicting results were obtained where males tend to underwent pacemaker surgery at younger age than females [6].
The indications for PPM implantation were parallel with New Zealand registry, in terms of order of indication, where degenerative complete heart block was the prime indicator for implantation (68.3% vs. 29%); followed by sick sinus syndrome (9% vs. 19%) and second degree atrioventricular block (7.8% vs. 11%) [14]. Pacemaker registry of Netherlands showed sick sinus syndrome as the prime indicator (42.3%) for pacemaker implantation followed by heart block (38.9%) [15] and Swedish pacemaker registry reported atrioventricular conduction disorders (38%) as the commonest cause followed by sick sinus syndrome (34%) [10].
In this study, single chamber pacemakers were implanted in more than two third patients (68.3%). The VVI and VVIR pacemakers were used predominantly followed by DDDR and DDD pacemakers. One of the possible reasons for using more single chamber devices could be financial constraints of patients. However, studies that compared trends in PPM, showed that the use of dual chamber pacemaker has elevated with time [16,17]. Italian pacemaker registry showed use of dual chamber pacemaker in 65% patients [18]. According to 11th world survey of cardiac pacing and implantable cardioverter-defibrillators conducted in 2009, the overall use of dual chamber pacemakers have increased in most of the countries [6]. Many developing countries like India still use more number of single chamber devices than the more advanced dual chamber devices. The use of AAIR and VDD pacemakers was meagre in the current study.
The total cost of PPM and surgery is quite high, the cost and risks associated with pacemakers also increases as more advanced generation of pacemakers are used [19-21], many patients who want to yield a healthy and productive life with a pacemaker, can’t afford it. Hence, the selection of the pacemaker is affected by financial status of patients; this could be the reason for predominantly higher use of less expensive single chamber devices in this study. In this study, about half of the patients (47.1%) used different financial aids for implantation of a PPM and the other half were self-paid (52.9%). In present study, more than one third of the total population were able to obtain a pacemaker by receiving financial assistance from the government, under either state or central government schemes like Yesheswani, Hriduya Sanjeevani Scheme, Vajpayee Arogyasri, Chief Minister Relief Fund, Arogya Bhagya, Employee State Insurance and Central Government Health Scheme. The conception of using refurbished pacemaker has been utilised since the inception of pacemakers, in many cases a pulse generator had outlived the patient and such valuable resources should be refurbished. Various studies have already been performed which confirm that the pacemaker can be recycled and implanted to a second patient without any major complications [22,23]. Similarly in this study, 115 patients (7.4%) received explanted/donated pacemakers. Even after pacemaker implantation, there are chances of infection, haematoma, pneumothorax etc., to overcome such problems patients should be evaluated routinely for pacemaker activity and patient counselling should be conducted for necessary lifestyle changes. A nationwide registry should be established which aims to collect and track demographic profiles of patients undergoing pacemaker and other cardiac device implantation; such an initiative could help provide data of on-going trends, availability and acceptance of newer technology and various financial benefits from central and state government. Such an initiative would ensure that data are more relevant to the Indian population can be obtained and used for the betterment of patients.
Limitation
This was a single centre study and the nationwide data might represent different trends in PPM implantation. There was no follow-up post PPM implantation.
Conclusion
From this demographic study, one can conclude that, male population were implanted with a higher number of pacemakers than females. Males and females underwent pacemaker implantation at similar age. The use of single chamber PPM was higher than the dual chamber. Degenerative complete heart block was the major cause for pacemaker implantation followed by sick sinus syndrome. A significant volume of patients received financial aids from various health schemes by central and state government.
SD: Standard deviation
AV: Atrioventricular