Fabrication of Silicone Prosthesis for an Amputated Pollex with Kapandji Score 8: A Case Report
Anshulika Singh1, Mayank Singh2, Saumyendra V Singh3, Pooran Chand4, Deeksha Arya5
1 Junior Resident, Department of Prosthodontics, Faculty of Dental Sciences, King George’s Medical University, Lucknow, Uttar Pradesh, India.
2 Assistant Professor, Department of Prosthodontics, Faculty of Dental Sciences, King George’s Medical University, Lucknow, Uttar Pradesh, India.
3 Professor, Department of Prosthodontics, Faculty of Dental Sciences, King George’s Medical University, Lucknow, Uttar Pradesh, India.
4 Professor and Head, Department of Prosthodontics, Faculty of Dental Sciences, King George’s Medical University, Lucknow, Uttar Pradesh, India.
5 Associate Professor, Department of Prosthodontics, Faculty of Dental Sciences, King George’s Medical University, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Saumyendra V Singh, 2/273, Viram Khand, Gomti Nagar, Lucknow-226010, Uttar Pradesh, India.
E-mail: saumyendravsingh@rediffmail.com
Amputations are most commonly seen due to the accidents, congenital malformations and diseases. Regardless of the cause of the loss of the part of the body, an amputation results in aesthetic, physical and psychosocial damage to an individual. An amputation can be surgically treated but in some cases where patient reports to the prosthetist, when the damage is irreversible, it can be treated with prosthetic replacements of the lost part. A prosthetist acts as an important link in helping such patients in regaining the lost confidence by rehabilitation. Prosthetic management of an amputated thumb aims to deliver a well-fitting silicone prosthesis that can mimic the opposite thumb as closely as possible, with good range of movement without dislodgement. This case report presents rehabilitation of the amputated thumb with minimal residual thumb in a conventional way along with restoring the range of movements with evaluation of the range of movement without the use of an extra retentive aid.
Prosthetic rehabilitation, Retentive aid, Trauma
Case Report
A 20-year-old female patient reported to the Department of Prosthodontics, with a chief complaint of missing thumb of right hand [Table/Fig-1]. History revealed the patient had lost her pollex in a traumatic injury when she was 1½-year-old.
Pre Rehabilitation clinical and radiographic view.
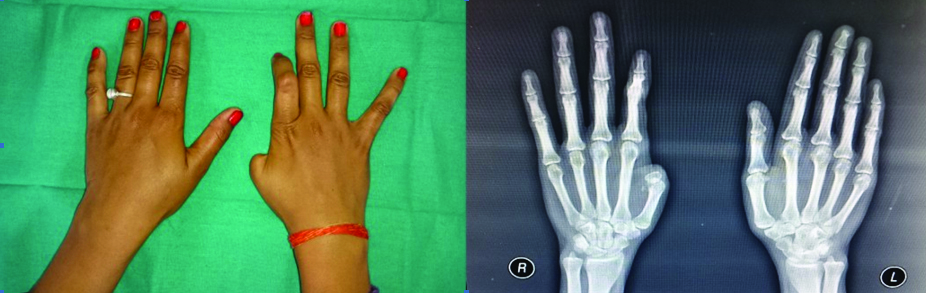
Physical and antero-posterior radiographic examination of right hand revealed amputated thumb at proximal phalanx [Table/Fig-1]. The index finger was osseointegrated at the interphalangeal joint of distal and middle phalanx in the flexed position because of an attempt to reattach the distal phalangeal portion at the time of injury. The patient was naturally not able to straighten the index finger [Table/Fig-1]. The skin of the amputated finger was completely healed.
The rehabilitation of her thumb was challenging due to level and site of amputation. The patient was informed about both possible treatment options-surgical reconstruction and prosthetic rehabilitation. But, due to surgical trauma and financial constraints, the patient agreed to prosthetic rehabilitation. So, thumb prosthesis was planned for the patient. As the patient was unwilling for any surgery, implant retained prosthesis was ruled out. Mechanical retention with devices such as Velcro strap would be quite discernible for pollex location. Therefore, glove type thumb prosthesis with retention aided by an incorporated wire in the silicone prosthesis was planned to work in harmony with the flexed osseointegrated index finger of the right hand.
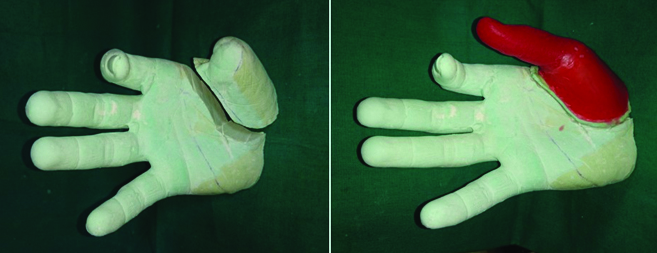
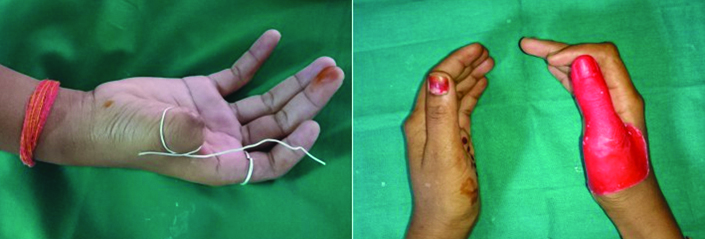
Patient was informed about the procedure and her consent was obtained. An impression of the right amputated thumb stump was made using irreversible hydrocolloid impression material (Zelgan) and poured with Type-III dental stone (Kalstone, Kalabhai Pvt., Ltd., Mumbai, India) to obtain the working model [Table/Fig-2]. Then 1 mm reduction was done all around the thumb stump to enhance fit to the elastic silicone prosthesis. After that, an impression of the patient’s left thumb was made with alginate and poured in molten modelling wax (Link dental modelling wax no. 2, MDM Corporation, Delhi, India). This wax pattern of the left thumb was adapted to pollex stump model [Table/Fig-2] and the borders were merged with the area adjacent to the defect site. A 20 gauge silver wire was incorporated into the wax pattern as an aid for mechanical retention of the prosthesis. It was adapted at the root of the stump extending upto the metacarpophalangeal joint of the index finger, attaching to a ring worn on the index finger [Table/Fig-3]. Fabrication of silicone prosthesis with incorporated wire to aid in retention is hardly documented. Anatomic crease lines were carved to give a more natural appearance. Then, the wax pattern was tried on the patient’s hand [Table/Fig-3]. Along with the shape and size, the fit, orientation, emergence and borders of the pattern were evaluated.
Working model and wax pattern adapted to the thumb stump.
Silver wire try in for wax pattern and the wax pattern tried on the patient’s hand.
The pattern was then invested in a two piece mould made using type I dental stone. The two piece mould was made by pouring the dorsal and palmer halves separately. The first pour enscoring the palmer half was made with type 1 dental stone, at slight angle. Keys were made into the first piece of mold and separating media was applied on the surface. This was followed by pouring the second half of the mold with type 1 dental stone. After the investment was set, dewaxing was done and moulds were obtained [Table/Fig-4]. The correct position of wire element was ascertained in the mold.
Dewaxed moulds and final prosthesis with open margins.

Appropriate shades were matched for both the dorsal and the palmer surfaces with the help of digital spectrometer. The pigments were quantitatively measured, mixed with the heat temperature vulcanising silicone and added to the dewaxed mould. Surface tension releasing agent was applied to the mold surfaces. The molds were compressed and the curing process was performed according to the manufacturer’s instructions. After curing, the prostheses was removed gently, trimmed and finished. The shade was evaluated and extrinsic colouring done to match the exact colour of the patient.
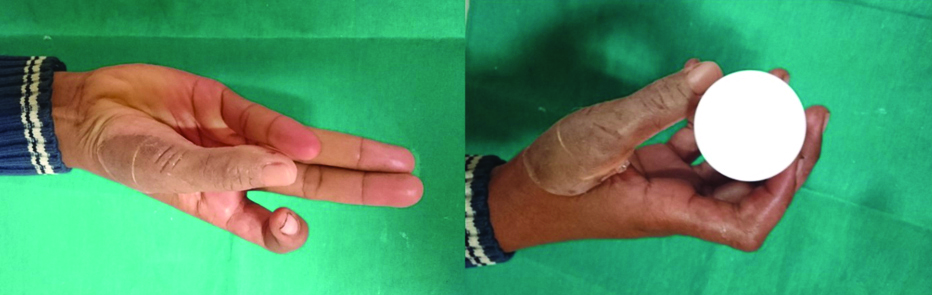
The prosthesis was inserted and retention was attempted by attaching the silver wire to a ring worn on the index finger. With this mode, prosthetic retention was good but on movement of the thumb the margins of the prosthesis opened up [Table/Fig-4]. So it was planned to cut the silver wire and medical adhesives were used for retaining the prosthesis [Table/Fig-5]. This also resulted in good retention and range of movement with a score of 8 as assessed with the help of Kapandji’s rule of 10 [1], where the patient was asked to touch ten specified areas of 4 fingers with the tip of the thumb. For assessment of the opposition of the thumb Kapandji score was used as a tool, based on where the tip of their thumb touches the patient’s hand [Table/Fig-6]. The patient was also asked to hold boxes of varying diameter to check for the grip [Table/Fig-6]. Post delivery the patient was instructed to remove the prosthesis daily and clean it with isopropyl alcohol, also asked to clean the underlying skin. A 6-month follow up for assessing the maintenance was planned for the patient.
Post Rehabilitation final prosthesis.

Kapandji score evaluation.
Discussion
Pollex is an important part of hand used to perform daily tasks including pinch, grip, grasp, and precision handling [2]. From functional standpoint it is the most important digit which performs the movements of opposition and apposition [3].
The patient is not able to perform various functional activities with the loss of thumb. The immediate loss of grasp, strength and security and the aesthetic impact may cause a great psychological trauma [4]. The thumb may be lost due to traumatic injuries or may be congenitally absent.
Traumatic amputation of thumb puts the patient through great aesthetic and psychological trauma, besides inability to perform functional movements, various gripping and opposing actions. To overcome these problems efforts are made to restore the lost thumb surgically or prosthetically. The first choice for treating amputated digits generally is surgical reconstruction while prosthetic rehabilitation may be considered in unsalvageable cases or in surgical reconstruction failure [5]. Options such as solitary digit transfer, bone lengthening or ray transposition allow for surgical reconstruction of lost digits achieving function and patient acceptance [6]. Prosthetic options include implant retained prosthesis which aids in higher degree of functional movements and aesthetics. Implant retained silicone finger prosthesis allow some pressure perception and tactile sensation, facilitating surface and texture distinction [7]. Tip pinch grip score can be used to determine the grip strength with marked pinch gauge, where the patient is asked to place the thumb under the gauge with the pulp of the index finger on top and dial facing upwards. This formed an O-shape whilst the other fingers are flexed [8]. However, there might be problems associated with loss of integration of these implants. Many patients do not agree to undergo surgery for implant or reconstruction due to surgical trauma, time consuming procedure and cost factors. Prosthetic replacement with mechanically retentive silicone prosthesis can serve as an acceptable option. This is non-invasive, less expensive and has good patient acceptance.
Similar case reports have been published for prosthetic rehabilitation of amputated finger/s [4,8], but rehabilitation has been without attempt at incorporation of wire. In the cases where stump length is severely reduced, there is associated difficulty in retention of the prosthesis. In such cases, where the patient is unwilling/unsuitable for osseointegrated implants, wire incorporation in silicone prosthesis might aid in retention.
Conclusion
This thumb prosthesis was designed to be fabricated with a silver wire incorporated, which would be attached with a ring to be worn on the index finger as an extra retentive tool since the pollex stump was very small. But due to problems like open margin and dislodgement of the prosthesis during movement of the residual stump or finger, the wire was cut and detached from the ring. Also, disadvantages such as show through of wire, susceptibility of silicone to tear from the portion where wire was emerging and difference in flexibility of the two materials, were expected with the prosthesis if the wire was retained. In the present case, since the disadvantages of using a wire to aid in mechanical retention was more, so medical adhesives were used to retain the prosthesis. Kapandji score was used as an assessment tool for evaluation of the functional movement and results with a good range of movement, without dislodgement were seen. This was achieved without any extra retentive element on the residual pollex stump of very small size.
[1]. Kapandji A, Clinical test of apposition and counter-apposition of the thumbAnn Chir Main 1986 5:67-73.10.1016/S0753-9053(86)80053-9 [Google Scholar] [CrossRef]
[2]. Bueno RA, Gellman H, Thumb reconstructionMedscape [Online] 2018 https://emedicine.medscape.com/article/1244563-overview [Google Scholar]
[3]. Shanmuganathan N, Maheswari MU, Anandkumar V, Padmanabhan TV, Swarup S, Jibran AH, Aesthetic finger prosthesisThe Journal of Indian Prosthodont Soc 2011 11:23210.1007/s13191-011-0074-923204732 [Google Scholar] [CrossRef] [PubMed]
[4]. Dhole R, Srivatsa G, Shetty R, Nandini Y, Sudhakar A, Thumb prosthesis-simplified approach: A case reportJ Dent Orofac Res 2014 10:21-24. [Google Scholar]
[5]. Cervelli V, Bottini DJ, Arpino A, Grimaldi M, Rogliani M, Gentile P, Bone anchored implant in cosmetic finger reconstructionAnn Chir Plast Esthet 2008 53:365-67.10.1016/j.anplas.2007.06.01018031918 [Google Scholar] [CrossRef] [PubMed]
[6]. Heitmann C, Levin S, Alternatives to thumb replantationPlast Reconstr Surg 2002 110:1492-503.10.1097/01.PRS.0000029362.01985.8012409769 [Google Scholar] [CrossRef] [PubMed]
[7]. Doppen P, Solomons M, Kritzinger S, Osseointegrated finger prosthesesJ Hand Surg Eur 2009 34:29-34.10.1177/175319340809380719091736 [Google Scholar] [CrossRef] [PubMed]
[8]. Agrawal KK, Aggarawal H, Singh K, Prosthetic rehabilitation of amputated thumb: a simplified approachJ Indian Prosthodont Soc 2014 14(Suppl 1):260-63.10.1007/s13191-013-0314-226199527 [Google Scholar] [CrossRef] [PubMed]