Prostatic cancer is the second commonest cancer in the world and the sixth commonest cause of cancer related mortality in men [1]. In India the Age Adjusted Incidence Rate (AAR) of prostatic cancer per one lac population of males varies in relation to geographical areas. It was 12.4 in Delhi area, 9.8 in Mumbai area, 6.7 in Chennai area and 8.2 in Bangalore area. The lowest AAR of 1.0 was noted in Tripura area [2]. Prostatic carcinoma is characterised by presence of crowded glands with haphazard growth oriented perpendicular to each other. Small atypical glands present between smooth muscle bundles and benign large glands represent infiltrative growth. Loss of glandular differentiation leads to formation of cribriform pattern, fused glands, solid sheets, cords and singly infiltrating cells. Circumferential perineural invasion, micro nodular formation and glomerulations with or without comedonecrosis are specific features of cancer. Cytologically presence of intraluminal crystalloids, amphophilic cytoplasm, nuclear enlargement and nucleoli are malignant features. One of the major criterias for cancerous glands is the absence of basal cell layer in the acini.
On routine H&E sections, the basal cell layer is hardly obvious. Cancer glands may show cells that mimic basal cells, which are actually fibroblasts hugging the glands. In atrophic foci, adenosis and High-grade Prostatic Intraepithelial Neoplasia (HGPIN), the basal cell layer is discontinuous and patchy [3].
A malignant diagnosis is difficult when suspicious small glands are focal or at the tip of the biopsy without showing cytological atypia. Presence of inflammation obscures the visualisation of basal cells in such cases. These situations prove to be a diagnostic dilemma for the pathologist. Bostwick DG et al., defined these lesions as Atypical Small Acinar Proliferation (ASAP) [4]. They proposed the following criteria for the diagnosis of ASAP. The focus should be smaller than 0.4 mm in diameter containing less than 24 acini showing clustered growth pattern, distorted acini, lack of nucleomegaly, loss of the focus on subsequent sections, patchy basal cell layer on IHC and negative p504s staining. They recommended re-biopsy for such lesions. Presence of such small foci mandates demonstration of basal cell layer with p63 or HMWCK for a definitive diagnosis.
This study was aimed at determining the efficacy of using p63 immunomarker alone to resolve suspicious foci in prostate biopsies as compared to using p63, HMWCK and p504s together. The main drawback of using p63 is the lack of a positive signal in cases of carcinoma. However, it is the most defining feature of carcinoma. A single marker instead of three is a very much viable option in situations like small focus of suspicion and economical constraints. There are many studies which have used p63, HMWCK and p504s individually and together as a cocktail in prostate biopsies. This study is innovative as we have compared the utility of p63 alone against the opinion derived from using three markers.
Materials and Methods
Thirty prostate needle biopsies which contained suspicious foci on histomorphology were selected for this study out of 664 prostatic specimens received in our department during the period of January 2014 to July 2016. Relevant clinical details and Prostate-Specific Antigen (PSA) levels were collected from the medical records department and documented. Institutional ethics committee clearance was obtained prior to onset of study.
Immunohistochemistry with p63, HMWCK and p504s was performed on the sections containing the suspicious foci by Polymer labeling 2-step method using super sensitive polymer-HRP (horseradish peroxidase), IHC detection system with Diamino-Benzidine (DAB) chromogen. Appropriate benign and malignant controls were also run simultaneously. The final diagnosis was given after correlating morphology and three IHC markers. The foci which had continuous p63 and HMWCK positivity with negative p504s was diagnosed as benign prostatic tissue.
The cases with discontinuous basal cell layer and positive p504s were labelled as HGPIN. The cases with glands showing no staining with p63 and HMWCK in the basal pattern and positive staining with p504s were given the diagnosis of carcinoma. The positive p504s was interpreted in comparison with the benign glands. The number of cases with benign diagnosis was 24 and six cases were diagnosed as carcinoma. The final diagnosis obtained by this method was taken as the gold standard.
The H&E slides and only p63 slides were then reviewed by two independent pathologists who were blinded to the above findings and were asked to provide a diagnosis based on the morphology and basal cell layer as depicted by p63. Their diagnoses were recorded and compared to the gold standard diagnosis. Statistical analysis was done using SPSS software to calculate sensitivity and specificity of p63. Cohen’s Kappa was used to evaluate interobserver agreement.
Results
The age range of patients in this study was 49 to 88 years. PSA levels ranged from 2.42 to 59.29 ng/mL. The final diagnosis achieved by using p63, HMWCK, and p504s was benign in 24 cases, and adenocarcinoma in six cases. There was agreement of diagnosis in 30 (100%) cases with pathologist 1 and in 29 (97%) cases with pathologist 2. There was significant agreement with the final diagnosis that was achieved using three IHC markers to the diagnosis achieved by using p63 alone. There was also significant reproducibility in the diagnosis between the two independent pathologists. The comparison of diagnosis is tabulated in [Table/Fig-1].
Comparison of diagnosis achieved by using three markers to that obtained by using p63 alone.
| Diagnosis | Using H&E, p63, HMWCK and p504s | Pathologist 1 using H&E and only p63 | Pathologist 2 using H&E and only p63 |
|---|
| Benign | 24 | 24 | 23 |
| Adenocarcinoma | 6 | 6 | 7 |
p63 had 100% sensitivity and specificity in diagnosing adenocarcinoma with pathologist 1. With pathologist 2 it had sensitivity of (6/6) 100% and specificity of (23/24) 95.83%. Cohen’s kappa value was 0.902 (kappa value ranges from 0 to 1, 0.8-0.9 is taken as indication for strong agreement) for interobserver agreement between the two pathologists which indicated statistically significant agreement between them. The comparison between the diagnosis rendered by using three markers and by using p63 alone is tabulated in [Table/Fig-1].
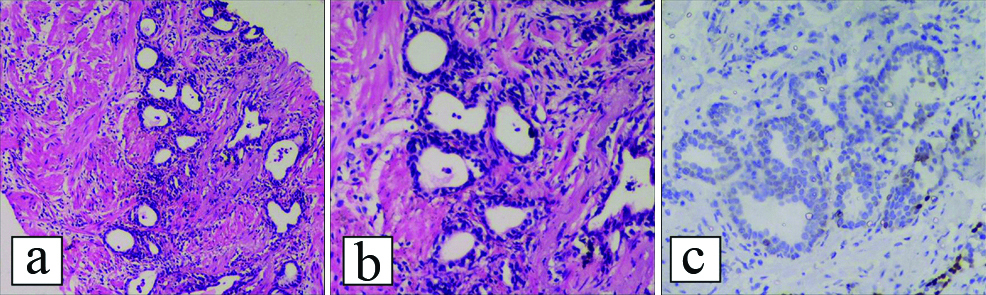
[Table/Fig-2] shows the case in which there was a difference of opinion was due to patchy and light p63 stain in the basal cell layer of the glands. There was continuous circumferential stain with HMWCK and negative p504s stain in that particular focus. The second pathologist interpreted it as absence of basal cell layer and gave a diagnosis of carcinoma.
Case in which there was a disparity in diagnosis: (a) suspicious focus composed of crowded glands with sharp luminal border and hyperchromatic lining cells (x40); (b) (x200); (c) p63 IHC showed faint patchy staining.
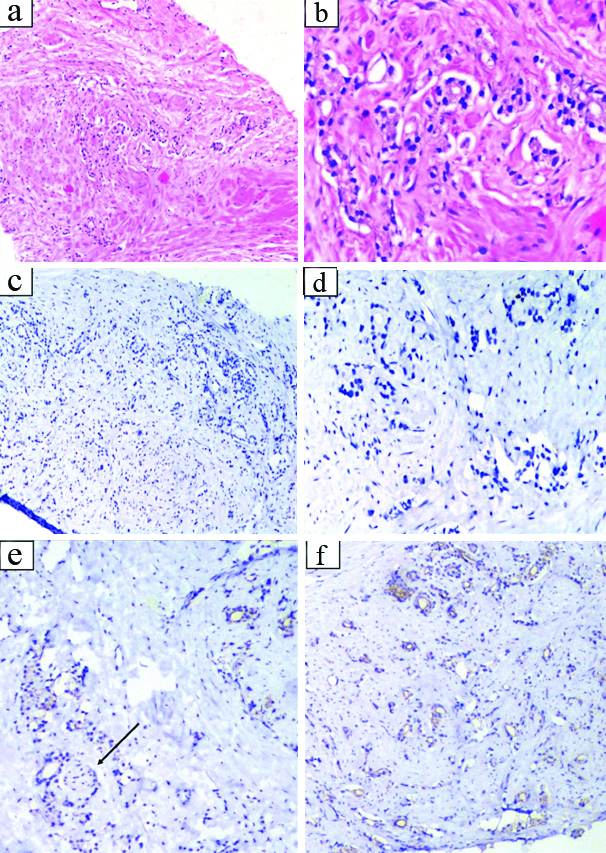
[Table/Fig-3] shows biopsy of a 65-year-old gentleman with a focus of ASAP. It proved to be benign on IHC. In this case, the appearance was suspicious because of atrophic glands appearing to have a single layer of epithelium with hyperchromatic nuclei.
Biopsy of 65-year-old man with raised serum PSA showing atypical small suspicious glandular proliferation: a) Crowded small atypical glands measuring less than 0.4 mm (x40); b) (x200). The size of the focus corresponds to ASAP diagnostic criterion; c) p63 stained the inconspicuous basal cells in all the suspicious glands (x200); d) Higher magnification of p63 IHC (x400).
[Table/Fig-4] shows a prostate needle biopsy which had a focus of limited carcinoma. Epstein JI defined limited carcinoma as cancer involving less than three cores without grade 4 or grade 5 component and that involving less than half of the tissue of the cores [5]. The basal cell markers were negative in those glands. p504s was positive in them highlighting the lumina.
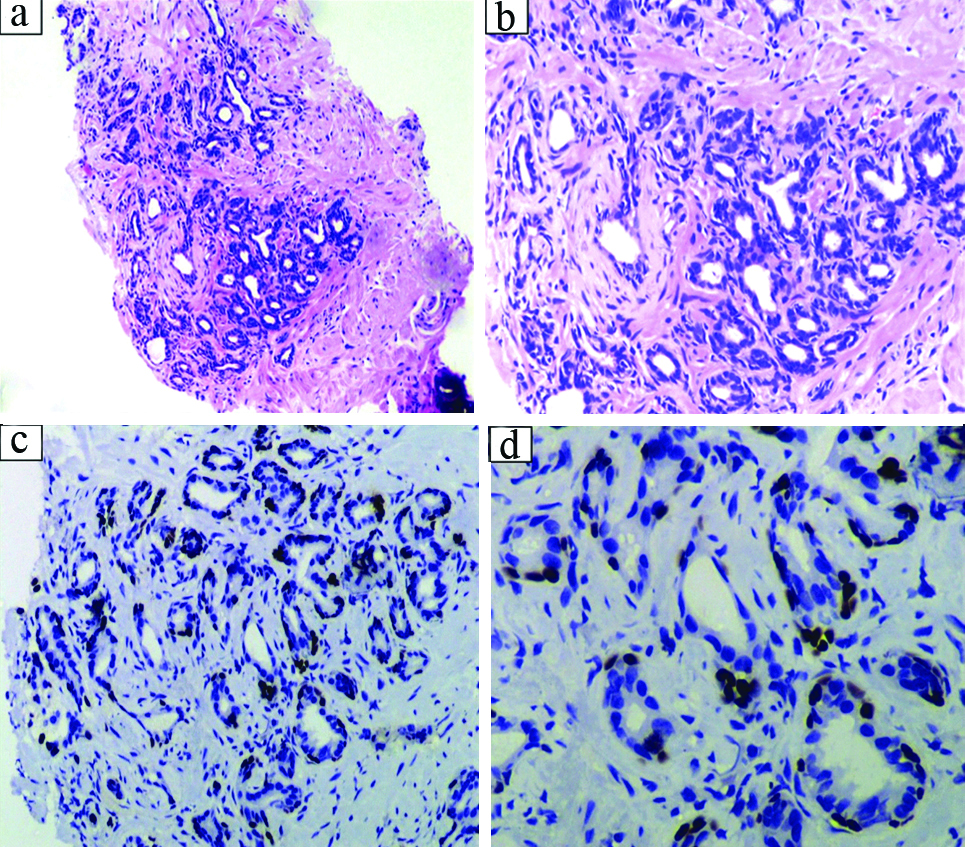
Negative p63 stain in a limited carcinoma (only two cores were involved out of 10. No Gleason pattern 4 or 5 was seen. Less than 10% of the cores were involved): a) suspicious small glands infiltrating the muscle bundles (x40); b) (x200); c) Absence of HMWCK staining in the suspicious glands (x100); d) Absence of p63 staining in the suspicious glands (x200); e) Positive p504s in the suspicious glands. Arrow indicating perineural invasion (x100); f) Positive p504s in the suspicious glands (x100).
Discussion
The advent of PSA as a screening test for prostate cancer led to an increase in the number of biopsies performed in cases with high clinical suspicion. The biopsy technique has evolved to mapping biopsy guided by trans-rectal ultrasound resulting in more number of cores (up to 12) being submitted for histopathological examination.
The challenge of diagnosing biopsies harboring minute foci of suspicious lesions and under sampled cancer is being faced more often. The uncertainty on the part of pathologist has led to the introduction of newer diagnostic categories such as ASAP and limited cancer. Many pointers are given by established uropathologists for the diagnosis of prostate cancer. The major criteria to be considered are architectural features such as infiltrative growth and presence of irregular spacing between glands when compared to benign glands. Absence of basal cells in the suspicious glands is a major criterion for diagnosing cancer. Cytological features such as presence of amphophilic cytoplasm, nuclear atypia and enlarged nucleoli are specific for cancer. Other features such as perineural invasion, glomerulations inside the glands and formation of micronodules of collagen are specific for cancer. When in doubt the comparision between benign glands for architectural and cytologic features will solve the issue [6]. Recognition of basal layer only by H&E stain is sometimes difficult and prone to errors. Immunohistochemistry is being employed more often to arrive at the final diagnosis. Absence of basal cells on IHC is a major criteria for diagnosing cancer [7]. p63 and HMWCK are used for this purpose. Various factors like method of antigen retrieval and method of IHC affect these two antibodies. Some authors opine that p63 is slightly better than HMWCK. Latest guidelines for IHC in prostate carcinoma given by International Society of Urological Pathology (ISUP) recommend that IHC is not needed in obvious cases of carcinoma and cases with benign glands. They recommend a combination of p63, HMWCK and p504s to be done in suspicious cases. They recommend that a cocktail of these three antibodies with different chromogens to be used to conserve tissue and the suspicious focus [8]. But in the current scenario these triple cocktails are neither widely available nor cost effective. So a step wise approach to the biopsies is preferable by selecting the best marker to be done first. This is to avoid the issue of loss of tissue containing the focus of interest.
p63 gave reliable results in all the cases in our centre. p63 is also a more frequently used marker than HMWCK as it is utilised in neoplasia of other organ systems also.
Many mimickers of prostatic cancer are seen in routine practice. IHC with p63 can resolve most of them. Atrophy, partial atrophy, adenosis, sclerosing adenosis, basal cell hyperplasia and clear cell cribriform hyperplasia can be resolved by using p63. Benign tissue like seminal vesicle and Cowper’s glands also can be highlighted by p63 IHC when they cause confusion. Using p504s in this setting can cause confusion because it is focally positive in some cases of atrophy and adenosis. Nephrogenic adenoma and mesonephric remnant hyperplasia are two rare lesions but can be a potential pitfall for misdiagnosis of carcinoma. These lesions are negative for p63 and can show p504s positivity causing confusion. Nephrogenic adenoma shows PAX8 positivity. PAS stain will show thickened hyaline lining around the glands. Mesonephric remnant hyperplasia typically occurs in periurethral region and not in the periphery. It is also positive for PAX8. These two lesions are seen in Transurethral Resection of Prostate (TURP) specimens more commonly than prostate biopsies [9].
Weinstein MH et al., studied p63 IHC in 70 prostatic specimens with HMWCK as gold standard. They have found p63 was as effective as HMWCK and was informative in 55 specimens to reach a final diagnosis. p63 expression was informative in 93% of IHC where charged slides were used and in 75% where uncharged slides were used after de-staining H&E sections [10].
In the Indian scenario, the middle ground approach of ASAP is not always possible because of the cost and patient incompliance for a repeat biopsy. The reporting pathologist is asked for a report which needs to be benign or malignant.
The problem is further complicated by loss of the focus of interest on sectioning because of excessive trimming. This can be solved by leaving one unstained section for every block that is cut for IHC purpose [11]. This approach is not feasible in most of the labs with high workload because slides used for routine H&E sections are coated by egg albumin-glycerol mixture and those used for IHC are charged polylysine coated slides which need special preparation technique amounting to higher processing cost per biopsy. Hameed O et al., compared utility of performing IHC on interval sections cut on uncharged slides to that of using recut sections [12]. Only 55% of cases on which IHC was done on uncharged slides showed identical results to that of re-cut sections on charged slides. Another approach is to use an antibody cocktail. Molinie V et al., were able to resolve the doubt in 93% of the suspicious lesions using an antibody cocktail comprising of p63 and p504s [13]. This method has drawbacks related to interpretation of staining where a single colour chromogen is used. There can be confusion in cases such as carcinoma over expressing p63 and in cases with background staining due to faulty processing and IHC technique. Use of dual colour chromogens with two separate secondary antibodies is expensive [14,15]. The conversion rate of suspicious lesions to carcinoma after performing IHC is relatively low as demonstrated by some studies. Most suspicious lesions prove to be benign. In a study by Molinie V et al., out of 109 cases of suspicious lesions, 23 cases were given the final diagnosis of carcinoma after performing IHC with p63 and p504s [16]. In our study out of 30 suspicious cases 24 cases were proved to be benign and 6 cases as carcinoma after IHC.
p63 has demonstrated much reliability in diagnosing prostate cancer in many previous studies. Zhou M et al., studied the expression of p63 and HMWCK as a cocktail, as well as separately in nine cases of benign prostatic hyperplasia and a tissue microarray of 103 cases of localised prostate cancer [17]. All cases with benign glands (98%) stained positively with p63. The positivity however varied between the cases. In about 0.3% of carcinoma cases showed patchy positivity. The authors believe the positivity in these glands might have been due to entrapped basal cells. They concluded that aberrant expression of basal markers may occur in poorly differentiated cancers.
Shah RB et al., performed p63 and HMWCK on 25 needle biopsies (NBX), two TURPs containing atypical foci, 55 needle biopsies with confirmed cancer and 12 total prostatectomies removed for benign prostatic hyperplasia [18]. In all the adenocarcinoma cases, none of the malignant glands showed positivity for p63. Ninety one percent of all needle biopsies and 95% of TURPs diagnosed as benign, showed complete positivity with p63 in a basal distribution. The comparison between these previous studies and the present study is depicted in [Table/Fig-5]. p63 positive prostate carcinoma is a rare variant which is described in the literature. This particular variant has the architectural features of carcinoma but shows p63 positivity in the nuclei of the cells lining the cancer glands. This variant though very rare when present could be a potential pitfall and can lead to misdiagnosis of carcinoma as benign glands. In this variant, though p63 is positive in the glands, HMWCK is negative and p504s is positive. In benign glands, the p63 positivity is seen in a basal pattern whereas p63 positive prostate cancer shows nuclear positivity in the cells lining the glands. Attention to the morphology and IHC pattern is required to correctly diagnose this variant. The evaluating pathologist must be aware of this pitfall when using p63 alone [19].
Comparison between previous studies on p63 and the present study.
| P63 positivity in | Weinstein MH et al., [10] | Zhou M et al., [17] | Shah RB et al., [18] | Present study |
|---|
| Benign cases | 100% | 98% | 91%of NBX, 95% of TURP | 100% |
| Adenocarcinoma | 0% | 0.3% | 0% | 0% |
Where some specimens are from economically backward patients, performing two to three immunomarkers may prove economically nonviable. If only one basal cell marker (p63) can be used for arriving at the diagnosis, issues of cost efficiency and loss of focus of interest can be resolved efficiently. In those cases where the ambiguity persists after p63 staining, p504s and HMWCK IHC may be resorted to for confirmation.
Limitation
As in this study, there were only six cases out of thirty, of adenocarcinoma, so we could not compare between utility of p63 in benign and malignant prostrate biopsies.
Conclusion
We conclude that using p63 alone, we can resolve suspicious prostate biopsies with reliable accuracy. The good performance of this IHC marker in this aspect is well documented in literature as well as in our experience. The most recent best practices suggested by uropathology experts state that IHC should be resorted to in only suspicious cases. Our recommendation is that when the focus of interest is very small, especially in biopsies, p63 should be used first to document the presence or absence of basal cells.