Ultrasound Elastography is the novel, non-invasive imaging modality, which upon its invention in late 19th century, has gained various clinical advantages. Elastography is an Ultrasonographic (USG) analogue of manual palpation, based on the principle that pathology changes the stiffness of the tissue [1]. Two methods have been devised to study this phenomenon. They are strain elastography which is based on tissue deformation due to external compression and shear wave elastography which is based on the propagation of acoustic shear waves through the tissues which causes deformation.
Thyroid lesions are one among the commonly encountered radiological finding in our day to day practice as they are increasingly diagnosed with greater awareness among the population. Though there have been a diverse clinical and radiological findings depicted to differentiate benign and malignant thyroid lesions but altogether fails to satisfactorily differentiate the lesions as benign or malignant [2]. Ultrasound elastography, also known as “Electronic palpation imaging” is a promising, newly developed non-invasive imaging modality, which has emerged as a recent advancement in ultrasonography. Elastography was first developed by Ophir J et al., at the University of Texas Medical School [1]. This technique helps in assessment of stiffness by measuring the degree of distortion under external force application. This technique is used to detect relative tissue stiffness or displacement (strain) in response to applied force. Stiff tissues deform less and exhibit less strain than compliant tissues when same force is applied. Thus, the basis of elastography is analogous to manual palpation. This technique shows that malignant lesions appear to be stiffer when compared to benign lesions [3]. By applying this principle, we evaluated the diagnostic performance of ultrasound elastography in characterising thyroid lesions as benign/malignant and its correlation with FNAC/biopsy results.
Materials and Methods
This prospective diagnostic study was performed after obtaining Institutional Ethical Committee approval IEC REF No: IEC: RC/14/58. This study was conducted in Department of Radio-Diagnosis at Pondicherry Institute of Medical Sciences on 88 thyroid lesions in 86 patients between October 2014 and April 2016 after explaining the method of diagnostic procedure and informed written consent was obtained. The inclusion criteria include all patients with clinically palpable thyroid lesions, equal to or above 20 years of age and exclusion include patients presenting with features of retrosternal goiter and post-thyroidectomy patients. The radiologists involved in this study received training on Elastography from SIEMENS application staff and practiced recording images prior to the study.
Examination Protocol
Routine Ultrasonography was performed in these patients with 9L4 (4-9MHz) linear high frequency transducer on SIEMENS ACUSON S 2000 ultrasound machine. Grey scale imaging was first done and the lesions were also evaluated using Colour Doppler. The cervical lymph node chain was also evaluated for any nodal enlargement and the findings were documented. After identifying the thyroid lesions on grey scale, elastography was performed using Elasticity tissue imaging technique and Acoustic Radiation Force Impulse (ARFI) technique.
Strain Elastography Technique
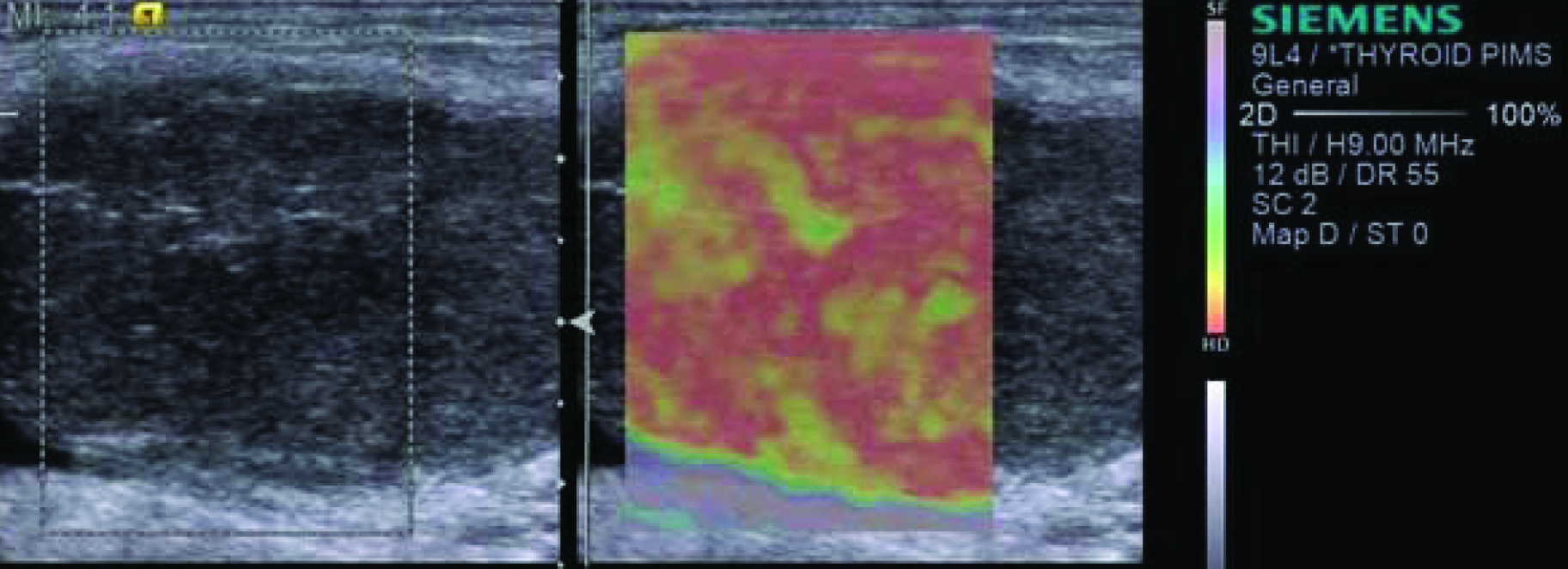
Elastography scores were first assessed using elasticity imaging technique. The probe was placed on the neck with light pressure and the patients were asked not to swallow their saliva to avoid motion artifacts due to swallowing and a box is highlighted, which included the lesion and part of surrounding thyroid tissue. The application displayed a real-time Quality Factor (QF) score by using advanced signal-intensity analysis. A high QF value indicated minimal global motion artifacts and a low QF value indicated global motion artifacts that may decrease diagnostic value [4]. Hence, by keeping the probe stationary for about 5-10 seconds, QF of about 45-50 or more was applied to assess the scores of the lesions [5]. The USE (ultrasound elastogram) was displayed next to the B-mode image and the maximum score was evaluated [6]. The colour mapping of the elastography score in our study was classified from purple, indicating a great amount of elasticity (soft component) to red, indicating lack of elasticity (rigid component). After obtaining the elastogram colour image, the lesions were scored based on Ei-Ueno classification scoring system and the images were saved for future references [6-8]. The above technique is illustrated as shown in [Table/Fig-1].
Technique of elasticity imaging in a 77 years old female with a lesion of EI score of 4 in the right lobe of thyroid which was proved to be papillary carcinoma on FNAC.
Shear Wave Elastograhy Technique
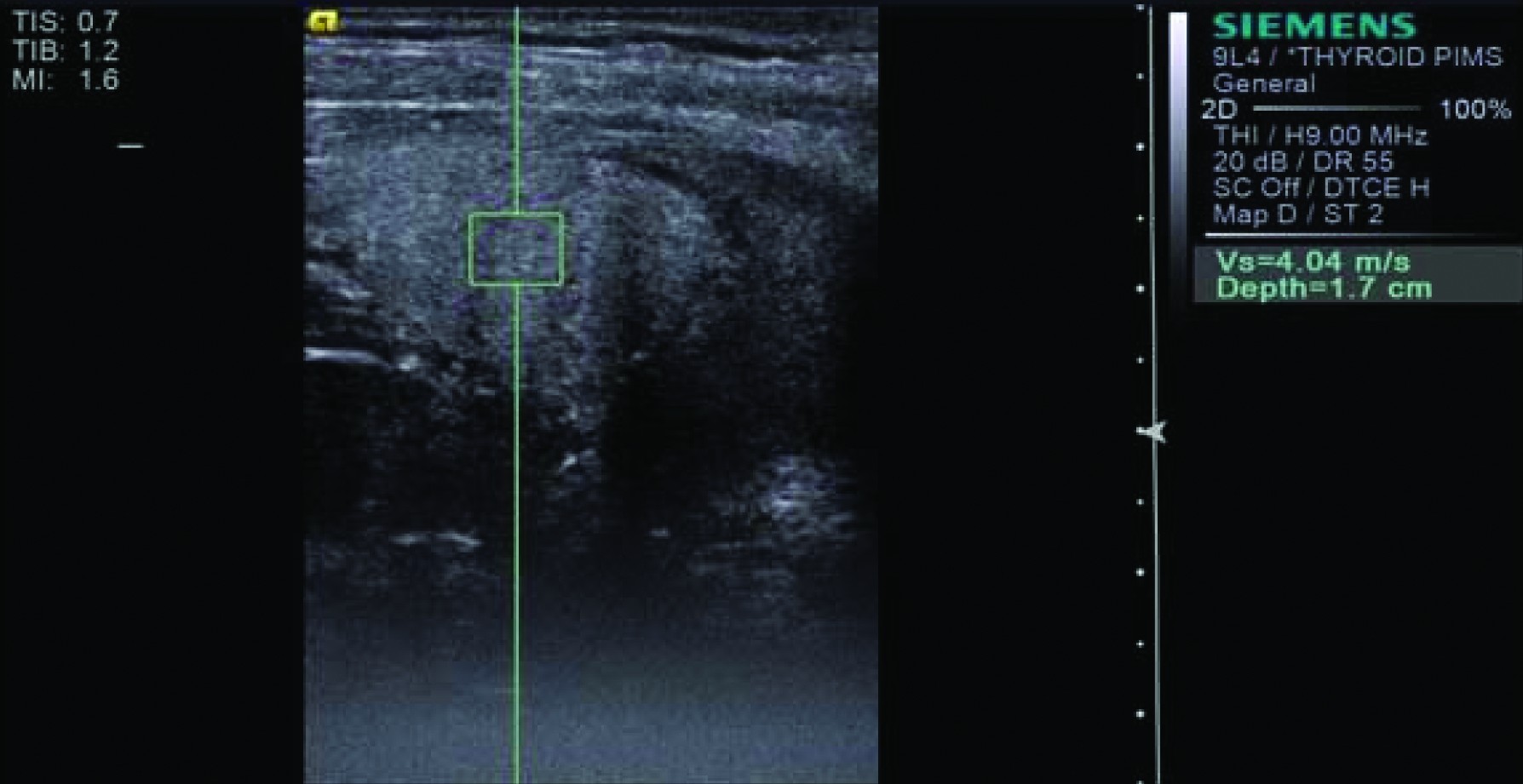
Virtual Touch Tissue Quantification (VTTQ) parameter was evaluated by ARFI technique in our study. After assessing the lesion based on elastography scores, VTTQ was performed. On performing VTTQ, the tissue within the Region Of Interest (ROI) identified on B-mode was excited mechanically using acoustic pulses for a short duration (<1 ms) in turn producing localised displacement of the tissue without any external compression. Localised tissue displacement will generate acoustic Shear Waves (SW). Value of this function represents the Shear wave velocity (m/s) which is the measure of peak displacement. Shear wave velocity is directly proportional to the tissue stiffness. The probe was placed gently over the body surface under light pressure on thyroid and patients were asked to hold their breath and not to swallow their saliva to avoid motion artifacts due to swallowing and respiratory movement artifacts. ROI was placed over the solid portion of the lesion and in this technique adjacent thyroid tissue was not included [9]. This technique is illustrated in [Table/Fig-2]. After selecting ROI, ARFI measurement was activated and the SWV (Shear Wave Velocity) value was displayed on the screen. The range for the SWV is 0-9 m/s. The VTTQ values were taken five times in each lesion and mean value was selected as SWV value of the nodule [10,11]. Values beyond these ranges were displayed as “X.XX m/s”. In other words, both extremely hard and soft tissue can be shown as “X.XX m/s”. After excluding the possible influencing factors such as patient’s respiration and operator’s inappropriate gesture, VTTQ measurement of “X.XX m/s” was replaced by values of 9 m/s or 0 m/s, with the value of 9 m/s corresponding to the solid portion and 0 m/s corresponding to the cystic portion respectively [5,12,13].
Technique of shear wave elastography imaging in a 70 years old female with a lession in left lobe of thyroid which was proved to be anaplastic carcinoma on FNAC.
Histopathological Correlation
FNAC was done later in patients identified with thyroid lesions and biopsy was done only if FNAC was positive for malignancy or if the lesion was surgically removed. Ultrasound elastography scores and SWV values were then correlated with FNAC or biopsy results as gold standard in the same patients. Biopsy results were taken into account for patients who underwent thyroidectomy, irrespective of FNAC diagnosis as biopsy results are gold standard as when compared to FNAC in evaluation of thyroid lesions [14].
Statistical Analysis
The data was entered in Microsoft Excel 2010 and analysed using SPSS 20.0 version software. The clinical characteristics of the study patients were described using mean and standard deviation for continuous variables and percentages for categorical variables. A p-value <0.05 is considered significant. ROC curve analysis was done for elasticity imaging scores and shear wave velocity values to find sensitivity and specificity of ultrasound elastography in differentiating benign and malignant lesions. False positive rate, false negative rate and accuracy rate were also calculated. Areas under ROC curves were calculated and best cut-off values and 95% confidence intervals were estimated.
Results
In this prospective diagnostic study, we evaluated 86 patients, most of the patients belonged to the age group of 36-45 years (28%). The demographic data of our study is illustrated in [Table/Fig-3]. The distribution of pathological diagnosis of the lesions included in our study is depicted in [Table/Fig-4]. Out of 88 lesions, 15 lesions (17%) were found to be malignant on FNAC or Biopsy. A total of 73 lesions (83%) were found to be benign on FNAC or Biopsy.
Demographic data- Distribution of subjects according to age group (in years).
| Age Group | Number of Case | Percentage |
|---|
| 0-25 | 5 | 6 |
| 26-35 | 17 | 20 |
| 36-45 | 24 | 28 |
| 46-55 | 20 | 23 |
| 56-65 | 15 | 17 |
| >66 | 5 | 6 |
| Total | 86 | 100% |
Total number of thyriod lesions diagnosed by FNAC or Biopsy in our study.
| FNAC / Biopsy Diagnosis | No of Lesions | Percentage |
|---|
| Goitre | 46 | 52.3% |
| Autoimmune Thyroiditis | 25 | 28.4% |
| Follicular Adenoma | 2 | 2.3% |
| Papillary CA | 6 | 6.8% |
| Follicular Variant of Papillary CA | 3 | 3.4% |
| Follicular CA | 3 | 3.4% |
| Medullary CA | 1 | 1.1% |
| Anaplastic CA | 2 | 2.3% |
| Total | 88 | 100% |
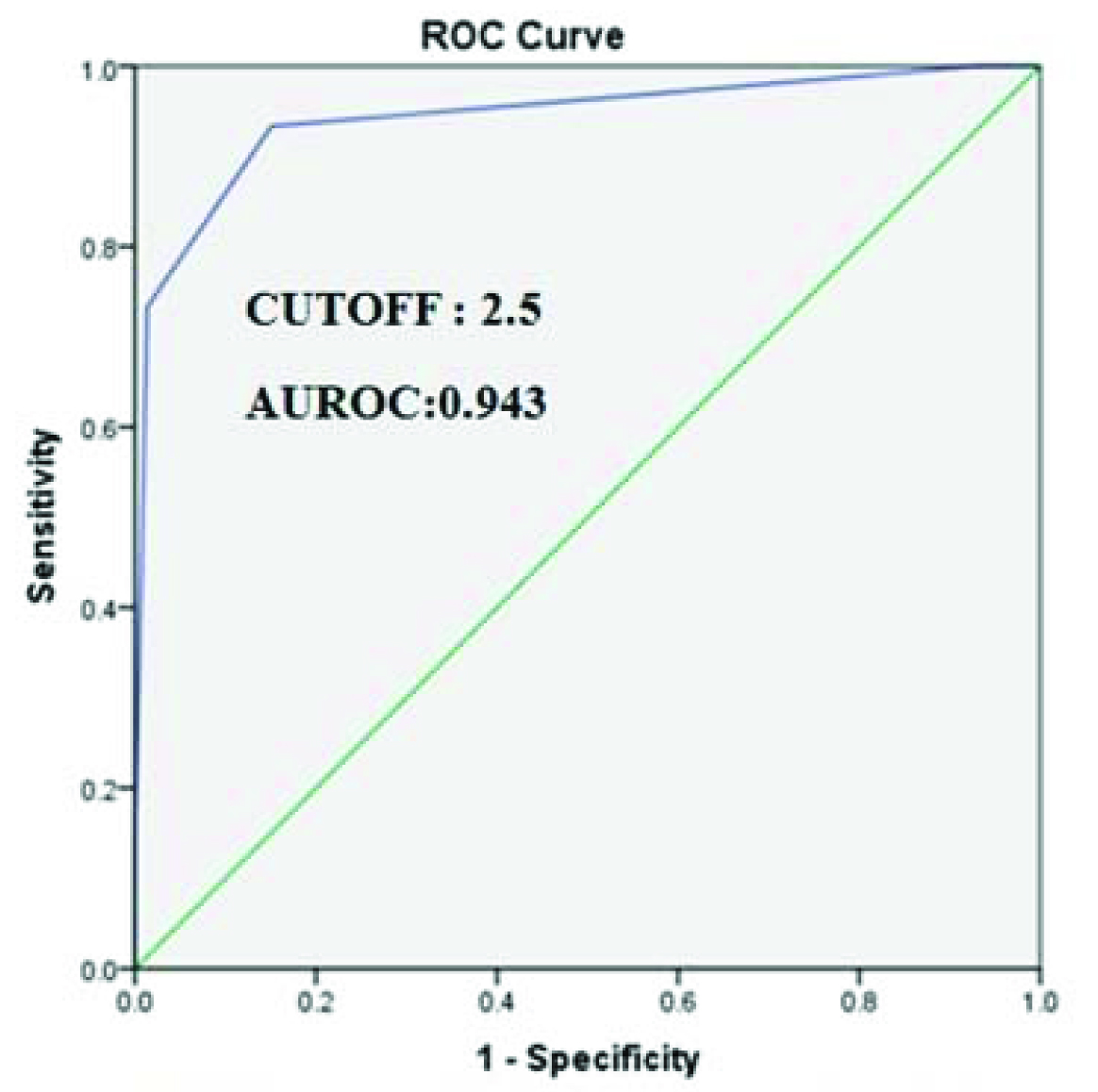
Comparison between EI scores and FNAC or Biopsy results: Out of 88 thyroid lesions, 5 lesions had Elasticity Imaging (EI) score of 1 (5 were benign and no malignant lesions), 58 lesions had EI score of 2 (57 were benign and 1 was malignant), 13 lesions had EI score of 3 (10 were benign and 3 were malignant), 10 lesions had EI score of 4 (9 were malignant and 1 was benign) and 2 lesions had EI score of 5 (2 were malignant and no benign lesions). ROC curve analysis was performed for EI scores and showed that area under the curve for EI was 0.943 (95% confidence interval: 0.87-1.0) and p-value <0.001 and was statistically significant. The best cut-off point for EI scores was 2.5, which means scores 1 and 2 are benign and scores 3, 4 and 5 are malignant as shown in [Table/Fig-5].
ROC curve analysis for Elasticity Imaging (EI) scores.
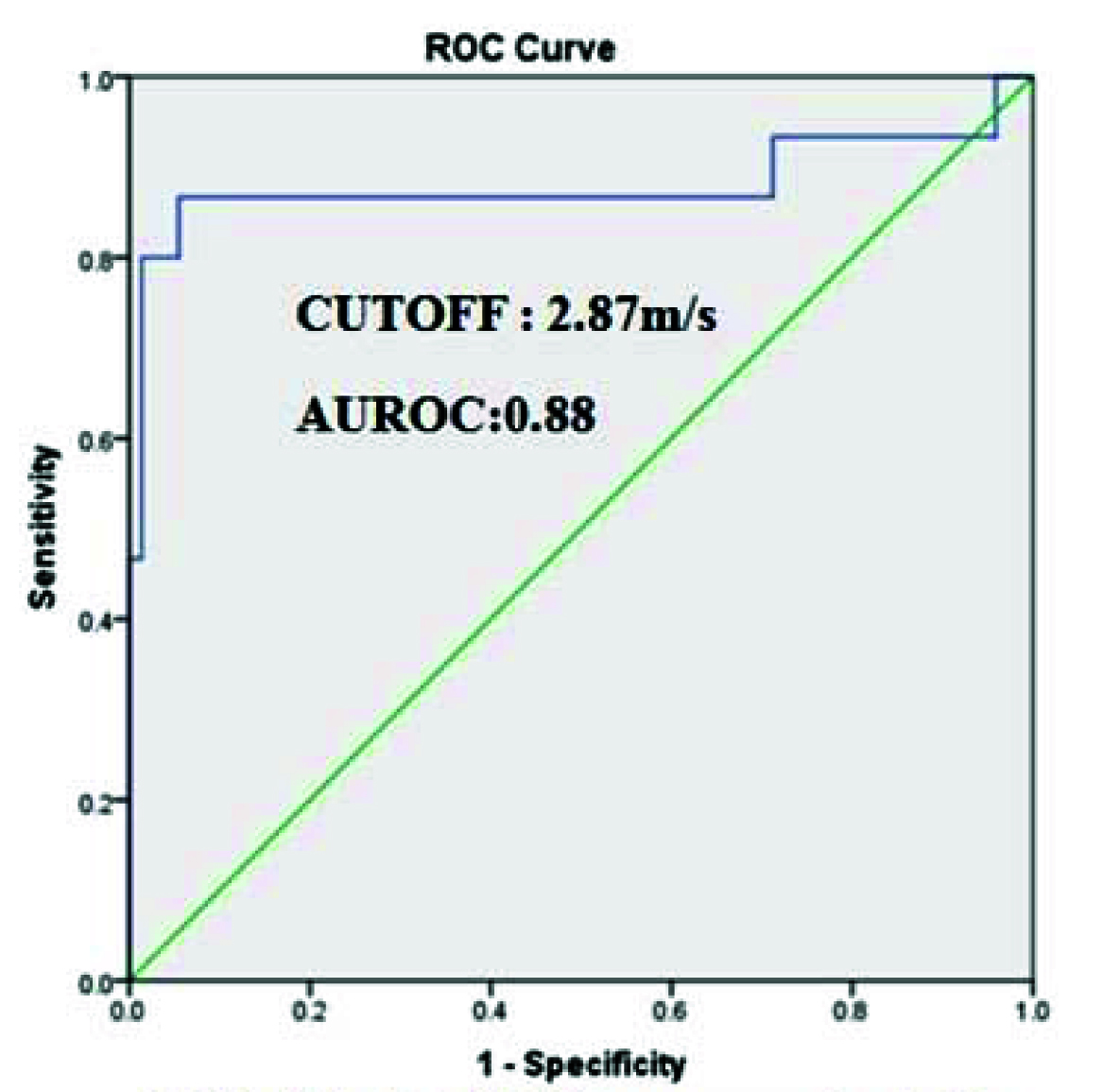
Comparison between SWV values and FNAC or Biopsy results: ROC curve analysis was performed for SWV values and showed that area under the curve for SWV value was 0.88 (95% confidence interval: 0.735-1.000) and p<0.001 and was statistically significant. The best cut-off point for SWV values in differentiating between benign and malignant thyroid lesions was 2.87 m/s, which means SWV ≤2.87 m/s are benign and SWV ≥2.88 m/s are malignant as shown in [Table/Fig-6].
ROC curve analysis for SWV (ARFI-VTTQ) values.
The sensitivity, specificity, PPV, NPV, accuracy, false positive rate, false negative rate, positive and negative likelihood ratios of EI scores and SWV values were illustrated in [Table/Fig-7].
Comparison of sensitivity, specificity, positive predictive value (PPV), nagative predictive value (NPV), accuracy, positive likelihood ratio and negative likelihood ratio between elasticity imaging (EI) scores and SWV (AREI- VTTQ) values.
| Parameters | Elasticity Imaginic (EI) Scores | SWV (ARFI-VTTQ) value |
|---|
| Specificity | 93.3% | 86.7% |
| Specificity | 84.9% | 94.5% |
| PPV | 56.0% | 76.5% |
| NPV | 98.4% | 97.2% |
| Accuracy | 86.4% | 93.2% |
| False Positive Rate | 15.1% | 5.5% |
| False Negative Rate | 7.0% | 13.3% |
| Positive Likelihood Ratio | 6.19% | 15.76 |
| Negative Likelihood Ratio | 0.08% | 0.14 |
Discussion
Various studies showed that papillary carcinoma is the most common thyroid malignancy [15,16]. In this study, we were able to supplement the statistical data with nine lesions of papillary carcinoma (60%) including its follicular variant, out of 15 malignant lesions.
Previous study by Eltyib HEH et al., performed ultrasound elastography scoring to differentiate between benign and malignant thyroid lesions. Elastography scores of 1 and 2 were found in 47 cases and were diagnosed as benign lesions on FNAC. A score of 3 was found in 12 cases, of which 2 were malignant and were reported as follicular carcinomas. Scores of 4 and 5 were found in 19 cases. Among them, 13 were malignant and 6 were benign. This study reported with sensitivity of 93.7%, specificity of 90%, PPV of 71%, NPV of 98% and accuracy of 91% [16]. Similar study by Abdelrahman SF et al., evaluated 73 thyroid lesions of indeterminate cytology with ultrasound elastography scores. Among them, 57 nodules were benign and 16 nodules were malignant. Among 57 benign nodules, 41 nodules had a score of 1 or 2 (15 nodules with a score of 1, and 26 nodules with a score of 2) and 16 nodules had a score of 3. Of the 16 malignant nodules, 15 had a score of 4 or 5 (8 nodules with a score of 4, and 7 nodules with a score of 5). Only 1 of the malignant lesions had a colour score of 3 which was histologically found to be follicular variant of papillary carcinoma. On ROC curve analysis, the best cut-off point of 2.31 was used. Thus, all 57 cases with a final diagnosis of benign nodule had a score of 1-3, while 15 of 16 malignant lesions had a score of 4-5, with a sensitivity of 93.3%, specificity of 100% and accuracy of 97.8%. The PPV and NPV were 54% and 98.2% respectively [17].
In contrary to these past studies, our findings show that out of 88 lesions studied, ROC curve analysis performed for EI scores depicted best cut-off point as 2.5 with highest area under the curve of 0.943. This furthur portrays that EI scores of 1 and 2 are benign and scores 3, 4 and 5 are malignant. In our study out of 88 lesions, 25 lesions had EI score of ≥3, of which 14 were malignant and 11 were benign. A total of 63 lesions had EI score of ≤2, of which 62 were benign and 1 was malignant. In our study, the false negative malignant lesion was follicular carcinoma with EI score of 2. Eleven lesions were false positive with EI score of ≥ 3. Among them, 9 were goitres with EI score of 3 and 1goitre with EI score of 4 and the other 1 lesion was autoimmune thyroiditis with EI score of 3.
Previous study by Ning CP et al., showed that the best cut-off point for SWV values to differentiate between benign and malignant thyroid lesions was 4.2 m/s. Area under the curve was 0.88. The sensitivity and specificity of ARFI-VTTQ was found to be 82.4% and 71.6% respectively [18]. Another similar prospective study by Wang H et al., which evaluated 168 thyroid nodules best cut-off point to differentiate between benign and malignant lesions was 3.85 m/s with area under the curve of 0.907. The sensitivity, specificity and accuracy was 80.7%, 91.4% and 88.1 % respectively [19]. Similar prospective research by Calvete AC et al., in the evaluation of SWV values of benign and malignant thyroid lesions using ARFI-VTTQ technique showed the best cut-off point for SWVs in their study to differentiate between benign and malignant thyroid lesions was 2.50 m/s with the sensitivity, specificity, PPV and NPV were 85.7%, 96.0%, 82.8% and 96.8% respectively [8].
In our study, we found that best cut-off value for differentiating between benign and malignant thyroid lesions was 2.87m/s. Out of 88 lesions, 17 lesions had SWV ≥ 2.88 m/s, of which13 were malignant and 4 were benign and 71 lesions had SWV ≤ 2.87 m/s, of which 2 were malignant and 69 were benign.
Our findings are consistent with previous studies done by Zhang YF et al., and Xu JM et al., on assessment of best cut-off point for SWV values in differentiation between benign and malignant thyroid lesions and the best cut-off point was 2.87 m/s [5,12].
In our study, out of 71 lesions with SWV values of ≤2.87 m/s, 69 lesions were benign and two lesions were false negative. Among these 2 false negative lesions, one lesion was follicular variant of papillary carcinoma and one lesion was follicular carcinoma. 17 lesions had SWV of ≥2.88 m/s, of which 13 lesions were malignant and four lesions were false positive. Among these four false positive lesions, two lesions were goitre and two lesions were autoimmune thyroiditis.
In our prospective study, the sensitivity and specificity analysis of EI scores and SWV (ARFI-VTTQ) values were compared with each other as shown in [Table/Fig-7]. EI scores had better sensitivity and NPV, as when compared to SWV values. SWV (ARFI-VTTQ) values had better specificity and PPV, as when compared to EI scores. Diagnostic accuracy was better with SWV values, as when compared to EI scores. Both parameters had good positive and negative likelihood ratios. EI technique is a qualitative analysis and images are assessed based on scoring and compression quality factor and there can be interobserver variability in this technique [4,20]. Various studies showed that ARFI-VTTQ technique is a quantitative method of imaging in ultrasound imaging and does not require compression, as “push-pulse” is generated by the machine itself and shear wave velocities are assessed [21-24]. In our opinion, by putting altogether, it was found that the Specificity was higher with SWV values than that of EI scores. PPV was higher with SWV values than that of EI scores. Diagnostic accuracy of SWV (ARFI-VTTQ) values were higher than that of EI scores.
Limitation
In our study, no correlation was studied between the grey scale ultrasound findings and FNAC or biopsy results. Elastography strain ratio and Virtual Touch Imaging (VTI), which are also the parameters in ultrasound elastography were not assessed in our study. In our study, only 15 lesions were proved to be malignant on FNAC or Biopsy. Hence, further studies with large number of patients will be required to ascertain the diagnostic accuracy of elastography in cases of follicular neoplasms, where the lesions may be soft in consistency and to distinguish them from benign lesions. Studies are also needed to assess whether this technique can be used to detect malignant lesions at an early stage for rapid management and to improve prognosis.
Conclusion
From our study, we strongly recommend Ultrasound Thyroid Elastography as a non-invasive imaging tool to aid in the vital process of differentiating benign and malignant thyroid lesions. ARFI-VTTQ technique has the high potential to detect benign lesions and can potentially reduce unnecessary FNAC procedures. It would further aid in follow up of lesions with indeterminate cytology on FNAC and managing them via follow-up observations. Elastography could be used as a non-invasive pre-FNAC triage tool in screening benign lesions with high level of confidence, although FNAC is a minimally invasive procedure that can take a toll on patients emotionally, especially in patients who have needle phobia.