Maintaining ‘V-Contour’ of the Neck after Surgery for Neglected Congenital Muscular Torticollis in an Adult (A New Technique)
Osama Neyaz1, Abhimanyu Vasudeva2, S L Yadav3
1 Senior Resident, Department of Physical Medicine and Rehabilitation, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
2 Senior Resident, Department of Physical Medicine and Rehabilitation, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
3 Professor, Department of Physical Medicine and Rehabilitation, All India Institute of Medical Sciences (AIIMS), New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhimanyu Vasudeva, A-1/124, Safdarjung Enclave, New Delhi-110029, India.
E-mail: abhimanyu.vmmc@gmail.com
In Congenital Muscular Torticollis (CMT), also called twisted neck or wryneck, an individual holds his or her head tilted to one side. There is a little consensus on the treatment approach of neglected CMT after skeletal maturity in adults. This case report describes a case of an 18-year-old male who presented with neglected CMT and was successfully managed using a novel surgical technique wherein after releasing the clavicular head of Sternocleidomastoid (SCM), proximal attachment was released while keeping the sternal head intact.
Sternocleidomastoid, Treatment outcome, Wryneck
Case Report
An 18-year-old, unmarried, male belonging to a rural area in Haryana attended the Outpatient Department (OPD) of a Government Hospital in Delhi in the month of March 2017, as a diagnosed case of right-sided CMT.
He was the first child of a nonconsanguineous marriage from a full-term vaginal delivery in a breech presentation. There was no family history of congenital deformities. He showed no other abnormalities. He was diagnosed with CMT in the first year of life. He was initially managed conservatively which included massage and stretching exercises of muscles of the neck. The deformity persisted and he was advised surgical correction at the age of 4 years by a local practitioner, but his parents continued with conservative management. Thereafter, at the age of 16 years, he consulted in a Government Hospital in Delhi due to peer pressure owing to aesthetic reasons where he was advised surgical correction; however, he was told that the prognosis may not be good at such a late age and, therefore, refused to undergo surgery. He subsequently visited the Department of Physical Medicine and Rehabilitation in the same Government Hospital at the age of 18 years where he eventually underwent surgery as he was counselled regarding the pros and cons of surgery. The head was tilted to the right with a mild rise of the ipsilateral shoulder and the projection of the chin to the left side. A shortened, prominent and band-like right Sternocleidomastoid (SCM) (Predominantly-Clavicular Head of the SCM) was noted [Table/Fig-1]. There was a limitation in rotation of the neck to the left side. Spine examination showed mild compensatory deformation in the cervical and upper thoracic part. No structural deformation of the vertebrae was seen in the Antero-Posterior and Lateral radiographs [Table/Fig-2]. The patient had attained skeletal maturity which was defined as Risser sign 5 on radiograph of the pelvis [1].
Preoperative image showing tilting of the head to the right with a mild rise of the ipsilateral shoulder and the projection of the chin to the left side.

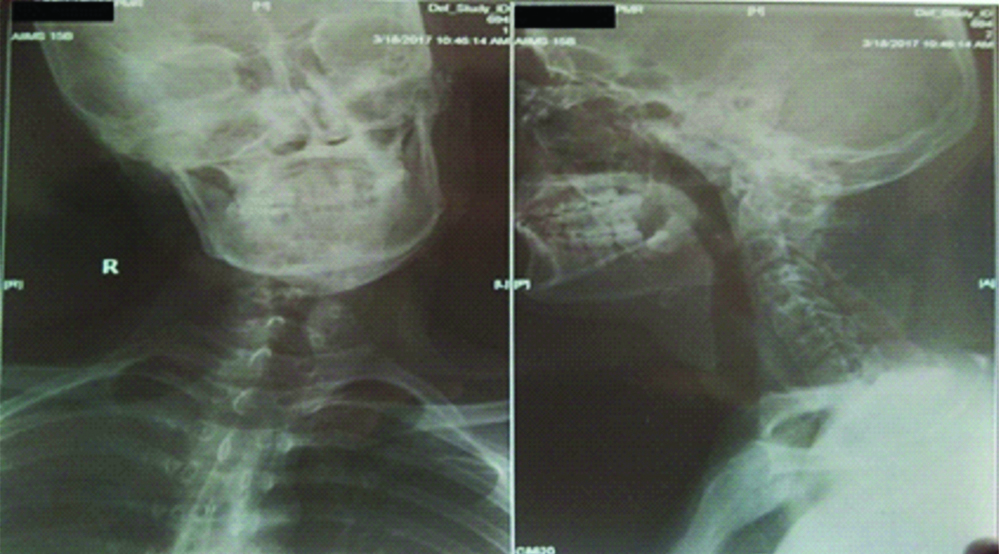
Radiograph of the cervical and thoracic spine antero-posterior and lateral view showing compensatory deformation and no structural deformation.
A bipolar release was planned and a distal incision was made in line with the cervical skin crease. The clavicular portion of the SCM was released completely and an intraoperative assessment of cervical Range Of Motion (ROM) was done and mild residual restriction in ROM was noted. Subsequently, a short incision was made behind the ear and the SCM insertion was divided just distal to the tip of mastoid. ROM was assessed again and release was found to be adequate and, therefore, the sternal head was not released. Subcuticular suturing was done to reduce scarring as much as possible [Table/Fig-3,4].
Intraoperative image showing complete release of clavicular head and proximal attachment of SCM muscle with intact sternal head.

Intraoperative image showing subcuticular suturing of incisions with intact sternal head.

Postoperatively, a neck exercise program including active and passive movements was started after one week and immobilisation with a torticollis brace was done for three months [Table/Fig-5].
Postoperative immobilisation with a custom moulded torticollis brace.

Modified Lee’s scoring system was used for the assessment of neglected muscular torticollis in the patient, postoperatively. An excellent result was given 14-15 points; good result 12-13 points; a fair result 10-11 points and a poor result is given 9 or less [2].
Patient got excellent results at the three months follow-up (Score=14 on Modified Lee’s Scale) and improvement persisted (Score=14) at the 15 months follow-up [Table/Fig-6,7].
Postoperative follow-up at 15 months (Front view).

Postoperative follow-up at 15 months (Rear view).

Discussion
The timing of surgical intervention is a crucial factor in influencing outcome. Best outcomes are obtained between 1 to 4 years of age group. After five years of age, the efficacy of surgery is reduced due to irreversible craniofacial deformity; however, it is still beneficial in older children in terms of cosmetic and functional improvements. There is little consensus on the treatment approach of neglected CMT after skeletal maturity in adults. Operative treatment has been found to have little value after skeletal maturity and may lead to more complications. However, a few studies have shown good clinical outcome in neglected case of adult CMT [3-5].
Several operations are in vogue to release the SCM muscle in torticollis. These include unipolar release of the muscle distally for mild deformity, bipolar release, bipolar release with Z-plasty for moderate and severe torticollis and endoscopic release [6].
To the best of our knowledge, there has been no technique described in literature wherein the sternal head was not released either completely or via Z-plasty prior to proximal release. However, since the patient had mild residual deformity after releasing the clavicular head on intra-operative assessment, proximal release was carried out at the mastoid to correct the mild residual deformity. This was done to maintain the ‘V-Contour’ of the neck especially as skeletal maturity had been attained with negligible chances of recurrence.
Standard bipolar release technique entails the complete release of the clavicular end and lengthening of the sternal end by Z-plasty. The mastoid end is subsequently released though an incision just below the tip of the mastoid process [7]. However, in this new technique the sternal end of the SCM was not disturbed at all.
This method of correction also leaves a window of an opportunity for further correction by releasing the sternal head in case of recurrence. It also has the advantage of preserving normal anatomy of the sternal head with less scarring. It is a safer procedure as proximity to major vessels is avoided.
Permission was obtained from the patients for presentation of this case.
Conclusion
Good postsurgical results can be obtained in adults with neglected CMT. ‘V-Contour’ of the neck can be maintained without Z-plasty at the sternal end in moderate to severe torticollis using this technique.
[1]. Yang JH, Bhandarkar AW, Suh SW, Hong JY, Hwang JH, Ham CH, Evaluation of accuracy of plain radiography in determining the Risser stage and identification of common sources of errorsJournal of Orthopaedic Surgery and Research 2014 9(1):10110.1186/s13018-014-0101-825407253 [Google Scholar] [CrossRef] [PubMed]
[2]. Omidi-Kashani F, Hasankhani EG, Sharifi R, Mazlumi M, Is surgery recommended in adults with neglected congenital muscular torticollis? A prospective studyBMC Musculoskelet Disord 2008 9:15810.1186/1471-2474-9-15819036153 [Google Scholar] [CrossRef] [PubMed]
[3]. Lim KS, Shim JS, Lee YS, Is sternocleidomastoid muscle release effective in adults with neglected congenital muscular torticollis?Clin Orthop 2014 472(4):1271-78.10.1007/s11999-013-3388-624258687 [Google Scholar] [CrossRef] [PubMed]
[4]. Min K-J, Ahn A-R, Park E-J, Yim S-Y, Effectiveness of surgical release in patients with neglected congenital muscular torticollis according to age at the time of surgeryAnn Rehabil Med 2016 40(1):34-42.10.5535/arm.2016.40.1.3426949667 [Google Scholar] [CrossRef] [PubMed]
[5]. Lee GS, Lee MK, Kim WJ, Kim HS, Kim JH, Kim YS, Adult patients with congenital muscular torticollis treated with bipolar release: report of 31 casesJournal of Korean Neurosurgical Society 2017 60(1):8210.3340/jkns.2016.0303.01828061496 [Google Scholar] [CrossRef] [PubMed]
[6]. Lepetsos P, Anastasopoulos PP, Leonidou A, Kenanidis E, Flieger I, Tsiridis E, Surgical management of congenital torticollis in children older than 7 years with an average 10-year follow-upJournal of Pediatric Orthopaedics B 2017 26(6):580-84.10.1097/BPB.000000000000032327203708 [Google Scholar] [CrossRef] [PubMed]
[7]. Sudesh P, Bali K, Mootha AK, Dhillon MS, Results of bipolar release in the treatment of congenital muscular torticolis in patients older than 10 years of ageJournal of Children’s Orthopaedics 2010 4(3):227-32.10.1007/s11832-010-0254-x21629376 [Google Scholar] [CrossRef] [PubMed]