Pneumococcal Vaccination among Adults with Respiratory Diseases-Indications, Adherence and Roadblocks
Divya Ramachandran1, Rajesh Venkitakrishnan2, Jolsana Augustine3, Melcy Cletus4
1 Consultant Pulmonologist, Department of Pulmonary Medicine, Rajagiri Hospital, Kochi, Kerala, India.
2 Senior Consultant Pulmonologist and Head, Department of Pulmonary Medicine, Rajagiri Hospital, Kochi, Kerala, India.
3 Consultant Pulmonologist, Department of Pulmonary Medicine, Rajagiri Hospital, Kochi, Kerala, India.
4 Junior Specialist, Department of Pulmonary Medicine, Rajagiri Hospital, Kochi, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jolsana Augustine, Consultant Pulmonologist, Department of Pulmonary Medicine, Rajagiri Hospital, Kochi-683112, Kerala, India.
E-mail: j_augustine08@ymail.com
Introduction
Globally, invasive pneumococcal disease poses a major challenge to the health system and causes significant economic burden. Pneumococcal vaccination is a recommended and well adhered practice among paediatric age groups as opposed to adult population, where it is often overlooked or ignored. CDC recommends pneumococcal vaccination in all subjects more than 65 years. In subjects less than 65 years, those with certain associated medical conditions are targets to pneumococcal vaccination strategy.
Aim
To evaluate the indications for pneumococcal vaccination in adult subjects admitted with respiratory diseases to a tertiary care facility, as well as to examine the adherence to pneumococcal vaccination protocols. In those who were not vaccinated as per guidelines, to determine the reasons for non-compliance to vaccination guidelines.
Materials and Methods
This was a retrospective observational study, which was carried out in the pulmonary medicine unit of a tertiary care hospital in Kerala, Southern India. Subjects admitted to the respiratory unit with various diseases over a three month period from January 2018 to March 2018 were included in the study. The demographic data, primary disease and medical comorbidities were noted. The indications to pneumococcal vaccination as per the CDC recommendations were evaluated. The actual subjects who underwent vaccine administration were noted down and reasons for non-compliance were recorded. The collected data were analysed using descriptive statistical methods, in which categorical variables were expressed as frequency and percentage, and continuous variables were analysed using mean and standard deviation with the Word excel software.
Results
A total of 284 patients were admitted to the respiratory unit in the study period due to varying primary respiratory diseases and comorbidities. Of these 268 patients were eligible for pneumococcal vaccination as per CDC criteria. Of these 268 patients 216 patients (80.59%) were vaccinated with either PPV or PCV depending on patient preference. A total of 52 patients were not vaccinated (19.4%). The reason for non-adherence to vaccination in these patients was variable. Sixteen patients (30.77%) received vaccination from another health care centre outside our hospital prior to admission. Three patients (5.77%) were transferred to another department for further care, but vaccination was not done at either units. A total of 26 patients (50%) with suspected Obstructive Sleep Apnea (OSA), who were admitted for overnight polysomnography, were not given vaccination although all of them had indications. One patient expired and two patients (3.84%) refused due to social reasons. Active counselling and vaccine recommendation was found to be missing in the case records of four patients, (7.69%) probably due to overlooking on the part of medical team.
Conclusion
A pneumococcal vaccination adherence rate of 81% was noted in the present study. Indications for pneumococcal vaccination were overlooked in a sizeable inpatient population being admitted for overnight polysomnography. Active counselling and vaccination recommendation was also missing in a small number of subjects.
Adult vaccines, Chronic lung diseases, Pneumococcal infections
Introduction
Invasive pneumococcal disease is an important cause of morbidity and mortality in adults aged above 65 years of age. Pneumococcal pneumonia, bacteraemia and meningitis are the syndromes grouped under invasive pneumococcal disease. Subjects with medical conditions that hamper their ability to mount antibody response to capsular polysaccharides of pneumococci are especially vulnerable [1]. Patients with chronic lung disease are at increased risk for pneumococcal pneumonia, and patients with medical comorbidities like chronic kidney disease, chronic liver disease and heart failure are more likely to have adverse outcomes if pneumonia occurs [2]. Asplenia greatly increases the risk for overwhelming pneumococcal sepsis, and a cerebrospinal fluid leak or a cochlear implant greatly increases the risk for pneumococcal meningitis. In the last two decades, asthma is also recognised as a significant risk factor for pneumococcal disease [3]. Diabetes independently increases the likelihood of invasive pneumococcal disease [4]. Pneumococcal vaccination is recommended for all children and for adults who have a condition that places them at increased risk for developing pneumonia or invasive pneumococcal disease or having a risk for serious outcome if pneumonia occurs.
Pneumococcal vaccination can reduce the mortality and morbidity risks associated with pneumococcal diseases by 50%. It protects against invasive infections like, meningitis, pneumonia and non-invasive infections like otitis media, sinusitis and bronchitis. There are two types of pneumococcal vaccines available for use. They are Polysaccharide and conjugate vaccines. The polysaccharide vaccine contains capsular polysaccharides from the 23 most commonly infecting pneumococci that cause about 60% of all pneumococcal infection in adults. The conjugate vaccine 13-valent pneumococcal conjugated vaccine in which pneumococcal polysaccharides are coupled with a carrier protein. While PPV23 induces only serotype specific antibodies, PCV13 generates the formation of both serotype specific antibodies and B memory cells, which are associated with a longer duration of vaccine-induced immune responses [5].
Despite clear-cut recommendations by the CDC [6], the adherence to pneumococcal vaccine among adult subjects has been traditionally low. Multiple factors contribute to low vaccination rates, including ignorance about the vaccine, myths, cost, suspicion on efficacy and fear of adverse effects. The present study looks at the proportion of in-patient subjects of a tertiary care respiratory ward who had one or more indications to pneumococcal vaccination over a three month period, the prescription rate among those who had indications and the cause for non-adherence to vaccination strategy.
Materials and Methods
The present study was a retrospective observational study which was conducted in the respiratory in-patient ward of a tertiary care hospital in Kochi, Southern India. The study was approved by institutional ethics committee.
All patients who were admitted to the respiratory medicine unit with various diseases over a three months period from January 2018 to March 2018 were included in the study. The available medical records were studied with regard to the primary disease which warranted admission and presence of any medical comorbidities. All subjects were analysed with complete blood count examination, fasting and post prandial sugar values, renal and liver function tests, 12 lead EKG, echocardiography and ultrasound abdomen. The presence of any indication for pneumococcal vaccination as per the CDC recommendation was noted. As per CDC recommendation pneumococcal vaccination is indicated in the following class of patients [6].
Those more than 65 years of age
Those with any chronic disease of heart, lung, liver and kidney
Immunosuppressed
Smokers.
Those subjects who do not have an indication for giving pneumococcal vaccination and those with any medical contraindication for an IM or subcutaneous injection were excluded from the study. The patients were explained about the need for vaccination and either polysaccharide or conjugate vaccine was administered as per patient’s preferences after obtaining their consent. The vaccination was done by the staff nurse in charge of the patient. The adherence to vaccination in those subjects who had indication for pneumococcal vaccine was noted down. The percentage of patients vaccinated in each of the common respiratory diseases group was studied. In case of non-administration of vaccine, the reason for the same was noted down. The collected data were analysed using descriptive statistical methods and results were noted using SPSS software version 25.
Results
A total of 284 patients were admitted under our department during the study period. Of these 268 patients, eligible for pneumococcal vaccination as per CDC criteria were included in the study. Of these, 173 (65.53%) were males and 95 (35.98%) females. The mean age of study population was 67.2 years. The demographic characteristics of the study subjects are depicted in [Table/Fig-1]. Almost half of the study subjects were greater than 65 years, which itself is an indication for pneumococcal vaccination even in the absence of associated medical diseases. Patients less than 45 years contributed to only 11% (30 patients) of study population.
Demographic characteristics of study population.
| Characteristics | Numbers | Percentage |
|---|
| Age (years) | | |
| <45 | 30 | 11.19% |
| 45-65 | 106 | 39.56% |
| >65 | 132 | 49.25% |
| Sex | | |
| Males | 173 | 64.55% |
| Females | 95 | 35.45% |
| Primary diseases | | |
| COPD | 101 | 37.69% |
| Pneumonia | 81 | 30.22% |
| ILD | 4 | 1.49% |
| Bronchial asthma | 30 | 11.19% |
| TB | 5 | 1.87% |
| OSA | 26 | 9.70% |
| Hemoptysis | 2 | 0.74% |
| Bronchiectasis | 9 | 3.36% |
| Pleural effusion | 7 | 2.62% |
| Pneumothorax | 3 | 1.12% |
| Comorbid illnesses* | | |
| Diabetes | 193 | 72.01% |
| Hypertension | 167 | 62.31% |
| Thyroid dysfunction | 144 | 53.7% |
| DLP | 105 | 39.1% |
| Heart disease | 56 | 20.89% |
| CKD/CLD | 18 | 6.7% |
*Most patients had combinations of any two or more comorbid illnesses
Majority of patients were admitted with an exacerbation of underlying airway disease, viz., COPD, asthma or bronchiectasis. This was followed by pneumonia. Most of the patients (88.06%) were having more than one comorbid illnesses. Majority of the study group were having diabetes (193 patients, 72.01%) followed by hypertension in 167 patients (62.31%). The thyroid dysfunction was seen in 144 patients (53.7%), dyslipidaemia in 105 patients (39.1%) and heart diseases in 56 patients (20.89%). All these patients were being followed up regularly as per the consultant’s decisions. For the patients in need of multidisciplinary care, cross consultations were taken from the concerned departments and follow ups were arranged at the time of discharge.
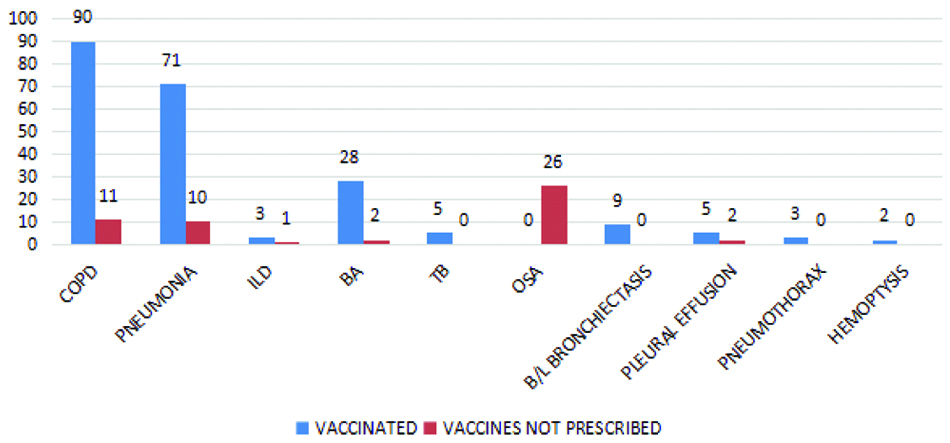
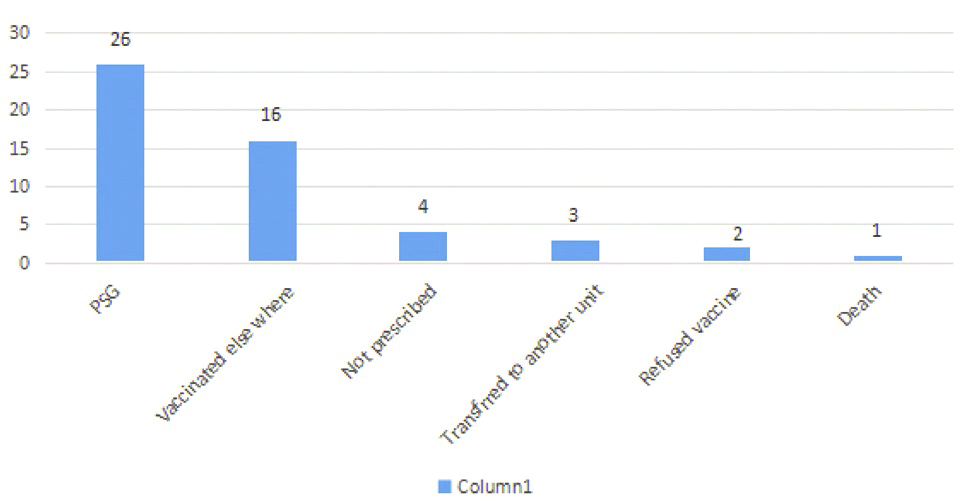
A total of 268 subjects admitted in the study period had one or more indications for pneumococcal vaccination. A total of 216 patients (80.59%) were vaccinated with either PPV or PCV depending on patient preference. The percentage of patients vaccinated in each disease group is summarized in [Table/Fig-2]. A total of 52 patients (19.4%) were not vaccinated. The reasons for failure to vaccinate these patients were variable and summarized in [Table/Fig-3]. A total of 16 patients received vaccination from another health care centre outside our hospital prior to the present admission, and as such did not require further administration. Three patients were later transferred to another department for further care, but vaccination was not done at either unit despite indications for the same. One patient expired during hospital stay. Two patients refused vaccination despite counselling on the benefits of the vaccine, due to concerns on the adverse effects of vaccine. Active counselling and vaccine recommendation was found to be missing in the case records of four patients, which may be viewed upon as non-exploitation of the medical team to utilise the vaccination opportunity. A total of 26 patients were admitted with suspected OSA for overnight polysomnography. These patients were discharged immediately after the study without focus on the vaccination recommendations, although all of them had medical comorbidities necessitating pneumococcal vaccine. They were followed up in outpatient department with sleep study reports. For those patients with associated chronic diseases, consultations were taken from the respective departments and managed accordingly.
Vaccination status in each disease group.
Reasons identified for non-vaccination.
Discussion
The present study reveals a pneumococcal vaccine administration rate of 80.59% in subjects admitted to respiratory unit with various demographic and medical indications for vaccination. This is in sharp contrast to some of the previous studies conducted in this arena, which have revealed adherence rates ranging from 2% to 82% [7-9]. A vaccine safety data link study has shown a vaccine adherence rate of 26% only in 60-65 year old population, which sharply rises to 82% in those above 65 years [10]. A single centre cross-sectional study revealed a vaccination rate of 41% in diabetic subjects [11]. The higher adherence rates in the present study may be a direct offshoot of the fact that the study was carried out in admitted patients as opposed to busy OPD settings, who are bound to be sicker than OPD subjects needing a dedication of greater time to the care of these patients. A vast majority of subjects in the present study also had more than one comorbidity, which automatically tends to alert the clinician of the potential need to administer pneumococcal vaccination.
The causes of non-adherence to vaccination guidelines are many and varied. In countries like India, pneumococcal vaccination expenses are not reimbursed by state and expenses are to be met out of patient’s pocket. The current cost of pneumococcal vaccine being Rs.1600/- per dose for 23 valent vaccine and Rs.3800/- per dose for conjugate 13 valent vaccine which may be difficult to afford for a sizable percentage of our population. Concerns over the safety of vaccine, vaccination myths and negative publicity stand as stumbling blocks in successfully implementing a vaccination programme. There is a lack of focus on adult vaccinations in undergraduate as well as post graduate training programmes across the country. A Western survey states that denial on the part of the patient is one of the major reasons for non-compliance [12,13]. In the in-patient setting, patients are much more sensitive to accept any prescribed vaccination and hence all of our patients have adhered to the suggestions. Previous researchers have attempted to define predictors of pneumococcal vaccine in older adults with pneumonia [14]. Various studies identified different predictive indicators for pneumococcal vaccination. One study identifies getting an influenza vaccine within the past, multiple chronic conditions, and age more than 70 years and religious faith as the variables determining vaccination acceptance. Recommendation by a health care provider was found to be an important predictor of PPV immunization among older adults in one study [15,16].
Rural to urban differences have been mentioned as predictors for acceptance of pneumococcal vaccination and a rural study revealed that knowing someone with pneumonia is a strong predictor of successful acceptance [17]. Further, every centre is unique with regard to its patient profile as well as social, culture and economic background of subjects. A proportion of our study subjects have been unique in the sense that our respiratory unit constitutes a referral centre for overnight polysomnography study for subjects with suspected OSA syndrome. These subjects are admitted overnight to the unit and form part of the in-patient subjects, but are not comprehensively counselled for vaccination protocols despite many of them having indications. This group constitutes the largest bulk of non-adherence to pneumococcal vaccination and needs to be targeted in the future.
Poor promotion of adult pneumococcal vaccine at community level compared with paediatric population is another barrier for vaccination. The community based educational program about pneumococcal vaccination will increase the uptake of this vaccine [16,18]. Sharing vaccination responsibilities with paramedical staff can improve vaccination rates in community [19,20].
Limitation
Our study has several limitations. This is a hospital based study on pneumococcal vaccination adherence whereas the real life challenge is getting the protocol implemented in OPD population who are not sick. We did not discriminate between subjects who received polysaccharide versus conjugate vaccine and did not stick to dual agent vaccination. This is crucial considering PPV23-induced hypo responsiveness and its implications in designing highly effective vaccination schedules for the optimal protection for high-risk individuals, which has been a topic of controversy in recent years. Subjects with suspected sleep apnoea being admitted for sleep study constitute a much less sick patient group as compared to in-hospital patients admitted for other respiratory ailments, and including them in the study cohort adds to inhomogeneity in patient population. Accepting all these drawbacks, the study still has the merit of being a unique work describing vaccination practices in Indian respiratory hospitalised patients.
Conclusion and Recommendation
The vast majority of hospitalised patients with respiratory ailments have one or more indications for pneumococcal vaccination. The adherence rate to vaccination protocols in the present study has been high, probably owing to the good consultant awareness and recommendations to the schedule. Despite this fact, a small minority of subjects were not counselled on the need of vaccination and indications were overlooked. Focus also needs to be given to conducting research on heterogeneous patient populations as well as social, economic and cultural settings.
*Most patients had combinations of any two or more comorbid illnesses
[1]. Nelson AL, Roche AM, Gould JM, Chim K, Ratner AJ, Weiser JN, Capsule enhances pneumococcal colonization by limiting mucus-mediated clearanceInfect Immun 2007 75(1):83-90.10.1128/IAI.01475-0617088346 [Google Scholar] [CrossRef] [PubMed]
[2]. Schoenmakers MCJ, Hament JM, Andre Risk factors for invasive pneumococcal diseaseRev Med Microbiology 2002 13(1):29-36.10.1097/00013542-200201000-00003 [Google Scholar] [CrossRef]
[3]. Boikos C, Quach C, Risk of invasive pneumococcal disease in children and adults with asthma: a systematic reviewVaccine 2013 42(31):4820-26.10.1016/j.vaccine.2013.07.07923965221 [Google Scholar] [CrossRef] [PubMed]
[4]. Mohan V, Unnikrishnan R, Thomas N, Pneumococcal infections and immunization in diabetic patientsJ Postgrad Med 2011 57:78-81.10.4103/0022-3859.7429921206113 [Google Scholar] [CrossRef] [PubMed]
[5]. Stein KE, Thymus-independent and thymus-dependent responses to polysaccharide antigensJ Infect Dis 1992 165:S49-S52.10.1093/infdis/165-Supplement_1-S491588177 [Google Scholar] [CrossRef] [PubMed]
[6]. Centers for Disease Control and Prevention (CDC)Advisory Committee on Immunization Practices. Updated recommendations for prevention of invasive pneumococcal disease among adults using the 23-valent pneumococcal polysaccharide vaccine (PPSV23)MMWR Morb Mortal Wkly Rep 2010 59:1102 [Google Scholar]
[7]. Nowalk MP, Middleton DB, Zimmerman RK, Hess MM, Skledar SJ, Jacobs MA, Increasing pneumococcal vaccination rates among hospitalized patientsInfect Control Hosp Epidemiol 2003 24(7):526-31.10.1086/50224012887242 [Google Scholar] [CrossRef] [PubMed]
[8]. Dexter PR, Perkins S, Overhage JM, Maharry K, Kohler RB, McDonald CJ, A computerized reminder system to increase the use of preventive care for hospitalized patientsN Engl J Med 2001 345(13):965-70.10.1056/NEJMsa01018111575289 [Google Scholar] [CrossRef] [PubMed]
[9]. Jha AK, Wright SM, Jonathan B, Performance measures, vaccinations, and pneumonia rates among high-risk patients in veterans administration health careAm J Public Health 2007 97(12):2167-72.10.2105/AJPH.2006.09944017971554 [Google Scholar] [CrossRef] [PubMed]
[10]. Jackson LA, Baxter R, Naleway AL, Patterns of pneumococcal vaccination and revaccination in elderly and non-elderly adults: A Vaccine Safety Datalink studyBMC Infectious Diseases 2009 9:3710.1186/1471-2334-9-3719321001 [Google Scholar] [CrossRef] [PubMed]
[11]. Alcusky MJ, Pawasauskas J, Adherence to guidelines for hepatitis b, pneumococcal, and influenza vaccination in patients with diabetesClin Diabetes 2015 33(3):116-22.10.2337/diaclin.33.3.11626203204 [Google Scholar] [CrossRef] [PubMed]
[12]. Punzalan M, Anjum MR, Beattie TL, Adult vaccination: barriers to compliance in the 65+ population in western New YorkAcad J Ped Neonatol 2016 1(1):AJPN.MS.ID.55555510.19080/AJPN.2016.01.555555 [Google Scholar] [CrossRef]
[13]. MacDougall DM, Halperin BA, MacKinnon-Cameron D, Li Li, McNeil SA, Langley JM, The challenge of vaccinating adults: Attitudes and beliefs of the Canadian public and healthcare providersBMJ Open 2015 5(9):e00906210.1136/bmjopen-2015-00906226419683 [Google Scholar] [CrossRef] [PubMed]
[14]. Krueger P, St Amant O, Loeb M, Predictors of pneumococcal vaccination among older adults with pneumonia: findings from the Community Acquired Pneumonia Impact StudyBMC Geriatrics 2010 10:4410.1186/1471-2318-10-4420591180 [Google Scholar] [CrossRef] [PubMed]
[15]. Stehr-Green PA, Sprauer MA, Williams WW, Sullivan KM, Predictors of vaccination behaviour among persons ages 65 years and olderAm J Public Health 1990 80(9):1127-29.10.2105/AJPH.80.9.11272382756 [Google Scholar] [CrossRef] [PubMed]
[16]. Hurley LP, Bridges CB, Harpaz R, Allison MA, O’Leary ST, US physicians perspective of adult vaccine deliveryAnn Intern Med 2014 160(3):161-70.10.7326/M13-233224658693 [Google Scholar] [CrossRef] [PubMed]
[17]. Madhavan SS, Borker RD, Fernandes AW, Amonkar MM, Rosenbluth SA, Assessing predictors of influenza and pneumonia vaccination in rural senior adultsJ Health and Soc Policy 2003 18(2):71-93.10.1300/J045v18n02_05 [Google Scholar] [CrossRef]
[18]. Grabenstein JD, Pharmacists as vaccine advocates: roles in community pharmacies, nursing homes, and hospitalsVaccine 1998 16(18):1705-10.10.1016/S0264-410X(98)00131-5 [Google Scholar] [CrossRef]
[19]. Jones KL, Hammer AL, Swenson C, Appel A, Phibbs S, Hill F, Improving adult immunization rates in primary care clinicsNurs Econ 2008 26(2):404-07. [Google Scholar]
[20]. Ko KJ, Wade RL, Yu HT, Miller RM, Sherman B, Goad J, Implementation of a pharmacy-based adult vaccine benefit: recommendations for a commercial health plan benefitJ Managed Care Pharm 2014 20(3):273-82.10.18553/jmcp.2014.20.3.27324564808 [Google Scholar] [CrossRef] [PubMed]