Serum Creatine Kinase Activity among Hypertensive Patients and its Role as a Predictor for Failure of Antihypertensive Treatment
Surankita Sukul1, Jyotirmayee Bahinipati2, Saurav Patra3, Kandasamy Ravichandran4
1 Tutor, Department of Biochemistry, IQ City Medical College, Durgapur, West Bengal, India.
2 Associate Professor, Department of Biochemistry, Kalinga Institute of Medical Sciences, Bhubaneswar, Odisha, India.
3 Consultant, Department of Biochemistry, Apollo Hospital, Bhubaneswar, Odisha, India.
4 Associate Professor, Department of Statistics, PIMS, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jyotirmayee Bahinipati, Associate Professor, Department of Biochemistry KIMS, Patia, Bhubaneswar-751016, Odisha, India.
E-mail: drjyotirmayee@yahoo.co.in
Introduction
Creatine Kinase (CK), a key enzyme of cellular energy metabolism helps the cells to function under high demands by involving in contractile processes and active trans-membrane transport by readily providing Adenosine-5’-triphosphate (ATP). Higher CK activity increases cardiovascular trophic responses and development of arterial hypertension. Hence, high CK activity may increase hypertension risk and may also be a cause behind the hypertensive treatment failure.
Aim
In the present study, serum CK levels are compared between hypertensive and normotensive study subjects and association of serum CK in hypertensive treatment failure cases.
Materials and Methods
A total of 75 known hypertensive patients who were under antihypertensive treatment for ≥3 months were taken as cases. Further grouping of the patients was done based upon the response to antihypertensive treatment into treatment control (n=40) and without treatment control (n=35) groups. Forty individuals age and sex matched normotensive control were taken. Serum Creatine Kinase, BMI, Systolic Blood Pressure, Diastolic Blood Pressure, was measured in the study group. Kruskal Wallis test was done to compare the parameters in all the three study groups. Correlation of serum CK with other parameters was done. Cut-Off value for serum CK was calculated in hypertensive cases.
Results
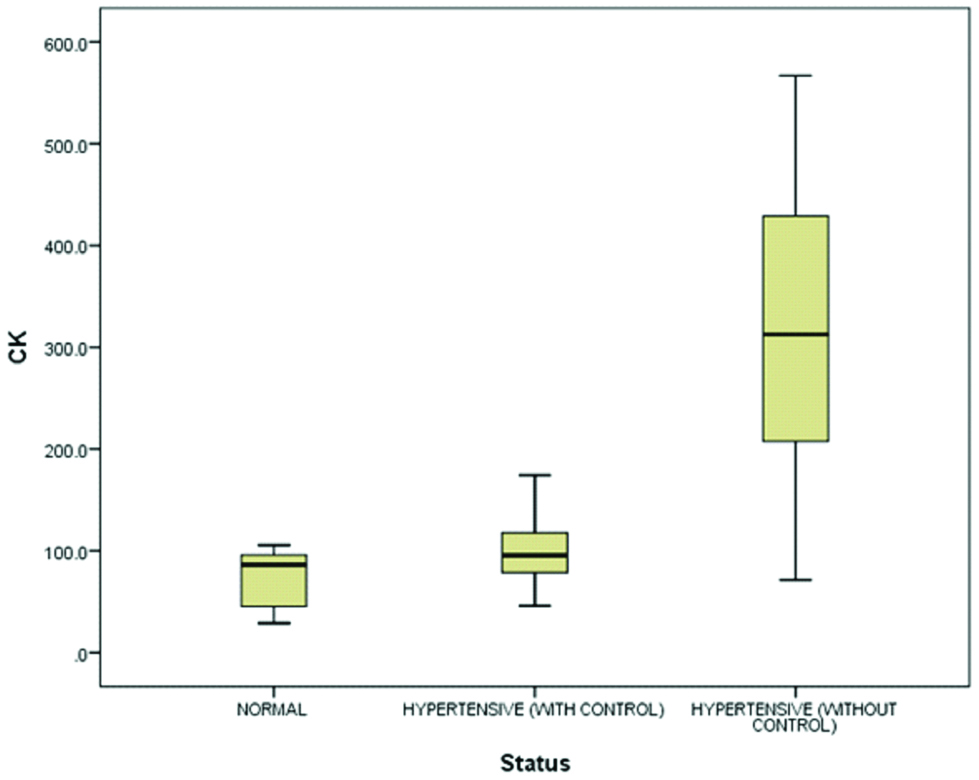
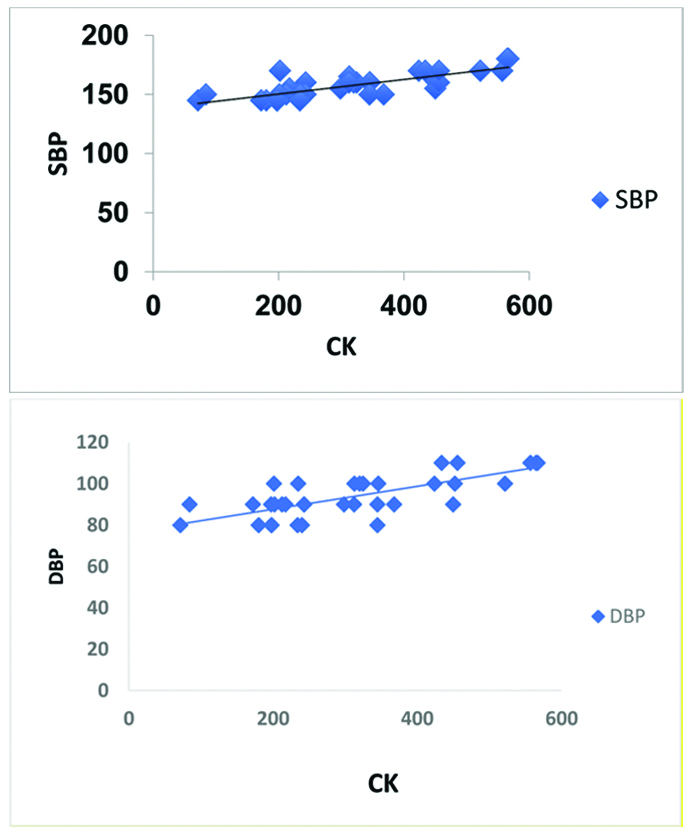
CK was found to be higher in hypertensive cases with treatment control (99.55±31.34) U/L compared to normotensives (72.66±25.42) U/L. Significantly higher CK level was found in hypertensive treatment failures (313.92±133.12) U/L compared to treatment control cases. Statistically significant correlation was found between serum CK with SBP and DBP in hypertensive treatment failure cases. A cut-off value of 168.5 U/L was found out in hypertensive patients.
Conclusion
Serum CK was found to be associated with severity of blood pressure and failure of antihypertensive therapy.
Blood pressure, Body mass index, Creatine Kinase
Introduction
Hypertension continues to be an important health issue worldwide. It has been associated with increased risk of coronary artery diseases and an independent risk for cardiovascular and chronic kidney diseases [1]. Global burden of diseases study has reported that in the year 2013 high systolic blood pressure led to 10.8 million deaths and 208.1 million Disability Adjusted Light Years (DALY) [2]. Worldwide cardiovascular disease accounts for approximately 17 million deaths a year of which, complications of hypertension account for 9.4 million deaths worldwide [3]. WHO data says by 2025 the global burden of hypertension will increase by 60% worldwide with higher in developing countries [4]. Developing countries specifically presents with higher incidence of undiagnosed, untreated and uncontrolled hypertension attributed to poor health system which may be because of population growth, ageing, behavioral risk factors, unhealthy food habits, lack of exercise and increase exposure to persistent stress [5]. Despite many efforts to treat hypertension JNC 7 (Joint National Committee) on prevention indicated 30% of hypertensive patients are unaware of their illness, 42% are not under treatment and 69% did not have their hypertension controlled in spite of patient’s adherence and physician’s proper treatment in accordance to required therapeutic criteria [6]. In the present scenario hypertensive treatment failure has become a major health concern in US and developing countries. In India only 25.6% of hypertensive had their BP under control with one fifth control in urban areas and even less than tenth in rural areas [7]. Substantial proportion have uncomplicated primary hypertension and not well explained why they are not able to obtain required treatment control despite therapy given in accordance to therapeutic guidelines. Adequate hypertension treatment and control is a necessity to reduce the mortality associated with it.
CK is abundantly expressed in both mitochondrion and cytosol. It catalyzes the transfer of high-energy phosphate moiety between Creatine and ADP [8].
ADP+Creatine P+H+Creatine Kinase→ATP+CreatineThis rate of generation of ATP by CK is much greater than that generated by oxidative phosphorylation. CK is specifically involved in skeletal muscle contraction, cardiovascular contractility, sodium retention, remodeling of the arteries where rapid generation of ATP is required. Till date CK is assayed clinically as a marker of damage of CK rich tissues [9]. Some studies have mentioned that CK is the predictor of blood pressure independent of age, sex, BMI or ethnicity [10]. High activity of these enzymes in the resistance arteries enhances pressure response leading to high blood pressure.
Studies have suggested association of high creatine kinase with hypertension [11,12]. Study in animal models have shown lowering in CK with antihypertensive therapy [13]. It has been also found that high serum CK may be a genetic factor increasing hypertension risk in certain population [14].
With the above known facts in view, this study is an attempt to focus on the levels of creatine kinase in hypertensive patients under treatment and find out its probability of association with hypertensive treatment failure.
Materials and Methods
The present study was done in Kalinga Institute of Medical Sciences with prior ethical clearance from institutional ethical committee from a period of August 2015 to December 2016. Written informed consent was taken from all the study subjects after explaining the aim and benefits of the study.
Study group included 75 known hypertensive cases of age group 25-60 years who were under antihypertensive treatment for at least more than three months. Forty age and sex matched normotensive subjects were selected.
Subjects with resistant hypertension (taking at least 3 medicines and one amongst them is a diuretic and their blood pressure not controlled), with recent intramuscular injection, known muscular disorder, heart disease, renal impairment, statin intake and persons who recently donated blood or received any kind of vaccination within three months were excluded from the study.
All the subjects were asked for abstinence from muscular exercise for at least three days prior to the test procedure. Normal daily activities were allowed.
Height and weight were recorded and BMI was calculated. Blood pressure was measured in a quiet and relaxed surrounding in the sitting position in the dominant arm at heart level. Mean of three consecutive blood pressure readings were taken into account to avoid the variability. Subjects were classified as treated controlled hypertension for those taking antihypertensive drugs and with SBP <140 mm of Hg and DBP <90 mm of Hg, treated uncontrolled hypertensives were those who were taking antihypertensive drugs with SBP ≥140 mm of Hg and DBP ≥90 mm of Hg, persons with SBP <140 mm of Hg and DBP <90 mm of Hg at three different sittings with no history intake of antihypertensive drugs were considered as normotensives.
CK activity was measured after three days of rest by Creatine Kinase N-Acetyl Cystine (CK-NAC) activated enzymatic UV method within six hours of sample collection in automated analyzer (Roche Diagnostics) by modified International Federation of Clinical Chemistry (IFCC) method. CK catalyzes reversible transfer of phosphate group from phosphocreatine to ADP. The ATP formed along with glucose is catalysed by hexokinase to form glucose 6 phosphate, which reduces Nicotinamide Adenine Dinucleotide Phosphate (NADP) to NADPH (reduced NADP) in presence of glucose 6 phosphate dehydrogenase. The rate of reduction of NADP to NADPH is measured as increase in absorbance at 340 nm which is proportional to CK activity in the serum [15].
Statistical Analysis
Data were presented as mean±SD. Wilcoxon Mann-Whitney U test was done for better comparison of Creatine Kinase activity in normotensive control and hypertensive subjects. Kruskal Wallis test was done to compare the parameters in all the three study groups. Pairwise comparison of status and Bonferroni adjustment was done to know which specific mean differed. Spearman’s correlation between Creatine kinase and SBP and DBP was done in all the study groups. Area Under Curve (AUC) and the cut-off value for serum Creatine Kinase were calculated by Receiver Operating Curve (ROC). A p-value <0.05 was considered as significant. All statistical analysis was done with SPSS software version 20.0.
Results
[Table/Fig-1] shows that there is significant difference in BMI, SBP, DBP, CK in the three study groups with statistically significant increase in hypertensive patients. BMI in hypertensive patients without control was found to be (31.27±3.35 kg/m2) which was significantly higher compared to hypertensive patients with control (29.70±4.30 Kg/m2). [Table/Fig-2] shows the comparison of BMI and CK between normotensives and hypertensives showing statistically significant increase in parameters in hypertensive group. The distribution of creatine kinase in the study groups has been depicted in a box plot showing the mean CK in hypertensive patients with treatment control was (99.55±31.34) U/L which was significantly higher compared to the normotensives (72.66±25.42) U/L. CK in hypertensive patients without treatment control (313.92±133.12) U/L showed significantly higher values than hypertensives with treatment control group (p<0.001) [Table/Fig-3]. There is statistically significant correlation between CK with SBP and DBP in hypertensive patients without treatment control as shown in [Table/Fig-4a,b]. [Table/Fig-5,6] shows the ROC curve with AUC of 0.956 for creatine kinase in hypertensive subjects. [Table/Fig-7] shows a cut-off value of serum CK of 168.5 U/L in hypertensive patients with 33 subjects with hypertension without treatment control and one patient with hypertension and treatment control above this value.
Comparison of parameters in study groups.
| Parameters | Normotensive (N=40) | Hypertensive with Treatment Control (N=40) | Hypertensive without Treatment Control (N=35) | p-value |
|---|
| Age (in years) | 60.2±7.38 | 60.37±7.84 | 57.05±8.19 | NS |
| BMI (Kg/m2) | 25.81±1.90 | 29.70±4.30 | 31.27±3.35 | <0.05* |
| SBP (mm of Hg) | 115.80±11.09 | 130.12±6.05 | 157.29±10.31 | <0.001* |
| DBP (mm of Hg) | 74.75±7.15 | 73.78±4.41 | 94.00±10.05 | <0.001* |
| CK (U/L) | 72.66±25.42 | 99.55±31.34 | 313.92±133.12 | <0.001* |
*p-value significant
NS: Not Significant; BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure
Comparison of parameters between normotensives and hypertensives.
| Parameters | Normotensive (n=40) | Hypertensives (Hypertension with treatment control+Hypertensive without treatment control) (n=75) |
|---|
| BMI (Kg/m2) | 25.81±1.90 | 30.43±3.94* |
| CK (U/L) | 72.66±25.42 | 199.59±142.31** |
*p<0.05; **p<0.001
Box plot showing values of CK (U/L) in all the three study groups.
Correlation between CK and SBP and DBP in hypertensive without treatment control.
SBP: Systolic blood pressure; DBP: Diastolic blood pressure
ROC curve for Creatine Kinase in hypertensive subjects.
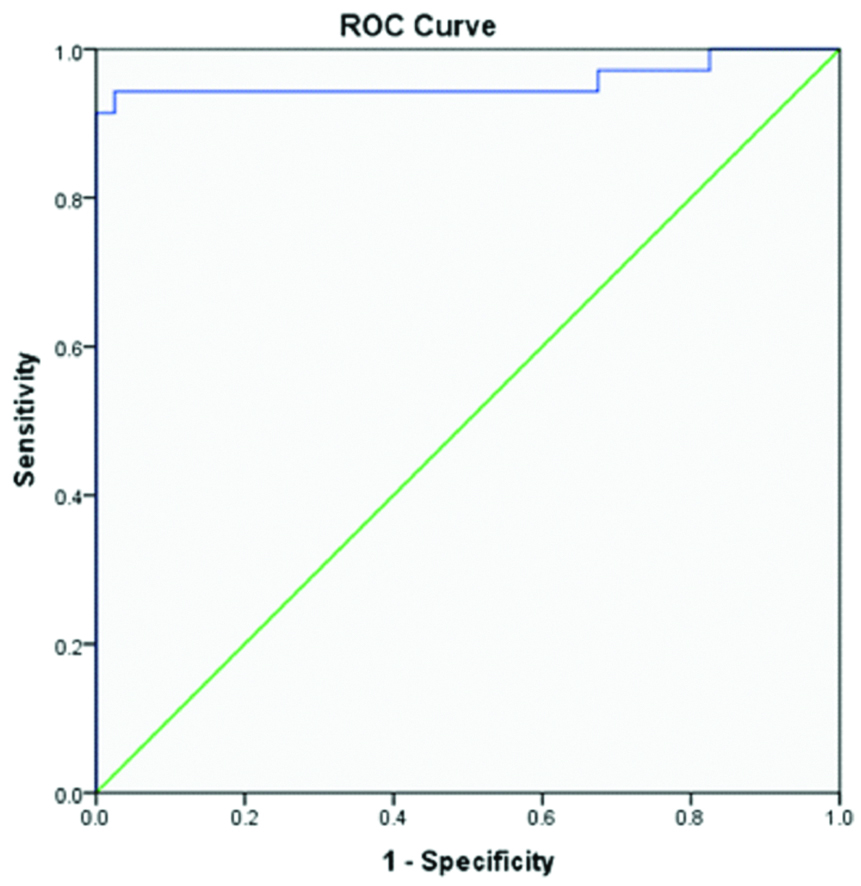
Area under the curve for Creatine Kinase in hypertensive subjects.
| Test Result Variable(s): Creatine Kinase |
|---|
| Area | Std. Error | Asymptotic Sig. | Asymptotic 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| 0.956 | 0.030 | 0.000 | 0.898 | 1.000 |
Creatine Kinase cut-off cross tabulation in hypertensive subjects.
| Parameter | Hypertensive (With Treatment Control) | Hypertensive (Without Treatment Control) | Total |
|---|
| CK 168.5_Cut-off | ≤168.5 | 39 | 2 | 41 |
| >168.5 | 1 | 33 | 34 |
| Total | 40 | 35 | 75 |
Discussion
Creatine kinase an enzyme involved with cellular energy system increases the capacity of the cells to meet high-energy demands of contractile processes and active trans-membranous transport by readily providing ATP [9].
In the present study we observed significantly higher CK level in hypertensive patients (199.59±142.31) compared to normotensive controls (72.66±25.42) U/L suggesting CK may be an associating factor contributing to increase in blood pressure. In the study, done by Johnsen SH et al., per log CK increases adjusted BP by 7.98 (3.27-12.68) mm of Hg of SBP and 4.69 (1.88-7.50) mm of Hg of DBP [10]. Our findings are also in consistence with the studies done by Brewster L et al., who found out that circulating CK is the main predictor of blood pressure in random sample of multiethnic origin [8]. In another study, done by them 48% of subjects with idiopathic increase in serum creatine kinase was hypertensive as compared to 19% of random population controls [16]. Studies have shown higher CK activity in all tissues in black population of Sub-Saharan African decent and hypothesised that it increases hypertension risk in this subgroup due to increase in pressure response [14]. According to Karamat FA et al., a strong association was found between human resistance artery CK mRNA and systemic SBP and DBP [17]. In an in vitro study done by Taherzadeh Z et al., isolated resistance arteries showed reduced vascular contractibility by 24.3% on addition of CK inhibitors like 2,4 dinitro-1-fluorobenzene [18]. Low serum CK levels are also associated with increase in fainting episodes [19]. Creatine Kinase regulates, buffers and transports energy to the sites of energy consumption like myofibrils and membrane ion pumps. At these cellular locations it is involved in contraction and active trans membranous transport processes by providing ATP readily. Creatine kinase also prevents acidosis due to ischaemia as it utilises the H+ and ADP for ATP formation. These factors result in increases trophic response resulting in increase of cardiovascular contractile reserve facilitating the development of arterial hypertension and hence, greater hypertension risk [10]. Common cause of increase in CK activity is exercise hence to avoid false results we suggested the study group a resting period of three days. In the absence of any tissue damage or any form of dysfunction increase in serum CK level suggests CK from the tissue activity [20].
In our study there was increase in serum CK in hypertensive treatment failure (313.92±133.12) U/L, which was significantly higher p<0.001 compared to hypertensive-controlled patients (99.55±31.34) U/L. A significant correlation (p<0.001) was also found out between serum CK and SBP and DBP in hypertensive treatment failure patients. These findings are in accordance to the findings of Oudman I et al., [13]. They found 72.9% treatment failure within highest CK tertile whereas 46.7% within lowest tertile. CK was found as the main predictor of treatment failure independent of age, sex, BMI, ethnicity or education level. They even found out a dose dependent association of serum CK with treatment failure. Studies have suggested that there is no direct evidence of increase in serum CK in hypertension and even hypertension does not effect the clearance of CK [8]. Even there is no such evidence that high blood pressure causes cardiovascular muscle damage causing increase in creatine kinase level. Hence resting subjects without muscle damage, serum CK is the direct measure of tissue CK. High serum CK which may be causal or induced, results in increase in contractile responses and salt retention. This increase in mean BP which is one of the important cause behind difficult to treat hypertension and hence results in hypertensive treatment failure.
Present study showed a positive association between CK and BMI in hypertensive patients. Studies have suggested that mean levels of SBP and DBP increases as BMI increases [21]. Strong and independent association between CK and BMI have also been found out [22]. In skeletal muscle higher activity of this enzyme is typically seen in type II muscle fibers, which are specifically characterised by low vascularisation and decreased capacity of uptake and oxidation of fatty acids and glucose. This promotes storage of fatty acid and glucose in adipose tissue leading to obesity [23]. Hence high CK phenotype may be responsible for obesity and hypertension. But no significant association was found between BMI and CK in hypertensive failure patients. This suggests that though BMI increases the hypertension risk, hypertensive treatment failure is independently associated with the serum CK value. A cut-off value for serum CK was found to be 168.5 from the co-ordinates of ROC curve for hypertensive patients with a sensitivity of 0.943. There were 40 hypertensive subjects above this level with 39 subjects having hypertension without treatment control. Hence a cut-off value for hypertensive subjects can be used as an independent predictor of development of hypertensive treatment failure. This can help us to segregate patients who may present with hypertensive treatment failure requiring more aggressive management and repeated follow up.
These findings suggest that creatine kinase estimation can help us to differentiate true hypertension from pseudo-hypertension and can also be used as a prognostic marker for suspected difficult to treat hypertension.
Conclusion
In congruence with previous findings our study also suggested the association of CK with hypertension. CK is also found to be higher in hypertensive treatment failure cases which is even independent of BMI. As hypertension is a multifactorial condition being affected by environmental and physiological factors, treatment failure cases must be studied cautiously in patients having multiple risk factors and co-morbidities.
Limitation
Our study had certain limitations; no detailed history of antihypertensive medication was taken into account. Presence of other comorbidities, patient’s adherence to treatment, diet, alcohol consumption that may affect the creatine kinase was not taken into account. Size of the study sample was not large enough to confer significant differences.
Hence prospective studies with history of different hypertensive medications should be taken into account for detailed association of CK with hypertension and treatment failure hypertension cases. Further studies are necessary to justify the causal association so that CK can better be used as the prognostic marker and treatment strategies can be adopted in cases of difficult to treat hypertensive cases.
*p-value significant
NS: Not Significant; BMI: Body mass index; SBP: Systolic blood pressure; DBP: Diastolic blood pressure
*p<0.05; **p<0.001
[1]. Frohlich ED, Quinlan PJ, Ochsner J, Coronary heart disease risk factors: public impact of initial and later-announced risksOchsner J 2014 14(4):532-37. [Google Scholar]
[2]. Bromfield S, Muntner P, high blood pressure: the leading global burden of disease risk factor and the need for worldwide prevention programsCurrent Hypertension Report 2013 15(3):134-36.10.1007/s11906-013-0340-923536128 [Google Scholar] [CrossRef] [PubMed]
[3]. Mendis S, O’Brien E, Seedat YK, Yusuf S, Hypertension and diabetes: Entry points for prevention and control of global cardiovascular epidemicInternational Journal of Hypertension 2013 2013:878460http://dx.doi.org/10.1155/2013/87846010.1155/2013/87846023653856 [Google Scholar] [CrossRef] [PubMed]
[4]. Mahajan R, Joint National Committee 8 report: How it differs from JNC7International Journal of Applied and basic Medical Research 2014 4(2):61-62.10.4103/2229-516X.13677325143876 [Google Scholar] [CrossRef] [PubMed]
[5]. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010Lancet 2012 380(9859):2224-60.10.1016/S0140-6736(12)61766-8 [Google Scholar] [CrossRef]
[6]. Slade AN, Kim H, Dietary responses to a hypertension diagnosis: evidence from National health and nutrition Examination Survey(NHANES) 2007-2010Behavioral Medicine 2014 40(1):01-13.10.1080/08964289.2013.82617124512360 [Google Scholar] [CrossRef] [PubMed]
[7]. Anchala R, Kannuri NK, Pant H, Khan H, Franco FH, Angelantonio ED, Prabhakaran D, Hypertension in India: a systematic review and meta-analysis of prevalence, awareness, and control of hypertensionJournal of Hypertension 2014 32(6):1170-77.10.1097/HJH.000000000000014624621804 [Google Scholar] [CrossRef] [PubMed]
[8]. Brewster LM, Mairuhu G, Bindraban NR, Koopmans RP, Clark JF, Montfrons GA, Creatine Kinase activity is associated with blood pressureCirculation 2006 114:2034-39.10.1161/CIRCULATIONAHA.105.58449017075013 [Google Scholar] [CrossRef] [PubMed]
[9]. Ferreira LG, Role of phosphocreatine system on energetic homeostasis in skeletal and cardiac musclesEinstein 2014 12(1):126-31.10.1590/S1679-45082014RB2741PMC4898252 [Google Scholar] [CrossRef] [PubMed]
[10]. Johnsen SH, Lilleng H, Wilsgaard T, Bekkelund SI, Creatine kinase activity and blood pressure in a normal population: the Tromsø studyJournal of Hypertension 2011 29(1):36-42.10.1097/HJH.0b013e32834068e021063205 [Google Scholar] [CrossRef] [PubMed]
[11]. Johnsen SH, Lilleng H, Bekkelund SI, Creatine kinase as predictor of blood pressure and hypertension. Is it all about body mass index? A follow-up study of 250 patientsThe Journal of Clinical Hypertension 2014 16(11):820-26.10.1111/jch.1242225279588 [Google Scholar] [CrossRef] [PubMed]
[12]. Brewster LM, Mairuhu G, Stronks K, Bindraban N, Clark JF, Montfrans GA, Serum creatine kinase as a marker of energetic capacity to create high blood pressureJournal of Hypertension 2003 21(4):98-99. [Google Scholar]
[13]. Oudman I, Kewalbansingh PV, Valkengoed I, Zwinderman AH, Clark JF, Montfrans GA, Creatine kinase is associated with failure of hypertension treatmentJournal of Hypertension 2013 31(5):1025-31.10.1097/HJH.0b013e32835f5c2923466941 [Google Scholar] [CrossRef] [PubMed]
[14]. Brewster LM, Clark JF, van Montfrans GA, Is greater tissue activity of creatine kinase the genetic factor increasing hypertension risk in black people of sub-Saharan African descent?Journal of Hypertension 2000 18(11):1537-44.10.1097/00004872-200018110-0000211081764 [Google Scholar] [CrossRef] [PubMed]
[15]. Schumann G, Bonora R, Ceriotti F, Clerc-Renaud P, Ferrero CA, IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37°C Part 2. Reference Procedure for the measurement of catalytic concentrations of creatine kinaseClinical Chemistry and laboratory Medicine 2002 40(6):635-42.10.1515/CCLM.2002.11012211662 [Google Scholar] [CrossRef] [PubMed]
[16]. Brewster LM, Bree S, Reijneveld JC, Noterman NC, Verschuren WM, Clark JF, Hypertension risk in idiopathic hyperCKemiaJournal of Neurology 2008 255(1):11-12.10.1007/s00415-008-0651-y18204808 [Google Scholar] [CrossRef] [PubMed]
[17]. Karamat FA, Oudman I, Stalpers CR, Afink GB, Keijser R, Clark JF, Resistance Artery creatine kinase mRNA and blood pressure in humansHypertension 2014 63(1):68-73.10.1161/HYPERTENSIONAHA.113.0135224126179 [Google Scholar] [CrossRef] [PubMed]
[18]. Taherzadeh Z, Karamat FA, Ankum WM, Clark JF, van Montfrans GA, van Bavel E, The effect of creatine kinase inhibition on contractile properties of human resistance arteriesAmerican Journal of Hypertension 2016 29(2):170-77.10.1093/ajh/hpv07826048947 [Google Scholar] [CrossRef] [PubMed]
[19]. Brewster LM, Mairuhu G, Ganzeboom K, Dijk Gert NV, Montfrans VA, Low creatine kinase is associated with a high population incidence of faintingClinical Autonomic Research 2009 19(4):231-36.10.1007/s10286-009-0013-619468786 [Google Scholar] [CrossRef] [PubMed]
[20]. Baird MF, Graham SM, Baker JS, Bickerstaff GF, Creatine-Kinase- and exercise-related muscle damage implications for muscle performance and recoveryJournal of Nutrition and Metabolism 2012 2012:960363doi:10.1155/2012/96036310.1155/2012/96036322288008 [Google Scholar] [CrossRef] [PubMed]
[21]. Dua S, Bhuker M, Sharma P, Dhall M, Kapoor S, Body mass index relates to blood pressure among adultsNorth American Journal of Medical Sciences 2014 6(2):89-95.10.4103/1947-2714.12775124696830 [Google Scholar] [CrossRef] [PubMed]
[22]. Oudman I, Jagernath Z, Kewalbansing P, Clark J, Van Montfrans G, Brewster L, Creatine kinase is associated with obesity in the general populationJournal of Hypertension 2011 (29):22010.1097/00004872-201106001-00607 [Google Scholar] [CrossRef]
[23]. Pisoni R, Hamrahian M, Fulop T, Creatine kinase, sodium retention, and blood pressure: Is there a link?Journal of Clinical Hypertension 2018 20(2):342-44.10.1111/jch.1317729357195 [Google Scholar] [CrossRef] [PubMed]