Anatomic Landmarks to Identify the Radial Nerve during the Posterior Approach of the Humerus: A Cadaveric Study
Mythraeyee Prasad1, Bina Isaac2, Prasanna Samuel Premkumar3
1 Assistant Professor, Department of Anatomy, Christian Medical College, Vellore, Tamil Nadu, India.
2 Professor, Department of Anatomy, Christian Medical College, Vellore, Tamil Nadu, India.
3 Lecturer, Department of Biostatistics, Christian Medical College, Vellore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bina Isaac, Professor, Department of Anatomy, Christian Medical College, Bagayam, Vellore-632002, Tamil Nadu, India.
E-mail: isaac@cmcvellore.ac.in
Introduction
Identification of the radial nerve and preventing injury to it is crucial, while surgically approaching the humerus from the posterior aspect to treat fractures of the midshaft or the distal third of the bone.
Aim
To identify certain anatomic landmarks, using which the radial nerve could be identified during surgical intervention, in order to prevent iatrogenic injury to the nerve.
Materials and Methods
Twenty-eight arms belonging to 14 adult cadavers (10 male and 4 female) were used for this study. The distance between the radial nerve on the posterior humerus and the point of confluence of the long and lateral heads of the triceps with the triceps aponeurosis was measured. Statistical analysis using Student’s paired t-test was done between the right and left sides. In the distal third of the humerus, the distance of the radial nerve and the lateral border of the triceps aponeurosis at four sites were determined.
Results
The mean distance from the point of confluence to the radial nerve along the posterior humerus was 39.7±11.8 mm. The radial nerve passed adjacent to the lateral border of the triceps aponeurosis at a distance of 12-19.5 (±3.27) mm. It was never found to be closer than 4.6±2.54 mm to the aponeurosis.
Conclusion
The present study is useful for orthopaedicians while undertaking the surgical management of humeral fractures. The point of confluence and the triceps aponeurosis are two anatomic landmarks that can be used to locate the radial nerve.
Humeral fracture, Posterior approach to humerus, Triceps aponeurosis
Introduction
The radial nerve is the largest terminal branch of the posterior cord of brachial plexus and it has a root value C5, C6, C7, C8, T1. It lies behind the third part of axillary artery. Branches for long head, medial head of triceps brachii and posterior cutaneous nerve of arm arise from the radial nerve in axilla. It passes posteriorly through the triangular space accompanied by the profunda brachii artery. Branches for lateral and medial heads of triceps brachii are given off at the spiral groove. The other branches at this level are branch to anconeus passing through the medial head of triceps, lower lateral cutaneous nerve of arm and posterior cutaneous nerve of forearm. The radial nerve pierces the lateral intermuscular septum at the lower lateral aspect of humerus and enters the anterior compartment of the arm. It divides into its terminal branches which are the superficial and deep branch anterior to the lateral epicondyle of humerus [1].
Fractures of the shaft of the humerus and its operative fixation can result in radial nerve injury [2,3]. Radial nerve palsy is commonly seen in Holstein Lewis fracture, as these fractures involve the middle and middle-distal shaft of the humerus [4].
A posterior approach to the humerus is commonly used for open reduction and internal fixation of fracture shaft of the humerus [5]. Bony landmarks like the medial humeral epicondyle, lateral humeral epicondyle, and distal articular surface of humerus have been made use of in the past to identify the radial nerve during surgical exploration of the humerus [6-10].
In cases where the bony elements have lost their proper orientation as in comminuted fractures, humeral malunion/non-union, other landmarks need to be taken into consideration to prevent iatrogenic injury to the nerve [11,12]. In fractures of the distal part of shaft of humerus, surgeons may find it difficult to locate the radial nerve intraoperatively using osseous points [13]. It has been seen that the landmark of the confluence of the long and lateral heads of the triceps with the triceps aponeurosis, can be used to identify the radial nerve when exploring the midshaft of the humerus with the triceps-splitting approach [12]. In such cases, the radial nerve can be identified using the triceps aponeurosis, as the nerve has a consistent relationship with the lateral border of the aponeurosis [10]. Chaudhry T et al., and McCann PA et al., studied the relationship between the radial nerve and the lateral border of the triceps aponeurosis in British cadavers [10,14]. There are no corresponding values for the Indian population.
The present study was aimed to determine reliable anatomic landmarks that can be used for identification of the radial nerve while undertaking surgical exploration of the humerus using the posterior approach.
Materials and Methods
The present study was done on 28 arms belonging to 14 adult formalin embalmed cadavers (male-10, female-4) available in the Department of Anatomy, Christian Medical College, Vellore, Tamil Nadu, India, where in the average age of the cadavers was 73 years (range 44-90 years). Arms having any gross malformation or deformity were excluded from the study. The study was started in March 2015 and completed in February 2016 and was approved by the Institutional Review Board (letter no. 9241 dated 12.01.2015).
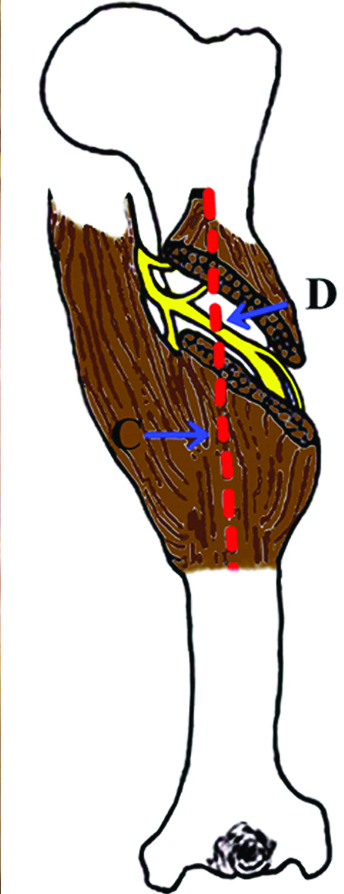
For each dissection, the cadaver was placed in a prone position on the dissection table. Both arms were placed in an extended position. An incision was made from the tip of the acromion process to the superior aspect of the olecranon process. The skin and subcutaneous tissues were removed. The intramuscular septum between the long and lateral heads of the triceps muscle was identified. The intersection of this septum with the triceps aponeurosis was identified (point C) [Table/Fig-1,2]. Blunt dissection through the triceps musculature at a level two finger breadths proximal to the point C was performed and the radial nerve was identified lying on the periosteum of the posterior humerus. The distance between the point C and the radial nerve (point D) was measured [Table/Fig-2].
Posterior view of right arm showing the point of confluence of long head of triceps, lateral head of triceps and triceps aponeurosis.
C: Point of confluence; Long H: Long head; Lat H: Lateral head

Point of confluence (C) and the position of the radial nerve on the posterior aspect of the mid axial humerus (D).
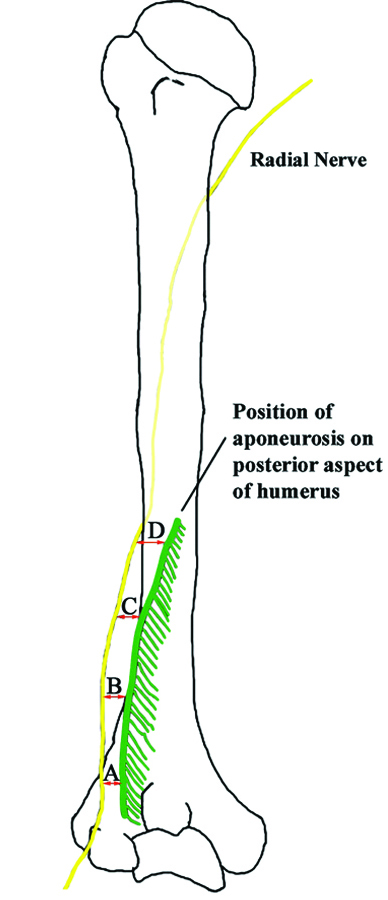
The lateral border of the triceps aponeurosis was identified and the radial nerve was exposed over the distal length of its course by dissecting the overlying muscle with a sharp scalpel [Table/Fig-3]. This ensured that the positions of the radial nerve and the triceps aponeurosis remained unaltered during the exposure. The distance between the radial nerve and the lateral margin of the triceps aponeurosis at four equally spaced points along the length of the aponeurosis was measured [Table/Fig-4]. The measurements were taken twice using a digital calliper (resolution of 0.01 mm) and the average of the values was taken.
Posterior view of the left humerus showing the Radial Nerve (RN) and the Triceps Aponeurosis (TA).

Measurements of the radial nerve in relation to the triceps aponeurosis.
A: Aponeurosis1/4 to nerve; B; Aponeurosis 2/4 to nerve; C: Aponeurosis 3/4 to nerve; D: Aponeurosis 4/4 to nerve
Statistical Analysis
The statistical analysis was done using SPSS version 16.0. Descriptive statistics like range, mean, standard deviation were evaluated for all the parameters studied. Paired t-test was used to assess differences in parameters between left and right sides.
Results
The mean distance from the point of confluence to the radial nerve along its posterior anatomic location was 39.7±11.8 mm {range 17.1-61.9 mm; [Table/Fig-5]}. Mean distances for the right and left humerus groups were 39.3±11.5 mm (range, 20.1-57.4 mm) and 40.1±12.6 mm (range, 17.1-61.9 mm) respectively. Statistical analysis of the right and left sides using student’s paired t-test revealed no significant differences (p-value=0.8).
Distance from the point of confluence to the radial nerve.
| Matched Pairs | Right (mm) | Left (mm) | p-value |
|---|
| 1 | 27.14 | 23.41 | |
| 2 | 20.06 | 47.25 | |
| 3 | 30.38 | 25.41 | |
| 4 | 30.34 | 47.54 | |
| 5 | 37.81 | 33.78 | |
| 6 | 32.72 | 38.56 | |
| 7 | 42.05 | 44.42 | |
| 8 | 53.68 | 53.13 | |
| 9 | 39.63 | 35.42 | |
| 10 | 40.68 | 37.63 | |
| 11 | 32.45 | 17.1 | |
| 12 | 57.37 | 54.72 | |
| 13 | 55.88 | 61.86 | |
| 14 | 50.13 | 41.69 | |
| Mean (SD) | 39.3 (11.5) | 40.1 (12.6) | 0.8 |
| Overall mean (SD) | 39.7 (11.8) | |
The distances between the radial nerve and the lateral border of the triceps aponeurosis at four equally spaced points are shown in [Table/Fig-6]. Throughout the course of its relationship with the triceps aponeurosis, the mean distance of the radial nerve from the aponeurosis was over 10 mm with a range of 12-19.5±3.27 mm. The closest distance between the radial nerve and the aponeurosis was found to be 4.6±2.54 mm.
Measurements of radial nerve in relation to triceps aponeurosis.
| Parameter | Mean distance±SD (mm) | Range (mm) |
|---|
| A: Aponeurosis to nerve 1/4 | 19.5±5.5 | 10.4-29.6 |
| B: Aponeurosis to nerve 2/4 | 15.3±4.2 | 6.9-24.6 |
| C: Aponeurosis to nerve 3/4 | 13.3±4 | 5.5-23.4 |
| D: Aponeurosis to nerve 4/4 | 12±4 | 4.6-23 |
Discussion
The course of the radial nerve has been extensively documented [1,5,15]. The nerve has a long and tortuous course, and because of its closeness to the humerus, it often sustains the injury in fractures of the humerus [16,17]. Humeral shaft fractures account for about 1-3% of all fractures [18] and radial nerve is the most commonly injured nerve following a humeral fracture (2% to 17% of cases) [19,20].
The management of humeral fractures depend on the type of injury and individual patient needs. Fractures like comminuted and spiral fractures of the humerus require early surgical exploration [21]. Surgical treatment is indicated in cases when nerve transaction is obvious, as in open injuries or when there is no clinical improvement after a period of three to six months of conservative treatment [16,22,23]. Proper identification and protection of the radial nerve during surgery may prevent secondary nerve palsy. Improper plate fixation can result in transaction of the radial nerve by screws [24]. Patients with distal fractures and those with previous fracture implants are at increased risk of iatrogenic radial nerve palsy [25].
The Posterior approach of the humerus provides good exposure to both middle and distal 1/3 humeral shaft fractures. A modified posterior approach is used in the surgical treatment of extra-articular distal-third diaphyseal fractures of the humerus [26]. It is possible that the more extensive radial nerve exploration, mobilisation, and manipulation required for this approach leads to a higher risk of radial nerve injury [25].
Although various studies have been done to determine the relationship between the radial nerve and bony landmarks [Table/Fig-7] [6-10], in cases where there is a fracture and displacement of the bony elements, a soft tissue landmark will prove useful to the orthopaedician to identify the radial nerve, and prevent potential iatrogenic injury. There are certain studies describing the relationship of the radial nerve to soft tissue landmarks like the apex of the triceps aponeurosis, triceps tendon and the point of confluence [Table/Fig-8] [12,27,28]. The point of confluence is an easily identifiable superficial landmark. In the present study of 28 arms, the distance of the radial nerve from the point of confluence was measured and it was found to be 39.7±11.8 mm. This finding is in accordance with the finding of Seigerman DA et al., in which the study of 30 arms reported that the radial nerve was at a mean distance of 39.0±2.1 mm from the point of confluence [Table/Fig-8] [12].
Position of radial nerve in relation to bony landmarks [6-10].
| Population | N | Landmark | Distance between radial nerve and bony landmark |
|---|
| Guse TR et al., [6] | American | 24 | Medial epicondyle to upper margin of spiral groove | 181±11 mm |
| Medial epicondyle to lower margin of spiral groove | 131±10 mm |
| Lateral epicondyle to lower margin of spiral groove | 126±11 mm |
| Gerwin M et al., [7] | American | 10 | Medial epicondyle | 20.7±1.2 cm |
| Lateral epicondyle | 14.2±0.6 cm |
| Uhl RL et al., [8] | American | 75 | Distal articular surface of humerus | 15.8±1.1 cm (men)15.2±1.1 cm (women) |
| Carlan D et al., [9] | American | 27 | Lateral epicondyle to upper margin of spiral groove | 17.1±1.6 cm |
| Lateral epicondyle to lower margin of spiral groove | 10.9±1.5 cm |
| Chaudhry T et al., [10] | British | 55 | Lateral epicondyle to upper margin of spiral groove | 156±1.3 mm |
| Lateral epicondyle to lower margin of spiral groove | 111±1.2 mm |
Position of radial nerve in relation to soft tissue landmarks [2,27,28].
| Population | N | Landmark | Distance between radial nerve and soft tissue landmark |
|---|
| Arora S et al., [27] | Indian | 10 | Apex of triceps aponeurosis | 2.51±0.2 cm |
| Seigerman DA et al., [12] | American | 30 | Point of confluence | 39.0±2.1 mm |
| Hasan SA et al., [28] | American | 33 | Triceps tendon | 2.3±1.7 cm |
| Present study 2016 | Indian | 28 | Point of confluence | 39.7±11.8 mm |
The triceps aponeurosis has been found to be a useful and reliable guide to locate the radial nerve intraoperatively. Chaudhry T et al., in their study of the relationship of the radial nerve to the triceps aponeurosis found that the nerve coursed at a distance of 22–27 (±2) mm from the lateral border of the aponeurosis in the British population [10]. It was never found to be closer than 13 (±1) mm to the aponeurosis. The area which is <10 mm from the aponeurosis represented a “safe” area for intervention. In the present study in the Indian population, the radial nerve was found at a distance of 12-19.5 (±3.2) mm from the lateral border of the aponeurosis. It was never found to be closer than 4.6 (±2.54) mm to the aponeurosis. The differences seen are because of racial variations. The area immediately adjacent to the aponeurosis (<4 mm) can be considered “safe” for soft tissue dissection and advancement to bone. Knowledge of these “safe zones” could potentially be useful for intraoperative guidance and might contribute to reduce the risk of radial neuropathy.
Limitation
The present study was done to offer a simple and safe procedure to identify the radial nerve during fixation of comminuted fractures of the humeral shaft using a posterior approach. The study was undertaken on embalmed upper limbs in one position only with the axial rotation of the arm and the level of flexion or extension at the elbow fixed. In the operative setting, there is more mobility within the arm as well as glide between separate tissues. Thus further studies in non-preserved cadaver specimens or surgical settings would be needed to confirm whether the exact position of the arm and forearm are critical to present findings. However, the consistency of the results obtained suggests that the point of confluence and triceps aponeurosis may provide useful guides to surgical approaches. Other limitations of the present study was the small sample size and the fact that gender variations have not been looked at in this study.
Conclusion
Preserving the integrity of the radial nerve is of paramount importance and in cases where the bony reference points are displaced, the point of confluence between the long and lateral heads of the triceps and the triceps aponeurosis serves as a reliable landmark to locate the radial nerve during operative fixation from a posterior approach. While exploring fractures of the distal third of the shaft of humerus, the lateral border of the triceps aponeurosis can be used as a landmark to trace the radial nerve and prevent iatrogenic injury to the nerve.
[1]. Standring S, Gray’s Anatomy: the anatomical basis of clinical practice 2016 41st edEdinburgChurchill Livingstone/ Elsevier:783 [Google Scholar]
[2]. Crenshaw AH, Perez EA, Fractures of the shoulder, arm and forearm, In: Canale ST, editorCampbell’s Operative Orthopaedics 1992 Vol 311th edPhiladelphaMosby:3397-98. [Google Scholar]
[3]. Rockwood CA Jr, Gree DP, Bucholz RW, Heckman JD, Rockwood and Green’s Fracture in Adults 1996 4th edPhiladelphiaLippincott-Raven Publishers:1043-45. [Google Scholar]
[4]. Shao YC, Harwood P, Grotz MR, Limb D, Giannoudis PV, Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic reviewJ Bone Joint Surg Br 2005 87:1647-52.10.1302/0301-620X.87B12.1613216326879 [Google Scholar] [CrossRef] [PubMed]
[5]. Ebraheim NA, Andreshak TG, Yeasting RA, Saunders RC, Jackson WT, Posterior extensile approach to the elbow joint and distal humerusOrthop Rev 1993 22:578-82. [Google Scholar]
[6]. Guse TR, Ostrum RF, The surgical anatomy of the radial nerve around the humerusClin Orthop Relat Res 1995 320:149-53.10.1097/00003086-199511000-00025 [Google Scholar] [CrossRef]
[7]. Gerwin M, Hotchkiss RN, Weiland AJ, Alternative operative exposures of the posterior aspect of the humeral diaphysis with reference to the radial nerveJ Bone Joint Surg Am 1996 78:1690-95.10.2106/00004623-199611000-000088934483 [Google Scholar] [CrossRef] [PubMed]
[8]. Uhl RL, Larosa JM, Sibeni T, Martino LJ, Posterior approaches to the humerus: when should you worry about the radial nerve?J Orthop Trauma 1996 10(5):338-40.10.1097/00005131-199607000-000088814575 [Google Scholar] [CrossRef] [PubMed]
[9]. Carlan D, Pratt J, Patterson JMM, Weiland AJ, Boyer MI, Gelberman RH, The radial nerve in the brachium: an anatomic study in human cadaversJ Hand Surg Am 2007 32:1177-82.10.1016/j.jhsa.2006.07.00117923300 [Google Scholar] [CrossRef] [PubMed]
[10]. Chaudhry T, Noor S, Maher B, Bridger J, The surgical anatomy of the radial nerve and the triceps aponeurosisClin Anat 2010 23:222-26.10.1002/ca.2090320014401 [Google Scholar] [CrossRef] [PubMed]
[11]. Browner BD, Jupiter JB, Levine AM, Trafton P, Krettek C, Skeletal Trauma 2008 4th edPhiladelphiaElsevier [Google Scholar]
[12]. Seigerman DA, Choung EW, Yoon RS, Lu M, Frank MA, Gaines LRJ, Identification of the radial nerve during the posterior approach to the humerus: a cadaveric studyJ Orthop Trauma 2012 26(4):226-28.10.1097/BOT.0b013e31821d020021918485 [Google Scholar] [CrossRef] [PubMed]
[13]. Kamineni S, Ankem H, Patten DK, Anatomic relationship of the radial nerve to the elbow joint: clinical implications of safe pin placementClin Anat 2009 22:684-88.10.1002/ca.2083119637299 [Google Scholar] [CrossRef] [PubMed]
[14]. McCann PA, Smith GC, Clark D, Amirfeyz R, The tricipital aponeurosis-a reliable soft tissue landmark for humeral platingHand Surg 2015 20(1):53-58.10.1142/S021881041550007025609275 [Google Scholar] [CrossRef] [PubMed]
[15]. Hollinshead WH, Anatomy for Surgeons 1982 3rd edNew YorkHarper and Row:376-379. [Google Scholar]
[16]. Bumbasirevic M, Palibrk T, Lesic A, Atkinson H, Radial nerve palsyEFORT Open Rev 2017 1(8):286-94.10.1302/2058-5241.1.00002828461960 [Google Scholar] [CrossRef] [PubMed]
[17]. Ljungquist KL, Martineau P, Allan C, Radial nerve injuriesJ Hand Surg Am 2015 40(1):166-72.10.1016/j.jhsa.2014.05.01025442768 [Google Scholar] [CrossRef] [PubMed]
[18]. Strohm PC, Reising K, Hammer T, Sudkamp NP, Jaeger M, Schmal H, Humerus shaft fractures-where are we today?Acta Chir Orthop Traumatol Cech 2011 78(3):185-89. [Google Scholar]
[19]. Niver GE, Ilyas AM, Management of radial nerve palsy following fractures of the humerusOrthop Clin North Am 2013 44(3):419-24.10.1016/j.ocl.2013.03.01223827843 [Google Scholar] [CrossRef] [PubMed]
[20]. Rocchi M, Tarallo L, Mugnai R, Adani R, Humerus shaft fracture complicated by radial nerve palsy: Is surgical exploration necessary?Musculoskelet Surg 2016 100(Suppl 1):53-60.10.1007/s12306-016-0414-327900704 [Google Scholar] [CrossRef] [PubMed]
[21]. Yeşil M, Özcan Ö, Kaya ÖA, Erginoğlu SE, Atypical injury of radial nerve after humeral shaft fractureEklem Hastalik Cerrahisi 2017 28(2):132-36.10.5606/ehc.2017.5519628760131 [Google Scholar] [CrossRef] [PubMed]
[22]. Korompilias AV, Lykissas MG, Kostas-Agnantis IP, Vekris MD, Soucacos PN, Beris AE, Approach to radial nerve palsy caused by humerus shaft fracture: is primary exploration necessary?Injury 2013 44(3):323-26.10.1016/j.injury.2013.01.00423352153 [Google Scholar] [CrossRef] [PubMed]
[23]. Li Y, Ning G, Wu Q, Wu Q, Li Y, Feng S, Review of literature of radial nerve injuries associated with humeral fractures-an integrated management strategyPLoS One 2013 8(11):e7857610.1371/journal.pone.007857624250799 [Google Scholar] [CrossRef] [PubMed]
[24]. Kinaci A, Kloen P, Videler A, Kreulen M, Unusual radial nerve injury by a locking compression plate for humerus fractureBMJ Case Rep 2014 2014pii: bcr2013201515. doi:10.1136/bcr-2013-20151510.1136/bcr-2013-20151524862412 [Google Scholar] [CrossRef] [PubMed]
[25]. Shoji K, Heng M, Harris MB, Appleton PT, Vrahas MS, Weaver MJ, Time from injury to surgical fixation of diaphyseal humerus fractures is not associated with an increased risk of iatrogenic radial nerve palsyJ Orthop Trauma 2017 31(9):491-96.10.1097/BOT.000000000000087528459772 [Google Scholar] [CrossRef] [PubMed]
[26]. Páramo-Díaz P, Arroyo-Hernández M, Rodríguez Vega V, Aroca-Peinado M, León-Baltasar JL, Caba-Doussoux P, Surgical treatment of extra-articular distal-third diaphyseal fractures of the humerus using a modified posterior approach and an extra-articular plateRev Esp Cir Ortop Traumatol 2017 61(6):404-11.10.1016/j.recote.2017.10.00228890121 [Google Scholar] [CrossRef] [PubMed]
[27]. Arora S, Goel N, Cheema GS, Batra S, Maini L, A method to localize the radial nerve using the ‘Apex of Triceps Aponeurosis’ as a landmarkClin Orthop Relat Res 2011 469:2638-44.10.1007/s11999-011-1791-421286885 [Google Scholar] [CrossRef] [PubMed]
[28]. Hasan SA, Rauls RB, Cordell CL, Bailey MS, Nguyen T, “Zone of Vulnerability” for Radial Nerve Injury: Anatomic StudyJournal of Surgical Orthopaedic Advances 2014 23(2):105-10.10.3113/JSOA.2014.0105 [Google Scholar] [CrossRef]