Calcaneal fractures include sixty percent of tarsal injuries and two percent of all the fractures [1]. Sixty-five to seventy percent of calcaneal fractures in adults are displaced intra-articular fractures [2]. Ten percent of patients with calcaneal fracture have spine fracture; twenty six percent are associated with other fractures of extremities [3]. Ninety percent of calcaneal fracture occurs in males between age group of 21 to 45 years and common in industrial workers, thus economic effects are substantial for this fracture [4].
Intra-articular displaced calcaneal fractures are commonly due to high velocity trauma like fall from height or road traffic accidents. The comminution and fracture type is based on porosity of the bone, amount of force and the position of foot at the time of injury [5].
The fracture type and the amount of soft tissue damage are directly related to the force and energy of the trauma. Swelling and hematoma is seen with low energy trauma but the high velocity trauma result in severe soft tissue injury and compound fracture [6].
On Lateral X-ray of the foot, two important angles can be drawn in the calcaneum–Bohler’s angle and Gissane angle. The Bohler’s angle normally ranges between 20 and 40 degrees [7]. In Indian population, it ranges between 18 and 43 degrees [8] [Table/Fig-1]. In a fractured calcaneum, a decrease in Bohler’s angle is seen on the lateral X-ray, which indicates that the posterior facet of the calcaneus has collapsed and hence shifting the body weight anteriorly [Table/Fig-2] [7].
Intra-articular fractures must be accurately reduced to obtain joint congruity. This is possible by the reduction of the articular surface with rigid internal fixation like plates and screws [2,9]. Some of the studies have correlated Bohler’s angle and functional outcome of displaced intra-articular calcaneal fractures and found no correlation [10-12]. This study was proposed to address whether surgical restoration of Bohler’s angle leads to improvement in outcome functionally.
Materials and Methods
This was a prospective cohort study done in Kasturba Medical College, Mangalore from September 2015 to August 2017. Inclusion criteria were skeletally mature patient with closed displaced intra-articular calcaneal fractures. Exclusion criteria were undisplaced fractures (sanders type 1), extra-articular fractures, comorbidities like diabetes, associated spine fractures with neurological deficits and open fractures. Forty consecutive patients who met the inclusion and exclusion criteria were enrolled in this study. Institutional ethical committee clearance (IEC KMC MLR 12-13/276) was taken for this study and informed consent was taken from all the enrolled patients.
All patients were screened by lateral and axial view radiographs. CT scan with 3D reconstruction was done to classify fractures according to Sander’s classification [13]. All patients were treated surgically after preoperative workup. All patients were operated by one surgical team. Patients received 1.5 grams of Cefuroxime 30 minutes before the procedure. Procedure was carried out under torniquet. Calcaneal fractures were operated with either of these methods: (1) Open reduction and fixation with plates and screws; (2) Essex Lopresti maneuver with and without CC screws; (3) Open reduction with CC screw fixation; and (4) percutaneous CC screw fixation. The surgery was aimed for anatomical reduction of fracture fragments and to improve the Bohler’s angle [Table/Fig-3]. Pre and postoperative Bohler’s angle were recorded by single person. Bohler’s angle consists of two lines: 1) Line drawn from highest part of the anterior process to the superior most point of the posterior facet; and 2) Line drawn tangentially to the superior point tuberosity of calcaneus [7]. The Bohler’s angle between 18-43 degrees was taken as normal range (mean=30.62 degrees) [8].
Post surgical restoration of Bohler’s angle.

Postoperatively patients were put on below knee posterior splint and was mobilized non-weight bearing with crutches. Partial weight bearing was allowed at 6 weeks and full weight bearing was allowed only after 4 months. They were evaluated clinically and radiologically at 6 weeks, 3months, 6 months and 1 year. Functional outcome was evaluated using AOFAS hind foot score and visual analogue score. AOFAS scoring system, developed by Kitaoka BH et al., combines subjective scores of pain and function provided by the patient with objective scores based on the surgeon’s physical examination of the patient [14]. The maximal score is 100 points, indicating no symptoms or impairments. A Visual Analogue Scale (VAS) is a unidimensional measure of pain intensity, which has been widely used in diverse adult populations [15]. In this study, patient is asked to grade the pain perceived by him/her on a scale of zero to ten. Zero represents no pain and ten represents worst pain.
Statistical Analysis
The data obtained were assessed using SPSS 16.0 for windows. The correlation between Bohler’s angle and AOFAS hind foot score, Bohler’s angle and VAS were analysed with bivariate correlation (Spearman’s rank correlation). According to Spearman correlation, rs value in the range of 0.9 to 1.0 is very strong correlation, 0.7 and 0.89 is strong correlation, between 0.5 and 0.69 moderate, 0.3 and 0.49 is moderate to low, 0.16 and 0.29 is weak to low and less than 0.16 is too low correlation [16]. A p-value less than 0.05 was considered statistically significant.
Results
Forty patients with displaced intra-articular calcaneal fractures were included in this study. Patients belonged to 18-65 years age group, with average age of 36.67 years and all were males. Thirty patients were manual laborers, six students and four electricians. The mechanism of injury included 35 patients with fall from height, three road traffic accident, two had injury due to fall of heavy object on foot. As per Sanders classification, the fracture type included 14 with type II fracture, 14 with type III and 12 with type IV. Average injury-surgery interval was seven days (ranged 2 -14 days). At the end of one year of follow up, the functional outcomes were excellent in one patient, good in 20 patients, fair in 15 and poor in four patients as per AOFAS hind foot score [Table/Fig-4]. Complications involving the soft tissue were seen in three patients with two having wound edge necrosis and one having superficial infection. These were resolved by regular dressing and antibiotics as per culture reports.
AOFAS hind foot score and Sanders classification.
| | AOFAS Score | | |
|---|
| >90 | (75-89) | (60-74) | <60 |
| Sanders type II | 1 | 7 | 5 | 1 |
| Sander type III | - | 8 | 4 | 2 |
| Sander type IV | - | 5 | 6 | 1 |
| Total (n=40) | Excellent-1 | Good-20 | Fair-15 | Poor-4 |
The average preoperative Bohler’s angle value was 13.60 (range 1.2–20 degrees). The average postoperative Bohler’s angle value was 21.80 (8.7–35.7 degrees range). For patients who got excellent, good, fair and poor results as per AOFAS hind foot score, the average postoperative Bohler’s angle were 23.06 degrees, 23.86 degrees (range 21.36–35.7 degrees), 20.56 degrees (range 8.7-24.18 degrees), 14.05 degrees (12.1-17.9 degrees) respectively.
The preoperative Bohler’s angle measurement did not correlate with AOFAS hind foot score and Visual analogue scale (rs=0.053, p-value=0.751 and rs value=0.075, p-value=0.648 respectively) [Table/Fig-5]. The postoperative Bohler’s angle had strong correlation with both AOFAS hind foot score and Visual analogue scale (mean 73.897, rs value=0.736, p-value=<0.001 and mean=3.15, rs value=-0.701, p-value=<0.001 respectively) [Table/Fig-5].
Correlation between Bohler’s angle and functional outcome score.
| Correlation | | rs value | p-value |
|---|
| Preoperative | Bohler’s angle | AOFAS score | 0.053 | 0.751 |
| Bohler’s angle | Visual analogue scale | 0.075 | 0.648 |
| Postoperative | Bohler’s angle | AOFAS score at 1 year | 0.736 | <0.001 |
| Bohler’s angle | Visual analogue scale | -0.701 | <0.001 |
Sperman’s rank correlation
Among the subjective variables in AOFAS hind foot scores, postoperative Bohler’s angle correlated with pain, activity limitations and walking surface (mean value= 3.256, rs = 0.692, p=<0.001; mean value=8.153, rs=0.434, p=0.005; mean value=4.282, rs=0.640, p=<0.001 respectively). There was no correlation with category of walking distance (mean value=5, rs=0.062, p=0.702). Moderate correlation was seen between postoperative Bohler’s angle and pain, walking surface categories, as the rs value was more than 0.5. Activity limitation category showed low correlation [Table/Fig-6].
Four subjective categories of AOFAS hind foot scores and postoperative Bohler’s angle correlation.
| Correlation | | rs value | p-value |
|---|
| Pain | Bohler’s angle | 0.692 | <0.001 |
| Activity Limitation | Bohler’s angle | 0.434 | 0.005 |
| Walking surface | Bohler’s angle | 0.640 | <0.001 |
| Walking distance | Bohler’s angle | 0.062 | 0.702 |
Spearman’s rank correlation
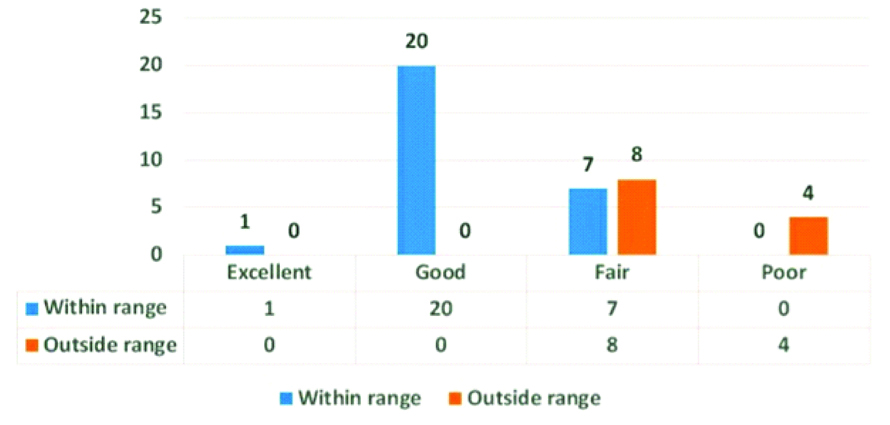
Surgical restoration of Bohler’s angle between the range 18-43 degree showed better functional outcome. When the postoperative Bohler’s angle was within 18-43 degrees range, one patient achieved excellent result, 20 patients achieved good results and seven patients achieved fair results. However, when postoperative Bohler’s angle was less than 18 degrees, none of the patients achieved excellent or good results but eight patients achieved fair result and four patients achieved poor results [Table/Fig-7].
Distribution of Bohler’s angle in different functional outcome groups.
Sanders fracture type was plotted with postoperative Bohler’s angle achieved [Table/Fig-8]. Eleven of the type II fractures were within the normal range and 3 were outside the range. Ten of type III fractures were within the range and 4 outside the range. Eight of type IV fractures were within the range and 4 were outside the range.
Postoperative Bohler’s angle in different fracture types.
| Bohler’s angle within range | Less than range |
|---|
| Type II | 11 | 3 |
| Type III | 10 | 4 |
| Type IV | 8 | 4 |
| Total n=40 | 29 | 11 |
Discussion
Bohler’s angle is a very useful tool in quantifying displacement of calcaneal fracture and 20° or less value is accurate in identifying the absence or presence of calcaneal fracture [17]. The effect of surgical restoration of Bohler’s angle to the normal range on the ultimate functional outcome has been debated. As per the study done by Loucks C et al., the maximum changes in the Bohler’s angle of injured feet showed poor functional outcome at 2 year follow up [18]. However, some of the studies showed no correlation between the good surgical restoration of Bohler’s angle and functional outcome [12,18-21]. Although, the number of operative patients in the above studies were less as compared to present study. Historically, intra-articular displaced calcaneal fractures were treated conservatively; however, surgical treatment of such fractures became more popular as fracture care improved [22]. Patients can be expected to benefit with open or closed reduction of fracture fixation in which anatomical fracture reduction can be achieved [23].
Bohler’s angle can be used as a tool to achieve articular congruity intraoperatively [24]. In the study by Paley D et al., the ratio of Bohler’s angle between injured and normal side was significantly less in patients with poor functional outcomes and hence they suggested that a decrease in this ratio is a poor prognostic factor [25].
Present study suggests that surgical restoration of Bohler’s angle to normal range result in good functional outcome. A strong correlation between postoperative Bohler’s angle and American Orthopaedic Foot & Ankle Society scores at the end of follow-up was seen. Restoring the Bohler’s angle at more than 18 degrees gave excellent to good results in this study. Bohler’s angle was found to correlate with three of the subjective categories of AOFAS hind foot score. When the postoperative Bohler’s angle was outside the range, the results were fair to poor. It was found that as the Sanders type increased, there was increase in number of patients in whom Bohler’s angle could not be restored to normal range. This shows that with increase severity of the fracture, it is difficult to restore the Bohler’s angle to the suggested range.
Limitation
The limitations of this study were different types of fixations used and short follow-up time. Merits and demerits of different fixation methods were not considered. other parameters like reduction quality of posterior articular surface that may influence the functional outcome were not considered. Results cannot be generalized because there were no female patients in the study. Therefore, long term studies involving larger sample size would be required to further substantiate these results.
Conclusion
The postoperative Bohler’s angle correlated strongly with the functional outcome and it is suggested Bohler’s angle to be restored >18 degrees.
Sperman’s rank correlation
Spearman’s rank correlation