Floating Canine in Maxillary Sinus – Case Report and Overview of Pathogenetic Literature
Ajay M Bhandarkar1, Shubhika Jain2, Adarsh Kudva3, Kailesh Pujary4
1 Associate Professor, Department of ENT, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
2 Undergraduate Student, Department of ENT, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
3 Assistant Professor, Department of Oral and Maxillofacial Surgery, Manipal College of Dental Sciences, Manipal Academy of Higher Education, Manipal, Karnataka, India.
4 Professor, Department of ENT, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ajay M Bhandarkar, Department of ENT, 4th Floor, Sharada Madhav Pai OPD, Kasturba Hospital, Manipal Academy of Higher Education, Manipal, Karnataka-576104, India.
E-mail: bm.ajay@gmail.com
The eruption of tooth other than the alveolar arch is called Ectopic Tooth. It is frequently encountered in the maxillary sinus. Facial pain is the most common presentation which is commonly misdiagnosed as chronic sinusitis. We present a case of a 47-year-old lady who was incidentally diagnosed to have an ectopic free lying canine in the maxillary sinus and discuss the various theories mentioned in literature predisposing to this condition.
Ectopic tooth, Endoscopic sinus surgery, Orthopantomogram, Toothache
Case Report
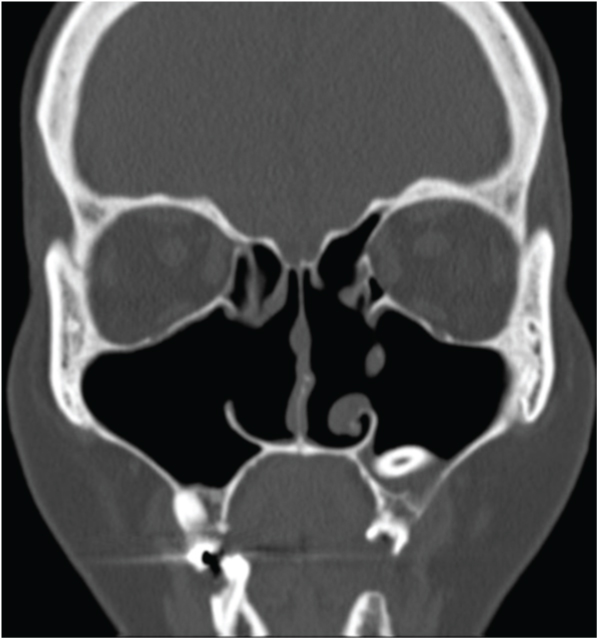
A 47-year-old lady presented to the ENT outpatient department with the chief complaints of pain in upper left back tooth region since three months. The pain was gradual in onset, progressive, moderate in intensity, diffuse nagging type, non-radiating with no aggravating and relieving factors. Intermittent swelling was present over the left malar area over three months with no discharge or bleeding from the site. No other nasal symptomatology was present. The patient had a previous history of endoscopic nasal surgery for chronic sinusitis three years prior to the current presentation. The postoperative period of the surgery was unremarkable. On oral examination, caries was noted in the left upper two premolars and first molar. Diagnostic nasal endoscopic examination revealed atrophic changes in the inferior turbinates on both sides with a septal perforation and postoperative endoscopic surgical cavities. Systemic examination was unremarkable. Orthopantomogram revealed presence of tooth like structure at apex, impacted horizontally in the floor of the maxillary sinus corresponding to the premolar area on the left side of upper jaw [Table/Fig-1]. No resorption of the adjacent structures was appreciated. Upper occlusal radiograph was also performed which revealed the presence of small cyst-like lesion with sclerotic borders with an impacted tooth in the left upper two premolars and first molar region which was reported as a possibility of a dentigerous cyst by radiology. Computed tomography of the paranasal sinuses revealed an ectopic tooth with horizontal alignment in the floor of the left maxillary sinus with mucosal thickening in the floor and the lateral wall of the left maxillary sinus without any evidence of cyst [Table/Fig-2,3]. Hence, a final diagnosis of ectopic canine in the maxillary sinus with atrophic rhinitis was made.
Orthopantomogram showing the presence of tooth like structure at apex, impacted horizontally in the floor of the maxillary sinus corresponding to the premolar area on the left side of upper jaw.

Axial CT section of the paranasal sinuses showing an ectopic tooth with horizontal alignment in the floor of the left maxillary sinus.

Coronal CT section of the paranasal sinuses demonstrating an ectopic tooth with surrounding mucosal thickening in the floor of the left maxillary sinus.
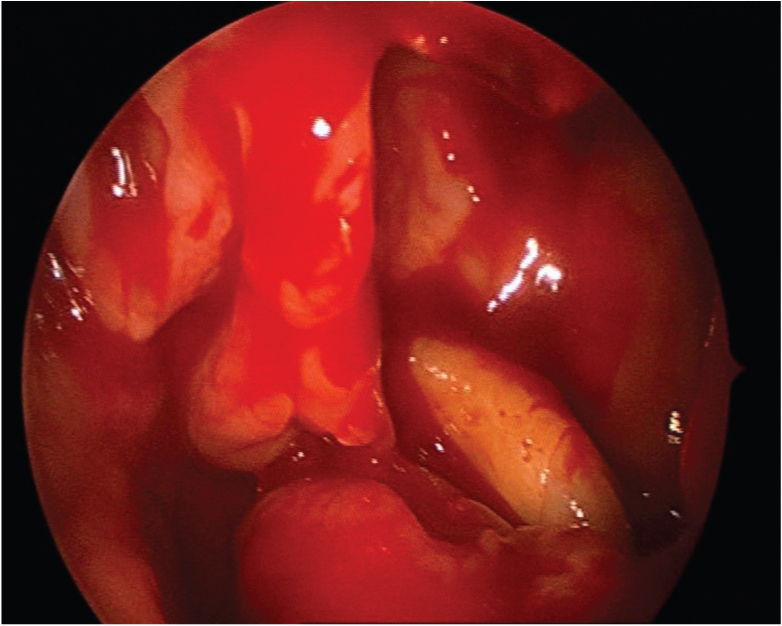
Based on the above investigations, extraction of the caries tooth was carried out. There was no evidence of cyst noted on extraction of teeth. Following this, the patient underwent left uncinectomy and endoscopic left middle meatal antrostomy under general anaesthesia. A freely lying canine tooth was observed in the floor of the left maxillary sinus with mucosal oedema [Table/Fig-4]. The canine was extracted from the maxillary sinus [Table/Fig-5].
Endoscopic image showing the presence of a freely lying intact canine tooth in the left maxillary sinus after uncinectomy and middle meatal antrostomy.
Canine tooth after removal from the maxillary sinus.

The patient also had atrophic turbinal changes in the nasal cavity owing to previous endoscopic nasal surgery which was confirmed by endoscopic examination. Patient is on regular follow-up for two years without any symptoms.
Discussion
The eruption of tooth other than the alveolar arch is called ectopic tooth. The most common reported sites for such presentation are maxillary sinus, nasal cavity, palate, mandibular condyle [1]. Aetiologic factors are challenging properties (such as radio opacity in Water’s view) in a patient with no sinusitis. Routine clinical evaluation and imaging lead to an incidental diagnosis, when patients are asymptomatic [2]. Definite aetiology is still unclear but several factors have been hypothesised to be the cause of this condition which has been discussed in this case report.
Ectopic canine is encountered infrequently [1,2]. The most common teeth to be encountered in ectopic location are the third molars [1]. Innumerable theories arising from varied aetiologies are mentioned in the literature which forms the crux of this discussion.
Trauma: This has been found to be the primary causative factor in ectopic teeth. This can predispose to the displacement of the tooth into the sinus or if it is sustained in infancy then it can predispose to ankylosis which leads to the development of an ectopic tooth. Traumatic tooth extraction could also be the cause for impaction of the tooth in the maxillary sinus [1,3].
Infections: Osteomyelitis of maxilla can cause displacement of teeth into the nasal cavity or into the maxillary sinus primarily due to the erosion of bone. Subsequently, the presence of ectopic teeth within the sinus can impede the mucociliary clearance and predispose to sinusitis [1,3].
Developmental Anomalies: Dental and skeletal anomalies have been proposed as the primary aetiology. Incompatibility between the volume of the dental arch and teeth is an aetiology mentioned in literature. Genetic predisposition in the form of an autosomal dominant trait has been mentioned as a causative factor. The presence of a cleft palate can result in the incomplete union of the embryonic processes leading to migration of teeth within the maxillary sinus. Aberrant extra-odontogenic epithelium within the sinus may also cause ectopic teeth [1-4].
Crowding of Teeth: Primary teeth retention for a prolonged duration of time can impede the gravitational development of secondary teeth predisposing it to protrude into the nasal cavity or the maxillary sinus. Mucosa may only be the barrier between the apex of teeth and the maxillary sinus floor which can also predispose to ectopic teeth development within the sinus [4].
The present patient had a history suggestive of an unerupted canine with caries of upper two premolar teeth and first molar tooth in the left upper jaw. Pre-existing dentigerous cyst displacing a tooth into the maxillary sinus is rare as noted in literature [5]. However, it was unlikely in the present case as the ectopic tooth was a canine and a small cystic pathology was noted around the premolars and first molar suggestive of inflammation which was relieved by extraction of teeth. Developmental anomaly maybe regarded as an important aetiological factor in the patient. The evidence of mucosal thickening on CT scan is due to the defective mucociliary clearance in the maxillary sinus owing to the presence of a tooth within the maxillary sinus.
Most of the patients are asymptomatic at presentation. The predominant presentation in symptomatic ectopic teeth is facial pain associated with nasal discharge due to recurrent maxillary sinusitis. Radicular cyst, ameloblastoma and odontogenic fibroma can be considered as a differential diagnosis [2].
Plain radiography of the paranasal sinus – Waters view, panoramic view of the teeth, lateral cephalometry and orthopantomogram are the imaging modalities which are sufficient to diagnose ectopic teeth. CT scan of the paranasal sinuses will provide clear cut evidence on the presence of sinusitis, cyst or mucocele [6-9]. The patient underwent an occlusal view, OPG and CT scan of the paranasal sinuses due to the non-availability of CBCT.
Treatment is limited to removal of teeth by endoscopic sinus surgical techniques or Caldwell-Luc surgery. If left untreated, an ectopic teeth may produce a cyst which can complicate in the form of nasolacrimal duct obstruction, sepsis, chronic headache and facial numbness [1,4,6,10]. Regular postoperative imaging is essential to rule out recurrences [11].
Conclusion
Ectopic teeth within the maxillary sinus are a rare condition which can be caused by various aetiological factors. It can be diagnosed incidentally or can be symptomatic mimicking a sinusitis. It is diagnosed by imaging and endoscopic sinus surgery is the treatment of choice.
Patient consent: Written and informed consent was obtained from the patient.
[1]. Baykul T, Doğru H, Yasan H, Çina Aksoy M, Clinical impact of ectopic teeth in the maxillary sinusAuris Nasus Larynx 2006 33(3):277-81.10.1016/j.anl.2006.01.00416675177 [Google Scholar] [CrossRef] [PubMed]
[2]. Dağistan S, Cakur B, Göregen M, A dentigerous cyst containing an ectopic canine tooth below the floor of the maxillary sinus:a case reportJ Oral Sci 2007 49(3):249-52.10.2334/josnusd.49.249 [Google Scholar] [CrossRef]
[3]. Alexandrakis G, Hubbell RN, Aitken PA, Nasolacrimal duct obstruction secondary to ectopic teethOphthalmology 2000 107(1):189-92.10.1016/S0161-6420(99)00023-8 [Google Scholar] [CrossRef]
[4]. Bodner L, Tovi F, Bar-Ziv J, Teeth in the maxillary sinus - imaging and managementJ Laryngol Otol 1997 111(9):820-24.10.1017/S00222151001387219373546 [Google Scholar] [CrossRef] [PubMed]
[5]. Mohan S, Kankariya H, Harjani B, Sharma H, Ectopic third molar in the maxillary sinusNatl J Maxillofac Surg 2011 2(2):222-24.10.4103/0975-5950.9448822639520 [Google Scholar] [CrossRef] [PubMed]
[6]. Sharma V, Lavania A, Mallick SA, Sharma M, Ectopic canine tooth: A rare cause for maxillary antral mucocoeleKathmandu Univ Med J 2006 4(2):251-52. [Google Scholar]
[7]. Datli A, Pilanci O, Cortuk O, Hospital T, Saglam O, Hospital KM, Ectopic tooth superiorly located in the maxillary sinusJ Craniofac Surg 2014 25(5):1927-28.10.1097/SCS.000000000000091425119397 [Google Scholar] [CrossRef] [PubMed]
[8]. Altas E, Karasen RM, Yilmaz AB, Aktan B, Kocer I, Erman Z, A case of a large dentigerous cyst containing a canine tooth in the maxillary antrum leading to epiphoraJ Laryngol Otol 1997 111(7):641-43.10.1017/S00222151001381989282204 [Google Scholar] [CrossRef] [PubMed]
[9]. Di Felice R, Lombardi T, Ectopic third molar in the maxillary sinus. Case reportAus Dent J 1995 40(4):236-37.10.1111/j.1834-7819.1995.tb04802.x7575278 [Google Scholar] [CrossRef] [PubMed]
[10]. Thakur G, Nair PP, Thomas S, Ahuja R, Kothari R, Dentigerous cyst associated with ectopic maxillary third molar in the maxillary antrumBMJ Case Rep 2011 2011:piibcr022011387310.1136/bcr.02.2011.387322696724 [Google Scholar] [CrossRef] [PubMed]
[11]. Ramanojam S, Halli R, Hebbale M, Bhardwaj S, Ectopic tooth in maxillary sinus: Case seriesAnn Maxillofac Surg 2013 3(1):89-92.10.4103/2231-0746.11007523662268 [Google Scholar] [CrossRef] [PubMed]