Introduction
Trapezius muscle pain and spasm is most common musculoskeletal disorder occurring in individuals who works with an awkward position of neck for a prolonged period of time, with repetitive movements. Active Release Therapy (ART) and Myofascial Release (MFR) are soft tissue manipulation techniques practiced by physiotherapists for reducing muscle spasm and pain.
Aim
To compare the effect of ART and MFR on the upper trapezius muscle spasm on pain and cervical range of motion.
Materials and Methods
The study was done on 60 patients of both genders between the age group of 20 to 55 years with upper trapezius spasm. They were divided into two groups by computerised randomisation. Each group received treatment in the form of either ART or MFR for seven days. Cervical Range of motion (ROM), Neck Disability Index scale (NDI) and Visual Analog Scale (VAS) were used as outcome measures.
Results
Paired Sample t-test was used to compare the outcome differences within each group, while Independent t-test was used to compare the differences between the two groups for the same outcome measures. Improvement was found in both the groups on seventh day following intervention, but the group which received ART showed significant improvements in neck ROM (p<0.001), NDI (p<0.0001) and in VAS (p<0.0001) as compared to group which received MFR.
Conclusion
Although both techniques are effective in alleviation of symptoms and associated disability in upper trapezius muscle spasm, ART gave better results as compared to MFR.
Neck disability index, Range of motion, Soft tissue manipulation, Trapezius pain
Introduction
Neck pain is the common problem in general population with prevalence between 10% and 15%. Population based surveys have shown lifetime prevalence of neck pain between 67% and 87% [1]. Work related neck pain is a major concern in the industrialised world. Even among adolescents, this trend is growing, posing future challenges to society [2-4], Pain symptoms are believed to worsen in response to prolonged static muscle activity and/or repetitive job tasks, which cause muscle metabolic disturbances [5,6].
Trapezius pain is a classic example of stress pain and the most common musculoskeletal disorder which leads to long and serious disability. The upper trapezius muscle being a postural muscle is highly susceptible to overuse [7,8]. Interruptions of low frequency in the muscle activity during repetitive tasks are associated with future development of neck pain. More recent studies have shown a correlation between trapezius muscle activation and pain [9,10]. Muscle spasm keeps the muscle continuously in contraction and this overload creates knot in the muscle. These are known as trigger points leading to pain [8,11]. Myofascial trigger point is most commonly found in the midpoint of upper border of trapezius [8]. Pain, stiffness and tenderness are felt on palpation in the belly and at paraspinal region [12]. Tightness in muscle reduces the range of neck movements as well as the mobility of the cervical joints. Neck pain and restricted movements give a subjective feeling of stiffness which further aggravate pain and ultimately leads to muscle spasm, increase in soft tissue tightness, with an ensuring pain–spasm cycle which can be difficult to break [7,12]. It is essential to provide relief and to improve the function.
Physiotherapy is the choice of treatment for trapezius spasm which includes passive treatment such as massage, stretching etc., along with various modalities like interferential therapy, transcutaneous Electrical Nerve Stimulation, Ultrasound, heat application, cryotherapy and active treatment such as exercise therapy. In addition, soft tissue manipulation techniques like Positional Release Therapy (PRT), Muscle Energy Technique (MET), ART, MFR etc., are also used for relief of muscle pain & spasm [1,13].
This study compared the effectiveness of two techniques i.e., ART and MFR. According to Austin Sports Therapy, ART was developed by chiropractor Dr. P. Michael Leahy to work on a variety of muscle, tendon, ligament, fascia and nerve issues. In this technique deep digital pressure is applied over the tender point (trigger point) in a shortened position of the muscle and then patient is asked to actively take it in an opposite lengthened position. This will break the adhesions [14,15].
Myofascial Release (MFR) is a soft tissue mobilisation technique. It can be defined as “the facilitation of mechanical, neural and psycho-physiological adaptive potential as interfaced via the myofascial system [8]. Robert Ward, an osteopath, is attributed with coining the term MFR in the 1960s. MFR therapy involves specifically guided low load, long duration mechanical forces to manipulate the myofascial complex, intended to restore optimal length, decrease pain, and improve function [13]. MFR utilises the manual traction and prolonged stretching of the fascia and muscle to break down the adhesions, thus helps to decrease the pain and increase flexibility and thereby increase ROM [16].
Literatures are available which shows the effectiveness of both the techniques either individually or with some other technique but there is dearth in the literature comparing the effectiveness between two techniques ART and MFR in patients with upper trapezius spasm [17]. Therefore, the aim of the study was to compare the effect of both techniques on range of motion, neck function and pain in upper trapezius spasm.
Materials and Methods
This was a randomised interventional study, Ethical approval was taken from the Human Research and Ethics Committee of HM Patel Centre for Medical care and Education (HMPCMCE: HREC/UGPG/23/Session 4/1 dated on 26/05/2014), Karamsad. CTRI registration number is CTRI//2018/02/011869.
Neck disability index was considered as the primary outcome for the study. A pilot study of 13 participants (not included in the study) revealed that the mean (SD) neck disability index was 20.22(5.01). Considering about five points difference between the two treatments as clinically important, we required a sample of size 28 per group at 5% alpha level and 80% power. Sixty participants of both genders between the age 20 to 55 years group who had upper trapezius spasm diagnosed clinically and referred for physiotherapy at Physiotherapy department were recruited for the study from June 2014 to February 2015. Participant having radiculopathy, neck and back deformities like torticollis or scoliosis, history of trauma or fracture or surgery in the neck or upper back or shoulder, any skin diseases in the trapezius area were excluded from the study.
They were divided into two groups, Group A and Group B, 30 each, through the computer randomisation. Group A received ART and group B received MRF. Neck ROM, NDI scale and VAS tools were used as outcome measures [18,19]. For application of ART, patient was made to sit on a stool with hands supported on the thighs. Therapist stood behind the patient stabilising the shoulder with one hand. Neck was taken in extension and contact was made using thumb with the trapezius muscle over the tender area and deep tension stretch was applied. Patient was then asked to flex and turn the neck. This was repeated for 3-5 times [14]. MFR was also applied with patient sitting on stool, arm supported on thighs. Therapist stood behind the patient close on the side to be treated. Forearm and/or ulnar border of the palm were used to apply the pressure and glide medially towards the base of the neck and/ or towards the upper scapular region. As the glide was given, patient was asked to do side bending and to turn the head in opposite direction while sitting in erect position. Glides were given for 3-4 times [8].
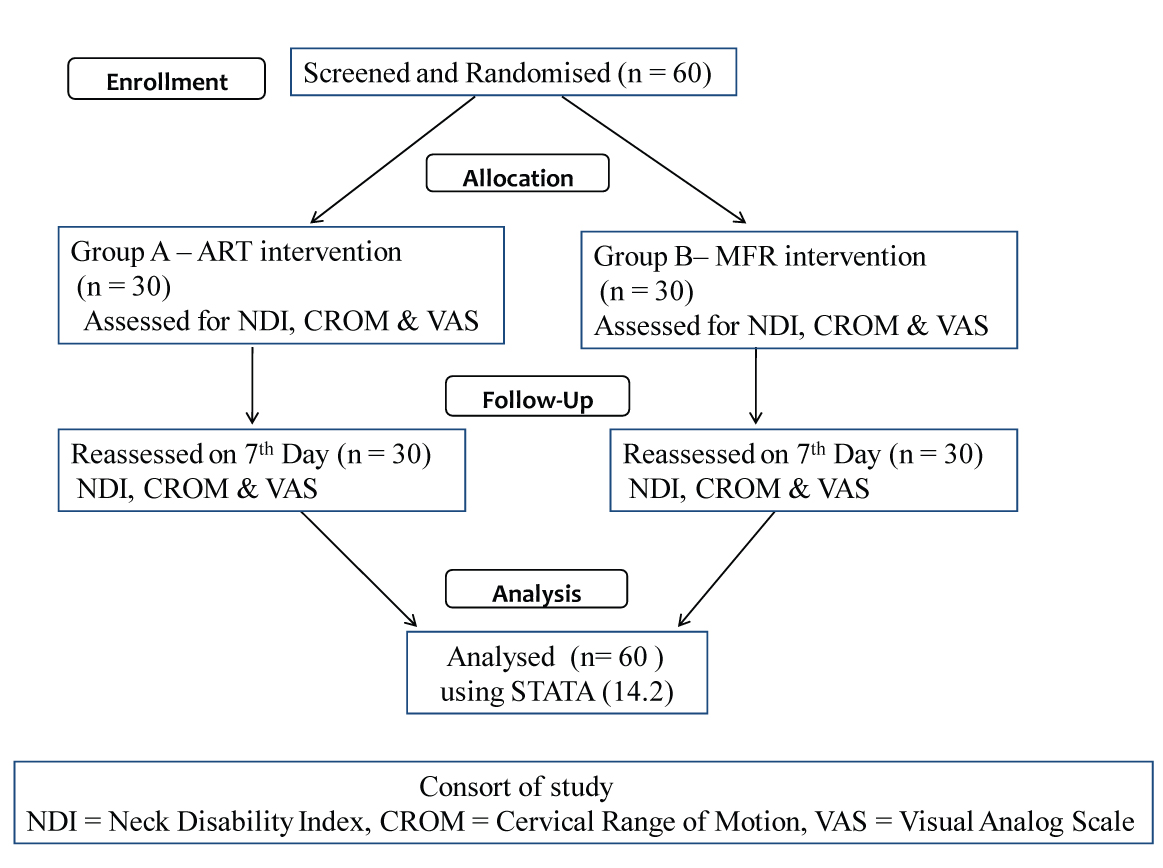
At the end of seventh day both the groups A and B were reassessed to check active cervical ROM using goniometer, functional ability of neck with NDI, the pain intensity of trapezius muscle with VAS. Data were recorded and both the groups were compared for its effect after seventh session of the treatment on seventh day on ROM, NDI & VAS [Table/Fig-1].
Statistical Analysis
Results were analysed using STATA (14.2). Descriptive statistics {mean (SD), frequency (%)} were used to depict the profile of study population. The improvement from the baseline was assessed using paired t-test in both groups (ART as well as MFR). The efficacy of the groups was compared using independent sample t-test on difference scores and p-value less than 0.05 with 95% Confidence Interval was considered statistically significant.
Results
The study comprised of 11 (37 %) male and 19 (61%) female in group A, while group B had 18 (62%) male and 12 (38%) female. The mean age of the patients affected in both the groups was 28.13±9.86 and 29.90±10.61 respectively.
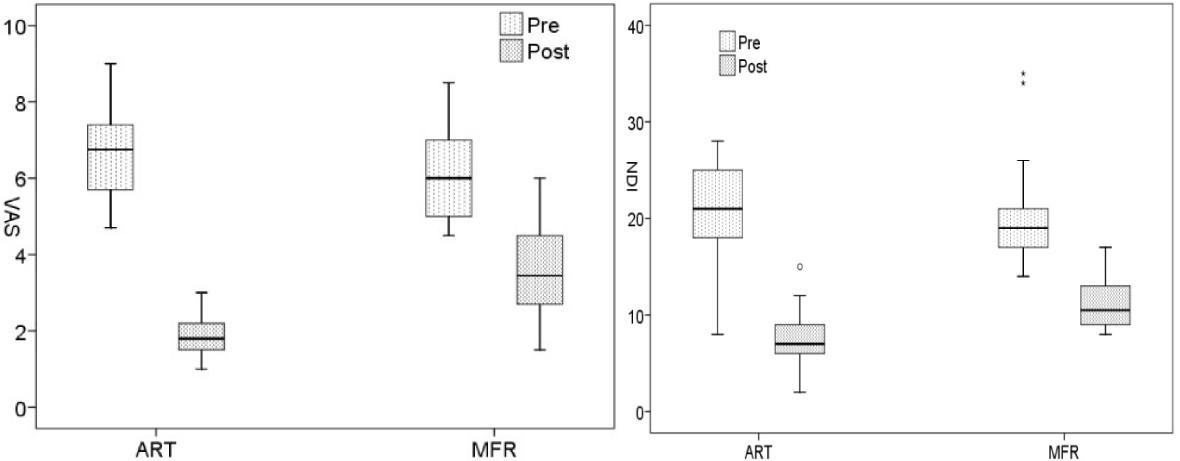
There was no baseline difference in all the parameters in both the groups. Both the techniques showed significant improvement [Table/Fig-2] in all the various parameters like cervical ROM, Neck functions NDI and pain on VAS but the improvement in all parameters were statistically higher in ART group as compared to MFR group. Difference of mean was stastically significant in ART versus MFR group for NDI (p <0.0001) and for VAS (p< 0.0001) [Table/Fig-3,4].
Intra group analysis of Cervical ROM, NDI, and VAS Scale for group A and B in patients with upper trapezius muscle spasm before treatment and after seven days of treatment.
| Outcomemeasures | | ARTMean (SD) | MFRMean (SD) |
|---|
| | PreTreatment | PostTreatment | Pairedt-testp-value | PreTreatment | PostTreatment | Pairedt-testp-value |
|---|
| ROM | Cervical Flexion | 30.97 (5.35) | 42.83 (3.73) | 0.0001 | 34.33 (4.82) | 39.97 (4.55) | 0.0001 |
| Cervical Extension | 19.60 (4.51) | 41.30 (3.37) | 0.0001 | 32.43 (6.53) | 38.53 (4.95) | 0.0001 |
| Cervical side flexion Rt | 33.17 (4.34) | 41.87 (3.36) | 0.0001 | 34.80 (4.94) | 40.53 (4.22) | 0.0001 |
| Cervical side flexion Lt | 30.07 (4.91) | 42.00 (2.89) | 0.0001 | 34.17 (5.7) | 40.30 (3.99) | 0.0001 |
| Cervical Rotation Rt | 48.97 (7.68) | 58.17 (2.45) | 0.0001 | 50.63 (5.35) | 56.13 (4.10) | 0.0001 |
| Cervical Rotation Lt | 48.23 (7.08) | 58.10 (3.33) | 0.0001 | 51.27 (6.64) | 56.73 (3.91) | 0.0001 |
| Neck Disability index | | 20.80 (5.12) | 7.47 (2.70) | 0.0001 | 19.80 (4.98) | 11.13 (2.69) | 0.0001 |
| Visual Analogue Scale | | 6.66 (1.14) | 1.86 (0.54) | 0.0001 | 6.10 (1.17) | 3.61 (1.26) | 0.0001 |
Inter group analysis of cervical ROM, NDI, VAS scale for group A and group B in patients with upper trapezius muscle spasm.
| GROUP A (ART) | GROUP B(MFR) | p-value |
|---|
| Mean of the difference | SD | Mean of the difference | SD |
|---|
| Cervical Flexion | 11.86 | 4.05 | 5.63 | 2.22 | <0.0001 |
| Cervical Extension | 11.70 | 4.05 | 6.10 | 4.02 | <0.0001 |
| Cervical side flexion (Right) | 8.70 | 3.78 | 5.73 | 2.65 | <0.001 |
| Cervical Side flexion (Left) | 11.93 | 4.77 | 6.13 | 4.00 | <0.0001 |
| Cervical Rotation (Right) | 9.20 | 6.68 | 5.50 | 2.82 | <0.007 |
| Cervical Rotation(Left) | 9.86 | 5.71 | 5.46 | 4.32 | <0.001 |
| Neck disability scale | -13.33 | 3.69 | -8.66 | 4.67 | <0.0001 |
| Visual Analog Scale | -4.79 | 1.129 | -2.48 | 0.8585 | <0.0001 |
Change from baseline in NDI, VAS scale between Groups.
Discussion
This was a comparative study to evaluate the efficacy of ART and MFR on trapezius muscle pain due to spasm, the most commonly found musculoskeletal disorder. ART by the literature is designed to accomplish three unique objectives. These are restoring free and unimpeded motion of soft tissues, release of entrapped nerve, vasculature and lymphatics thereby, re-establishing optimum texture, resilience and function of soft tissue [14,15].
The use of ART, as echoed by many authors, is found to be a successful treatment option in soft tissue injuries and muscle pain like hamstring tightness [14] and flexibility [20], Achilles tendinopathy [21], upper extremity overuse syndrome [22], lateral epicondylitis [23], adductor strain [24] etc. The possible mechanism for this effectiveness may be that ART by virtue of mechanical stimulation causes a reactive hyperemia and produces analgesic effect. Mechanical stimulation through digital pressure invokes the physiological response to cutaneous as well as muscular mechanoreceptors. This may alter the nociception and pain. With manual contact, mechanoreceptors may induce inhibitory effect on central nervous system which may result in decrease in H reflex. Patient also actively does the movement which increase the circulation and thus, reduction in pain and spasm may reduce the symptoms [24].
While in MFR, the gentle forces applied to the facial restrictions will elicit vasomotor response and increase blood flow to the affected area, thereby enhancing lymphatic drainage of toxic metabolic wastes. It also realigns the facial planes, and most importantly resets the soft tissue proprioceptive sensory mechanism. This latter factor reprograms the central nervous system, enabling a normal functional range of motion without eliciting the old pain pattern [25].
Paul J et al., who compared the effect of MFR and deep transverse friction massage for upper trapezius trigger point, explained that MFR improves the vertical alignment and lengthens the body providing more space for proper functioning of osseous structures, nerves, muscles, blood vessels and organs which improves the function [26]. Barnes MF claimed that as a result of MFR, there is change in the viscosity of the ground substance of the muscle and fascia which can restore proper alignment of the muscle fiber and increase the joint mobility. He explained that MFR made the fascia elongated, softened and more pliable thereby, helping to restore the normal length of the fascia. Thus, it can be helpful to increase the flexibility and joint ROM [25,26]. The resultant muscle relaxation may encourage a copious return of blood and oxygen, which dramatically elevates pain threshold and encourage healthy, compliant tissue. This promotes healing, reduces pain and pressure in the fibrous band of connective tissue or fascia by breaking up the adhesions.
This study shows that upper trapezius muscle spasm can cause neck pain, with restriction in cervical range of motion and increase disability according to NDI. Individually both ART and MFR were found to be effective in different conditions. This may be the first study which compares the effectiveness of these two techniques in pain due to trapezius spasm. In the present study ART was found to be more effective than MFR, the reason apart from its effect on the mechanoreceptors, may be because ART works directly on muscle and patient also actively involves himself in movement. As a result the scar tissue adhesions are broken and spasm is relieved due to shortening and lengthening of muscle thereby, giving quick and long lasting effect with regards to pain, mobility and improvement of neck function. Whereas, in MFR the stretch is applied to the fascia, which being the superficial structure has the direct effect. Muscle being the deeper structure will have an indirect effect. So, instant effect in terms of relief in the pain and spasm will be seen immediately following treatment, but it may not last for long period. Multiple sessions may be required to have the cumulative effect and sustained relief.
Limitation
The limitation of the present study was that follow up after four weeks or six weeks was not taken to see the sustained effect of therapy. Side specific involvement as per the dominancy was not considered for analysis.
Conclusion
Although both techniques are effective in alleviation of symptoms and associated disability in upper trapezius muscle spasm, Active Release Technique gave better results as compared to Myofascial Release Technique.
[1]. Kumaresan A, Deepthi G, Anandh V, Prathap S, Effectiveness of positional release therapy in treatment of trapezitisInternational Journal of Pharmaceutical Science and Health care 2012 1(2):71-81. [Google Scholar]
[2]. Punnett L, Wegman DH, Work-related musculoskeletal disorders: the epidemiologic evidence and the debateJournal of electromyography and kinesiology 2004 14(1):13-23.10.1016/j.jelekin.2003.09.01514759746 [Google Scholar] [CrossRef] [PubMed]
[3]. Andersen LL, Andersen CH, Zebis MK, Nielsen PK, Søgaard K, Sjøgaard G, Effect of physical training on function of chronically painful muscles: a randomized controlled trialJournal of Applied Physiology 2008 105(6):1796-801.10.1152/japplphysiol.91057.200818948442 [Google Scholar] [CrossRef] [PubMed]
[4]. Hakala P, Rimpelä A, Salminen JJ, Virtanen SM, Rimpelä M, Back, neck, and shoulder pain in Finnish adolescents: national cross sectional surveysBMJ 2002 325(7367):74310.1136/bmj.325.7367.74312364301 [Google Scholar] [CrossRef] [PubMed]
[5]. Andersen LL, Hansen K, Mortensen OS, Zebis MK, Prevalence and anatomical location of muscle tenderness in adults with nonspecific neck/shoulder painBMC Musculoskeletal Disorders 2011 12(1):16910.1186/1471-2474-12-16921777478 [Google Scholar] [CrossRef] [PubMed]
[6]. Gerdle B, Björk J, Cöster L, Henriksson KG, Henriksson C, Bengtsson A, Prevalence of widespread pain and associations with work status: a population studyBMC Musculoskeletal Disorders 2008 9(1):10210.1186/1471-2474-9-10218627605 [Google Scholar] [CrossRef] [PubMed]
[7]. Ravish VN, Helen S, To compare the effectiveness of myofascial release technique versus positional release technique with laser in patients with unilateral trapezitisJournal of Evolution of Medical and Dental Sciences 2014 3(9):2161-67.10.14260/jemds/2014/2121 [Google Scholar] [CrossRef]
[8]. Chaudhary ES, Shah N, Vyas N, Khuman R, Chavda D, Nambi G, Comparative study of myofascial release and cold pack in upper trapezius spasmInternational Journal of Health Sciences and Research (IJHSR) 2013 3(12):20-27. [Google Scholar]
[9]. Søgaard K, Blangsted AK, Nielsen PK, Hansen L, Andersen LL, Vedsted P, Changed activation, oxygenation, and pain response of chronically painful muscles to repetitive work after training interventions: a randomized controlled trialEuropean Journal of Applied Physiology 2012 112(1):173-81.10.1007/s00421-011-1964-621512799 [Google Scholar] [CrossRef] [PubMed]
[10]. Hanvold TN, Wærsted M, Mengshoel AM, Bjertness E, Stigum H, Twisk J, The effect of work-related sustained trapezius muscle activity on the development of neck and shoulder pain among young adultsScandinavian Journal of Work, Environment & Health 2013 39(4):390-400.10.5271/sjweh.335723494255 [Google Scholar] [CrossRef] [PubMed]
[11]. Hermans V, Spaepen A, Perceived discomfort and electromyographic activity of the upper trapezius while working at a VDT stationInternational Journal of Occupational Safety and Ergonomics 1995 1(3):208-14.10.1080/10803548.1995.1107631910603553 [Google Scholar] [CrossRef] [PubMed]
[12]. de las Peñas CF, Campo MS, Carnero JF, Page JC, Manual therapies in myofascial trigger point treatment: A systematic reviewJournal of Bodywork and Movement Therapies 2005 9(1):27-34.10.1016/j.jbmt.2003.11.001 [Google Scholar] [CrossRef]
[13]. Manheim CJ, The myofascial release manualSlack Incorporated 2008 [Google Scholar]
[14]. Kage V, Ratnam R, Immediate effect of active release technique versus mulligan bent leg raise in subjects with hamstring tightness: a randomized clinical trialInt J Physiother Res 2014 2(1):301-04. [Google Scholar]
[15]. Hammer WI, Functional soft-tissue examination and treatment by manual methods 2007 Jones & Bartlett Learning [Google Scholar]
[16]. Altindag O, Ozaslan S, Efficacy of myofascial release method on pain and disease severity in patients with fibromyalgiaJ Pain Relief 2014 3:16110.4172/2167-0846.1000161 [Google Scholar] [CrossRef]
[17]. Sadria G, Hosseini M, Rezasoltani A, Bagheban AA, Davari A, Seifolahi A, A comparison of the effect of the active release and muscle energy techniques on the latent trigger points of the upper trapeziusJournal of Bodywork and Movement Therapies 2017 21(4):920-25.10.1016/j.jbmt.2016.10.00529037649 [Google Scholar] [CrossRef] [PubMed]
[18]. Shin YJ, Kim WH, Kim SG, Correlations among visual analogue scale, neck disability index, shoulder joint range of motion, and muscle strength in young women with forward head postureJournal of Exercise Rehabilitation 2017 13(4):41310.12965/jer.1734956.47829114506 [Google Scholar] [CrossRef] [PubMed]
[19]. Travell JG, Simons DG, Myofascial pain and dysfunction: the trigger point manual 1983 Lippincott Williams & Wilkins; [Google Scholar]
[20]. George JW, Tunstall AC, Tepe RE, Skaggs CD, The effects of active release technique on hamstring flexibility: a pilot studyJournal of Manipulative and Physiological Therapeutics 2006 29(3):224-27.10.1016/j.jmpt.2006.01.00816584948 [Google Scholar] [CrossRef] [PubMed]
[21]. Miners AL, Bougie TL, Chronic Achilles tendinopathy: a case study of treatment incorporating active and passive tissue warm-up, Graston Technique®, ART®, eccentric exercise, and cryotherapyThe Journal of the Canadian Chiropractic Association 2011 55(4):269 [Google Scholar]
[22]. Schiottz-Christensen B, Mooney V, Azad S, Selstad D, Gulick J, Bracker M, The role of active release manual therapy for upper extremity overuse syndromes—a preliminary reportJournal of Occupational Rehabilitation 1999 9(3):201-11.10.1023/A:1021305902201 [Google Scholar] [CrossRef]
[23]. Howitt SD, Lateral epicondylosis: a case study of conservative care utilizing ART® and rehabilitationThe Journal of the Canadian Chiropractic Association 2006 50(3):182 [Google Scholar]
[24]. Robb A, Pajaczkowski J, Immediate effect on pain thresholds using active release technique on adductor strains: pilot studyJournal of Bodywork and Movement Therapies 2011 15(1):57-62.10.1016/j.jbmt.2010.04.00421147419 [Google Scholar] [CrossRef] [PubMed]
[25]. Barnes MF, The basic science of myofascial release: morphologic change in connective tissueJournal of Bodywork and Movement Therapies 1997 1(4):231-38.10.1016/S1360-8592(97)80051-4 [Google Scholar] [CrossRef]
[26]. Paul J, Kumar M, A comparative study on the effect of Myofascial Release versus Deep Transverse Friction on myofascial trigger points of upper backInternational Journal of Medical [Google Scholar]