Purple coloured urine occurs in the patients, mainly elderly who are on urinary catheters for a long-time and develop Purple Urine Bag Syndrome (PUBS), wherein the urinary bag and the tubing turn in to purple colour. The chain reaction responsible for PUBS begins with tryptophan from the food chain being metabolised by gut bacteria like Enterobacter, Klebsiella, Citrobacter etc., which form sulfatases and phosphatases leading to accumulation of indigo (blue) and indirubin (red) that becomes purple.
Data were from both OPD and indoor patients visiting the hospital between June 2015 to July 2017. Herein, we present a series of nine cases from our tertiary care hospital that had developed PUBS which can occur in any patient with Urinary Tract Infection (UTI) on catheter with bacteria possessing these enzymes. Bed-bound patients or population with Alzheimer’s, or dementia are groups of the patients who are at higher risk for UTI. Although, PUBS is a harmless problem, prevention and control of the catheter-associated UTIs is very important in present medical era.
Catheter, Diabetic, Nephropathy
One of the rare pathologic entities, initially reported in 1978, is PUBS. It is characterised clinically by purple discolouration of the urine, and is mostly seen in chronically debilitated female subjects. Subjects affected by this pathology and unaware of the lesion get particularly distressed. Association of UTI is often found to be present with PUBS [1]. In the current study, we have summarised a case series of nine subjects affected with PUBS.
Details of Cases
In our tertiary care hospital, series of nine cases affected with PUBS was reported. All these patients reported from June 2015 to July 2017.
Case 1: An 88-year-old male diagnosed with PUBS. The patient was bed ridden for six months, had Type 2 Diabetes Mellitus (DM), Diabetic Nephropathy (DN), and End-Stage Renal Disease (ESRD). He was treated with haemodialysis for three months.
Case 2: An 82-year-old male patient was diagnosed with PUBS. The patient had type 2 DM, DN, Alzheimer’s disease. He was on catheter for enlarged prostate and PUBS was noted on and off for two years duration.
Case 3: A 72-year-old male patient diagnosed with diabetes, coronary artery disease and post Coronary Artery Bypass Grafting (CABG) had developed urethral stricture. He developed UTI with pyelonephritis and later developed renal abscess. Patient was catheterised for three weeks and developed PUBS during hospital stay. Urine culture showed Enterococcus and E. coli growth.
Case 4: A 73-year-old female patient had acute viral hepatitis with hepatitis A reactive disease with fulminant hepatic failure. She developed intestinal perforation and peritonitis and sepsis. Patient was catheterised for six weeks and had purple urine during hospital course. Urine culture growth showed Pseudomonas.
Case 5: A 65-year-old male patient had diabetes mellitus, chronic kidney disease Stage 3 and coronary artery disease with ejection fraction of 35%. He developed Cerebrovascular Accident (CVA) and right hemiparesis and was bed ridden for one year. All the while he was catheterised and had recurrent UTI with polymicrobial growth (E. coli and Klebsiella).
Case 6: An 82-year-old male patient had chronic kidney disease Stage 3 with hypertension. He was post Cardiopulmonary Resuscitation (CPR) survivor with hypoxic brain injury. The patient was bed ridden and on catheter for two years. He had recurrent UTI (Klebsiella and Pseudomonas) during multiple admissions.
Case 7: A 70 year-old male patient with Middle Cerebral Artery (MCA) infarct causing CVA was in bed ridden state for one and half months. He was catheterised for 3-4 weeks and his urine culture grew Gram positive infection (E. coli).
Case 8: A 60-year-old female patient diagnosed with hypertension and COAD-IV with corpulmonale was on domiciliary Non Invasive Ventilation (NIV). She was on steroid treatment for six weeks. She was on catheter since three weeks.
Case 9: A 76-year-old male patient was diagnosed with chronic liver disease with hepatic encephalopathy Grade 2 and chronic pancreatitis. Patient was on catheter for 20 days and developed UTI with urine culture showing Acinetobacter.
Patients were distributed in three age groups: Group 1: 60-70 years, Group 2: 71-80 years and Group 3: 81-90 years. In the present study, there were seven male patients and two female patients.
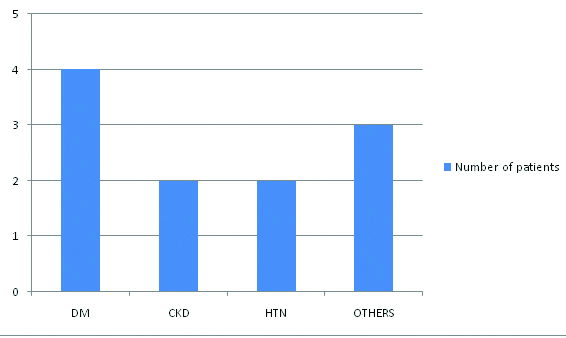
Even though PUBS and bacteriuria persisted, all patients had stable vital signs and had no symptoms of infection, leucocytosis or fever. These patients did not receive any significant antibiotic treatment. Duration of catheterisation was decreased in all the patients and regular replacement of Foley’s and urine bag along with improved quality of catheter care, improved or stopped PUBS. [Table/Fig-1] shows distribution of patients according to presence of comorbid condition.
Distribution of patients according to type of comorbid condition.
Discussion
Purple urine bag syndrome has been reported in patients with prolonged catheterisation. It was found to be associated with alkaline urine, UTIs, renal failure, polyvinyl chloride urine bag, and dementia. Most cases of PUBS turn out to be clinically harmless though underlying UTI can lead to serious complications as typical symptoms of dysuria are absent [2,3]. In urine culture, several bacterial species have been reported in association with PUBS including Providencia stuartii, P. rettgeri, K. pneumoniae, P. mirabilis, E. coli, Morganella morganii, and Pseudomonas aeruginosa [4-6]. A previous study showed that PUBS occurred predominantly in chronically catheterised, constipated women [7]. PUBS was found to be associated with alkaline urine as well as UTI induced by some species of bacteria with indoxylsulphatase/phosphatase [8]. Female gender or constipation was possibly not the absolute criteria of PUBS. Similar view has been taken by Lin HH et al., [9]. In a prevalence study of Hospital-Acquired Infections (HAIs) done by Zotti CM et al., a significant correlation was found with major risk factors related to medical procedures, such as urinary catheterisation [10]. Landi F et al., concluded in their study that a failure to decrease the unnecessary bladder catheter use and the duration of catheterisation would result in poor quality of care [11], according to study done by Zotti CM et al., a greater mean length of stay in hospital, and a higher risk of nosocomial UTI [10].
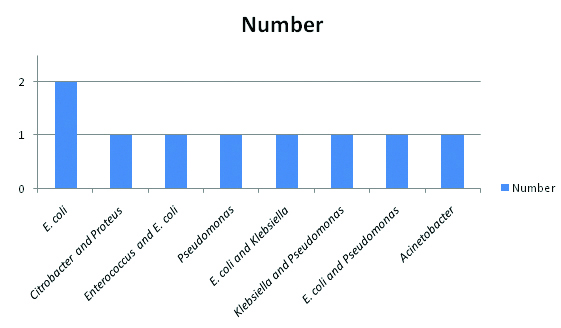
P. mirabilis compromises the care of many patients undergoing long-term indwelling bladder catheterisation [4]. [Table/Fig-2] shows the prevalence of type of microorganisms in the present study.
Prevalence of type of microorganisms in the present case series.
With increasing life expectancy of the Indian population and improved geriatric care, it would be useful if the awareness about this entity is present among practicing clinicians in primary and secondary health care setting. This would serve to avoid expensive investigations, unjustified antibiotic use, and unwarranted anxiety among patients, care takers and treating physicians while promoting early diagnosis and management of PUBS. Also this would lead to reducing anxiety among patients and care-providers and unwarranted cost of repeated health visits [1-3]. Yaqub S et al., reported a case report of a geriatric patient with UTI who presented with PUBS. After the commencement of the antibiotic therapy, the purple urine disappeared [12]. Strong association of constipation and intestinal obstruction has been observed with PUBS. Alteration of the gut motility and bacterial flora of the intestine occurs with chronic constipation. Dietary tryptophan is converted into indole, pyruvic acid, and ammonia by the tryptophase present in the normal bacterial flora. This is followed by rapid absorption of Indole into the portal circulation, after which its conversion into indoxylsulphate occurs in liver. Purple colour is then formed by mixing of indirubin and indigo, formed from indoxyl. Data from the past literature also shows that PUBS can be precipitated with other intestinal conditions like intestinal obstruction [13-16].
Under the light of above mentioned data, it can be suggested that PUBS seems to be a benign pathology with absence of any major consequences, and majority of the subjects are asymptomatic. Therefore, some researchers have an agreement that only altering the urinary catheter and urinary bag normally are sufficient to resolve the issue [15,16].
Conclusion
Purple urine bag syndrome is an uncommon condition that is getting increasingly noted nowadays. It is a harmless presentation and need not be aggressively treated. The presentation is commonly seen in elderly bed ridden patients who have indwelling catheter for long-time. It is not useful to treat these patients aggressively. The purpose of the study is to spread awareness about the entity to avoid alarm being raised by practicing doctors.
[1]. Al Montasir A, Al Mustaque A, Purple urine bag syndromeJournal of Family Medicine and Primary Care 2013 2(1):104-105.10.4103/2249-4863.10997024479059 [Google Scholar] [CrossRef] [PubMed]
[2]. Stanfel LA, Gulyassy PF, Jarrard EA, Determination of indoxylsulfate in plasma of patients with renal failure by use of ion-pairing liquid chromatographyClin Chem 1986 32:938-42. [Google Scholar]
[3]. Peters P, Merlo J, Beech N, Giles C, Boon B, Parker B, The purple urine bag syndrome: A visually striking side effect of a highly alkaline urinary tract infectionCan Urol Assoc J 2011 5:233-34.10.5489/cuaj.1017721801678 [Google Scholar] [CrossRef] [PubMed]
[4]. Tumbarello M, Citton R, Spanu T, Sanguinetti M, Romano L, Fadda G, ESBL-producing multidrug-resistant Providencia stuartii infections in a university hospitalJ Antimicrob Chemother 2004 53(2):277-82.10.1093/jac/dkh04714688041 [Google Scholar] [CrossRef] [PubMed]
[5]. Choi HK, Kim YK, Kim HY, Park JE, Uh Y, Clinical and microbiological features of Providencia bacteremia: experience at a tertiary care hospitalKorean J Intern Med 2015 30:219-25.10.3904/kjim.2015.30.2.21925750564 [Google Scholar] [CrossRef] [PubMed]
[6]. Barrios H, Garza-Ramos U, Reyna-Flores F, Sanchez-Perez A, Rojas-Moreno T, Garza-Gonzalez E, Isolation of carbapenem-resistant NDM-1-positive Providencia rettgeri in MexicoJ Antimicrob Chemother 2013 68:1934-36.10.1093/jac/dkt12423620464 [Google Scholar] [CrossRef] [PubMed]
[7]. Su FH, Chung SY, Chen MH, Sheng ML, Chen CH, Chen YJ, Case analysis of purple urine-bag syndrome at a long-term care service in a community hospitalChang Gung Med J 2005 28:636-42. [Google Scholar]
[8]. Ribeiro JP, Marcelino P, Marum S, Fernandes AP, Grilo A, Case report: Purple urine bag syndromeCrit Care 2004 8(3):R13710.1186/cc285315153241 [Google Scholar] [CrossRef] [PubMed]
[9]. Lin HH, Li SJ, Su KB, Wu LS, Purple urine bag syndrome: a case report and review of the literatureJ Intern Med Taiwan 2002 13:209-12. [Google Scholar]
[10]. Zotti CM, Ioli MG, Charrier L, Arditi G, Argentero PA, Biglino A, Hospital-acquired infections in Italy: a region wide prevalence studyJ Hosp Infect 2004 56(2):142-49.10.1016/j.jhin.2003.10.00115019227 [Google Scholar] [CrossRef] [PubMed]
[11]. Landi F, Cesari M, Onder G, Zamboni V, Barillaro C, Lattanzio F, Indwelling urethral catheter and mortality in frail elderly women living in communityNeurourol Urodyn 2004 23(7):697-701.10.1002/nau.2005915382190 [Google Scholar] [CrossRef] [PubMed]
[12]. Yaqub S, Mohkum S, Mukhtar KN, Purple urine bag syndrome: A case report and review of literatureIndian J Nephrol 2013 23(2):140-42.10.4103/0971-4065.10944223716923 [Google Scholar] [CrossRef] [PubMed]
[13]. Chung SD, Liao CH, Sun HD, Purple urine bag syndrome with acidic urineInt J Infect Dis 2008 12:526-27.10.1016/j.ijid.2008.02.01218514009 [Google Scholar] [CrossRef] [PubMed]
[14]. Muneoka K, Igawa M, Kurihara N, Kida J, Mikami T, Ishihara I, Biochemical and bacteriological investigation of six cases of Purple Urine Bag Syndrome (PUBS) in a geriatric ward for dementiaNihon Ronen Igakkai Zasshi 2008 45:511-19.10.3143/geriatrics.45.51119057104 [Google Scholar] [CrossRef] [PubMed]
[15]. Tang MW, Purple urine bag syndrome in geriatric patientsJ Am Geriatr Soc 2006 54:560-61.10.1111/j.1532-5415.2006.00643_13.x16551343 [Google Scholar] [CrossRef] [PubMed]
[16]. Bar-Or D, Rael LT, Bar-Or R, Craun ML, Statz J, Garrett RE, Mass spectrometry analysis of urine and catheter of a patient with purple urinary bag syndromeClin Chim Acta 2007 378:216-18.10.1016/j.cca.2006.11.01517196573 [Google Scholar] [CrossRef] [PubMed]