In peripheral nerve blocks, most anaesthetists prefer adding an adjuvant to local anaesthetic drugs to enhance the block by reducing the time of onset of block, improving the quality of block and prolonging the duration of blocks. Supraclavicular brachial plexus block provides anaesthesia to the entire upper limb. Many adjuvants like epinephrine, dexamethasone, opioids, alpha agonists, midazolam, ketamine, etc., have been used successfully over many years. They provide varied block characteristics and show different side effect profiles. Clonidine is a selective alpha adrenergic receptor agonist and it has been used as an adjunct to LA in various doses [1]. It definitely reduces the onset tie and prolongs duration of anaesthesia. However, higher doses have demonstrated various side effects like hypotension, bradycardia, sedation, etc., [1]. Clonidine opens up potassium channels leading to membrane hyperpolarisation; this amplifies the sodium channel blockade of local anaesthetic agents. In this state the cell is not responsive to excitatory inputs [2]. In clinical studies, on adding clonidine to local anaesthetic solutions, peripheral nerve blocks reduced the onset time, improved the efficacy of the block during surgery and extended the postoperative analgesia [3,5]. Clonidine has shown greater analgesic potential when added to local anaesthetics in peripheral nerve blocks.
The present study aimed to compare clonidine in two different doses with local anaesthetics in combination (lignocaine and bupivacaine) for supraclavicular approach to brachial plexus block.
Materials and Methods
The present study was carried out after the approval of Research Ethics Committee and written informed consent of the patients. The study was conducted from 1st July 2015 to 30th June 2016 in 90 ASA I and ASA II patients. They were aged between 18 and 60 years of either sex, weight range 40 to 70 kg, and were posted for unilateral upper limb surgery at a tertiary care hospital. The power of the study was calculated to be 0.831.
Patients with consent refusal, ASA Grade III and IV, with history of peripheral neuropathy, pregnant women, coagulation disorders, history of drug allergy or sensitivity to drugs, cutaneous infection at injection site and psychiatric disease were excluded from the study. All patients underwent a routine pre-anaesthetic check-up; where thorough history and general physical examination and routine investigations of the patient were carried out. Study protocol was explained and informed consent was taken. Premedication with tablet alprazolam 0.5 mg at 10 pm and at 5 am in the morning on the day of surgery (with a sip of water) was advised. The patients were randomly allocated to three groups of 30 patients each. Supraclavicular brachial plexus block was then performed by the anaesthesiologist using an ultrasound-guided technique with a total volume of 30.6 mL of drugs. Group N received 15 mL 2% lignocaine with adrenaline (1 in 200000) and 15 mL 0.5% bupivacaine with 0.6 mL of normal saline making a total volume of 30.6 mL. Group C1 received 15 mL 2% lignocaine with adrenaline (1 in 200000) and 15 mL 0.5% bupivacaine with 45 μg (0.3 mL) of clonidine plus 0.3 mL of normal saline. Group C2 received 15 mL 2% lignocaine with adrenaline (1 in 200000) and 15 mL 0.5% bupivacaine with 90 μg (0.6 mL) of clonidine.
After obtaining baseline vital data (ECG, heart rate, blood pressure and pulse oximetry) the patient was kept in a supine position, the skin was disinfected and the ultrasound transducer was positioned in the transverse plane immediately superior to the clavicle. The transducer was tilted caudally to obtain a cross-sectional view of the subclavian artery. The brachial plexus was seen as a collection of hypo-echoic oval structures lateral and superficial to the artery. The needle was inserted in plane into the peri-neural sheath. After a careful aspiration, 1 to 2 mL of local anaesthetic was injected document the proper needle placement. When the injection displaced the brachial plexus away from the needle, an additional advancement of the needle 1 to 2 mm deeper was required sometimes to accomplish adequate spread of the local anaesthetic. Then, the drug mixture was injected according to the groups allocated.
Time to the onset of sensory blockade in each of the major peripheral nerve distribution (ulnar, radial, median, musculocutaneous) and motor blockade was noted according to a three point score by pinprick method, by using blunt tip of 27 G needle at 0, 2, 5, 10, 15, 20, and 30 minutes. The duration of sensory and motor block was assessed postoperatively every hourly.
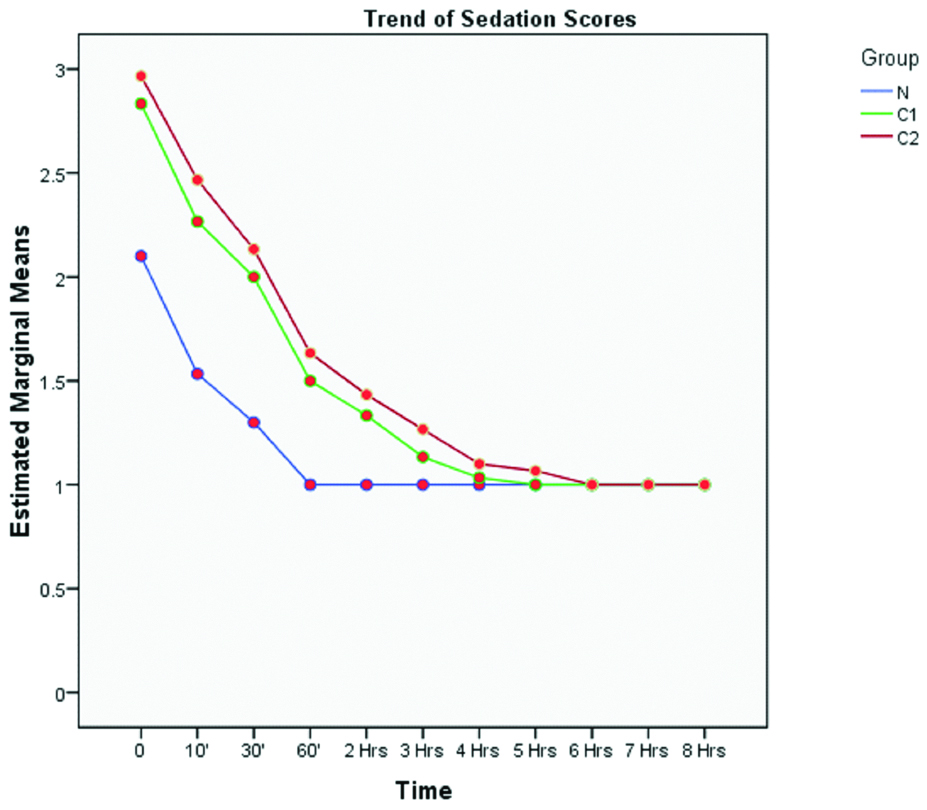
The quality of analgesia was assessed during surgery and was considered satisfactory if the patient did not complain of any pain or discomfort and if no sedation was required. In the postoperative period, analgesia was assessed according to a VAS score. When patient began to experience pain more than 8 on the VAS it was considered that the analgesic action of the drug had terminated and rescue analgesic was given (iv/im diclofenac sodium 1-1.5 mg/kg). In the circumstance of an insufficient block or the patient did not tolerate the procedure the block was supplemented with general anaesthesia and the case was excluded from the study. Heart rate, blood pressure, SpO2 was noted before anaesthesia (baseline), at premedication, in operation theatre, at two minutes and then at five minutes interval for the first 30 minutes and 15 minutes interval for the next two hours or till the surgery ends. Sedation score was assessed by using the Ramsay sedation scale for eight hours postoperatively.
Statistical Analysis
All the observations were noted and charted. Statistical analysis was done using ANOVA and Pearson’s chi-square test.
Results
Both groups were comparable in terms of age, gender and weight [Table/Fig-1a,b]. The baseline haemodynamic parameters were comparable in both groups.
| Group | Age (in years) | Weight (in kg) |
|---|
| Mean | SD | p-value | Mean | SD | p-value |
|---|
| N | 31.7 | 12.8 | 0.5766(Group N vs. C1) | 58.92 | 9.54 | 0.35(Group N vs. C1) |
| C1 | 33.6 | 13.4 | 0.1889(Group C1 vs. C2) | 60.57 | 8.74 | 0.43(Group C1 vs. C2) |
| C2 | 38.5 | 15.1 | 0.0649(Group N vs. C2) | 59.68 | 7.62 | 0.09(Group N vs. C2) |
| Sex | N | C1 | C2 |
|---|
| No. | % | No. | % | No. | % |
|---|
| Male | 22 | 73 | 22 | 73 | 24 | 80 |
| Female | 8 | 27 | 8 | 27 | 6 | 20 |
Motor Assessment
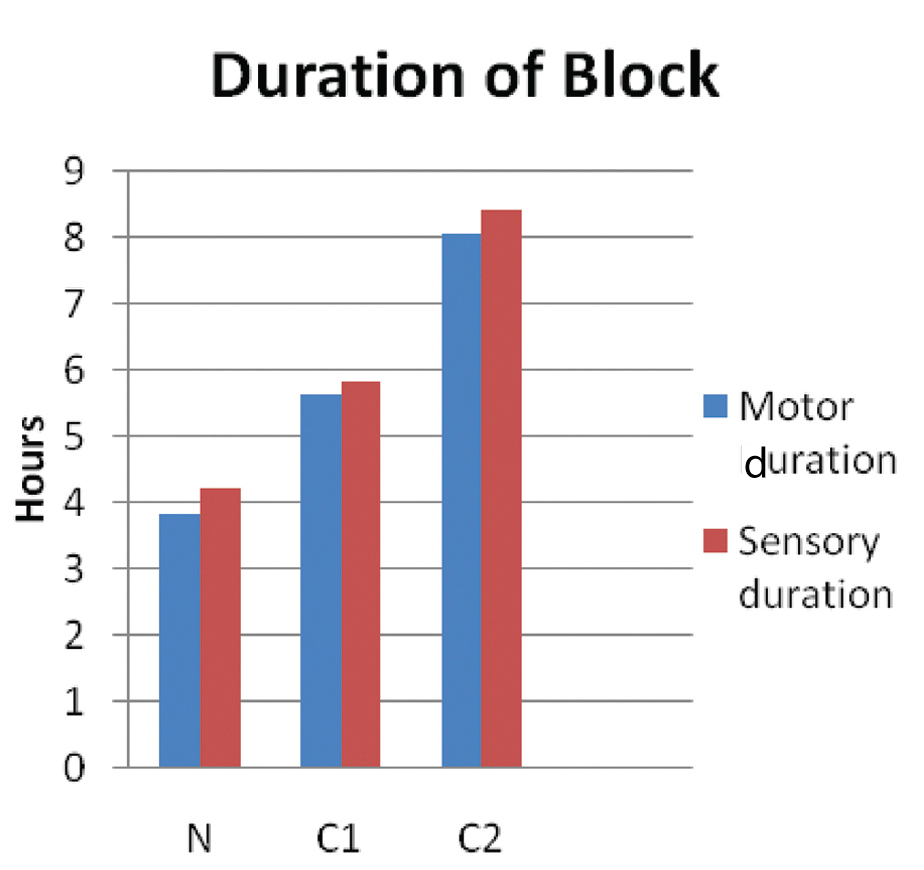
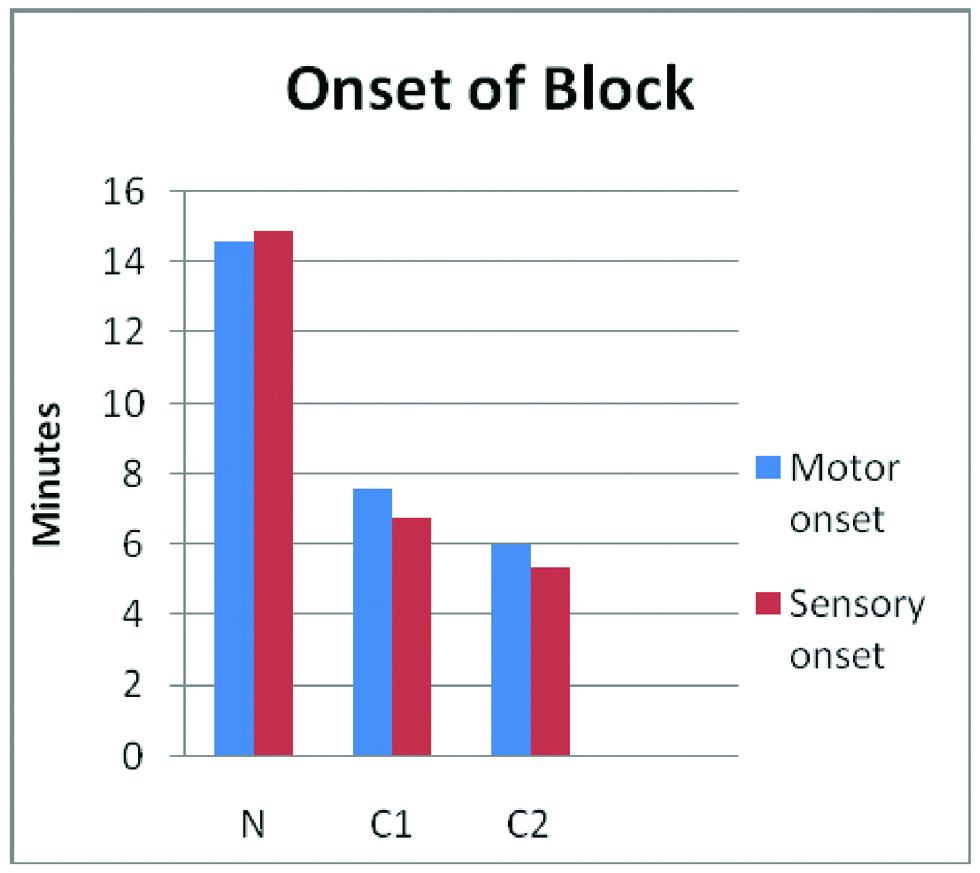
Time from injection to inability of patient to move his/her fingers or raise the hand was assessed in minutes. The mean duration (in minutes) of onset of motor block was 14.6±3.024 in Group N, 7.567±1.0726 in Group C1, 6.033±1.756 in Group C2. The onset was faster in Groups C2 and C1 than Group N and was statistically highly significant (p<0.001) [Table/Fig-2]. The mean duration (in hours) of motor block was 3.8±0.6967 in Group N, 5.65±1.1533 in Group C1, 8.05±0.9035 in Group C2. The mean duration of motor block was higher in Groups C2 and C1 than N and was statistically highly significant (p<0.001) [Table/Fig-2,3].
| Group of patients | Motor onset | Motor duration |
|---|
| Mean | SD | p-value | Mean | SD | p-value |
|---|
| N | 14.6 | 3.0240 | <0.001 | 3.850 | 0.6967 | <0.001 |
| C1 | 7.567 | 1.0726 | 5.650 | 1.1533 |
| C2 | 6.033 | 1.7564 | 8.050 | 0.9035 |
Sensory Assessment
Time to the onset of sensory blockade in each of the major peripheral nerve distribution (ulnar, radial, median, musculocutaneous) was noted according to a three point score by pinprick method. The mean onset of time (in minutes) of sensory block is 14.9±3.1442 in Group N, 6.8±1.0635 in Group C1 and 5.4±2.4403 in Group C2 [Table/Fig-4,5]. The difference was highly statistically significant (p<0.001).
| Group of patients | Sensory onset | Sensory duration |
|---|
| Mean | SD | p-value | Mean | SD | p-value |
|---|
| N | 14.900 | 3.1442 | <0.001 | 4.233 | 0.6915 | <0.001 |
| C1 | 6.800 | 1.0635 | 5.833 | 1.0367 |
| C2 | 5.400 | 2.4403 | 8.417 | 0.8914 |
The mean duration (in hours) of sensory block was 4.233±0.6915 in Group N, 5.833±1.0367 in Group C1 and 8.417±0.8914 in Group C2. The difference was highly statistically significant (p<0.001).
Postoperative Monitoring
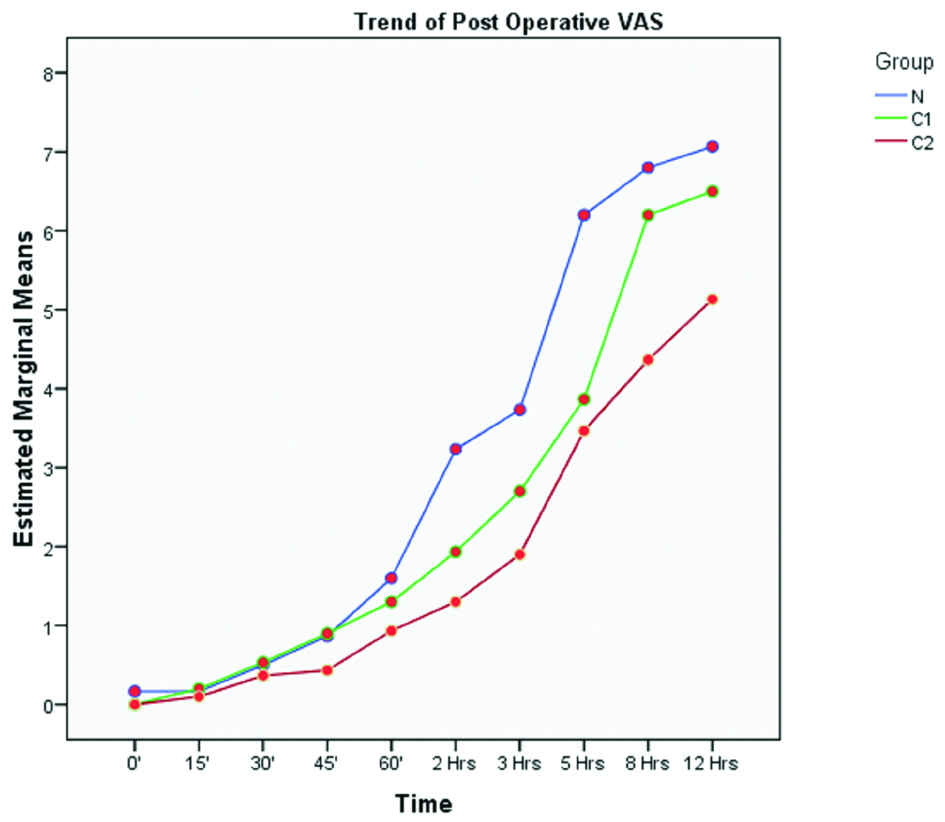
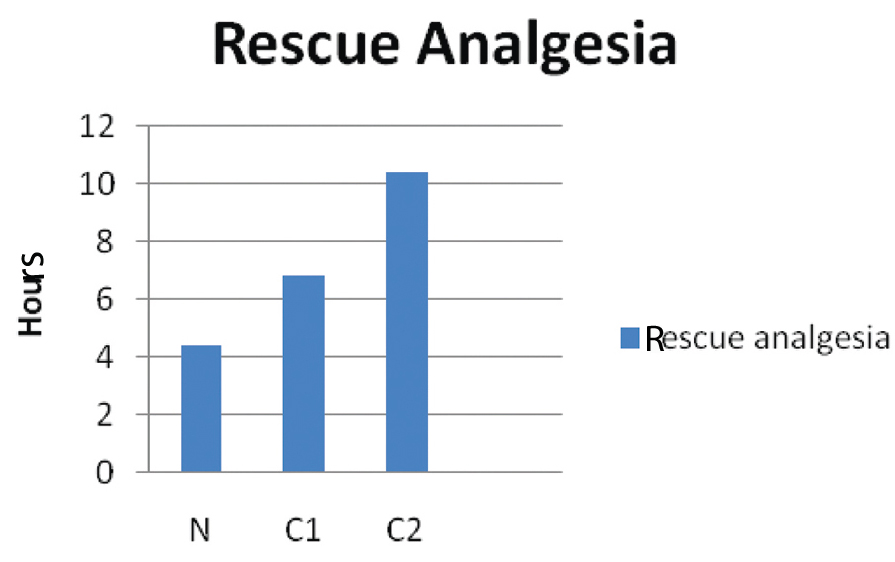
In the postoperative period analgesia was assessed according to a VAS score [Table/Fig-6]. Sedation score was assessed by using the Ramsay sedation scale for eight hours postoperatively [Table/Fig-7]. Rescue analgesia (iv/im diclofenac sodium 1-1.5 mg/kg) was required much earlier in Group N (4.43±0.774 hours) than in groups C1 (6.87±0.9 hours) and C2 (10.43±2.339 hours) [Table/Fig-8,9]. This was statistically highly significant.
Postoperative VAS scores.
Rescue analgesia requirements.
| N | Mean | Std. Deviation | p-value |
|---|
| Rescue analgesia | N | 30 | 4.43 | 0.774 | <0.001 |
| C1 | 30 | 6.87 | 0.900 |
| C2 | 30 | 10.43 | 2.239 |
Time for rescue analgesia.
Adverse Events
Incidence of drowsiness, pruritus, nausea, vomiting, Horner’s syndrome, unilateral phrenic nerve palsy, pneumothorax, respiratory depression and signs for local anaesthesia toxicity were looked for and noted. None of the patients had any such incidents.
Discussion
In the present study, brachial plexus blockade was achieved by Ultrasound Guided (USG) supraclavicular approach and satisfactory surgical anaesthesia was attained in all the cases for upper limb surgeries. Clonidine, when added to Local Anaesthetics (LA), was found to be superior to LA alone. Bernard JM and Macarie P, Patil KN and Singh ND, Kohli S et al., and Chakraborty S et al., concluded that clonidine as an adjuvant to ropivacaine significantly enhances the quality of supraclavicular brachial plexus block by faster onset, prolonged duration of sensory and motor block and improved postoperative analgesia, without associated adverse effects [1,3-5].
However, many studies contradict these. Jaiswal R et al., evaluated the effect of adding clonidine to ropivacaine for axillary plexus blockade, the addition of clonidine (150 micrograms) was of no benefit in the onset and duration of block [6].
Onset of Blocks
In the present study, the onset of both sensory and motor block was faster in Group C2 and C1 than Group N and was statistically highly significant (p<0.001). Also, the onset both motor and sensory was earlier in Group C2 than C1, which was highly statistically significant.
Chakraborty S et al., studied 70 patients, in which onset was almost seven minutes faster in the group with clonidine and bupivacaine (10.6±1.36 minutes) than in the group with only bupivacaine and saline (18.1±1.35 minutes) [5]. In a study by Kohli S et al., the motor and sensory onset were faster in the group with clonidine 2 μg/kg than in the group with 1 μg/kg clonidine [4]. In studies by Routray SS et al., and Prajapati J and Parmar H, the onset of the block were earlier in the group with 150 mcg clonidine than those in the group without clonidine [7,8]. In a similar study by Patel C et al., the mean time of onset for sensory and motor block was 8.3±1.45 minutes and 13.1±1.46 minutes for control group and 8.0±0.93 and 14.3±1.31 minutes for Group with clonidine [9].
However, in a study by Mohammed A et al., there was no statistically significant difference in the onset of sensory and motor [10]. This differs from the present study.
Duration of Blocks
The mean duration of sensory block was 4.233±0.6915 in Group N, 5.833±1.0367 in Group C1 and 8.417±0.8914 in Group C2 in the present study (p<0.001). Also, the duration of both motor and the sensory blockade was longer in Group C2 than C1.
Routray SS et al., Singelyn FJ et al., El Saied AH et al., and Ali QE et al., concluded in their study that adding clonidine to brachial plexus prolongs duration of anaesthesia and analgesia in brachial plexus block [7,11,12,13]. In the previous studies by Prajapati J and Parmar H, Mohammed A et al., by Gupta S et al., by Sirohiya P et al., and by Rustagi P et al., the duration of sensory and motor blocks were higher in the groups with clonidine added to ropivacaine than the group with only ropivacaine [8,10,14-16].
In the study by Chakraborty S et al., clonidine provided analgesia much longer than the control group [5]. The mean time for rescue analgesia was 415.4±38.19 minutes in the clonidine group but 194.2±28.74 minutes in the other group. In the study by Kohli S et al., postoperative analgesia lasted for 21.0±2.96 hours in Group II with 2 μg/kg clonidine and 14.9±3.0 hours in Group I with 1 μg/kg clonidine [4]. Postoperatively all patients in Group I required rescue analgesia by 20 hours, whereas in Group II the same was true only after 24 hours. In a study by Singh S and Aggarwal A, the majority of the patients (56%) of the clonidine group, recovery of sensation occurred after eight hours whereas in the control group, all patients had recovered sensations by eight hours [17]. The present study was comparable with the study by Mohammed A et al., regarding analgesia duration [10].
Haemodynamic Factors
All the patients of all three groups in the present study were haemodynamically stable at all times intraoperatively and postoperatively in relation to Heart Rate (HR), Systolic Blood Pressure (SBP), Diastolic Blood Pressure (DBP), Mean Arterial Pressure (MAP) and SpO2. None of them had hypotension, bradycardia or respiratory depression.
In a study by Kohli S et al., the haemodynamic parameters (mean HR, MAP, SpO2) remained stable at all times in most of the patients both intraoperatively and postoperatively in their study [4]. One episode of bradycardia and no episode hypotension with 1 μg/kg while two episodes of bradycardia and one episode of hypotension with 2 μg/kg was seen. Hence, with higher dose of clonidine showed occurrence of hypotension and bradycardia in the present study. However, in the present study no such episode of hypotension or bradycardia was seen even with 90 μg clonidine. Stable haemodynamics was also reported by Singelyn FJ et al., El Saied et al., and Sebastian D et al., [11,12,18]. In the study by Rustagi P et al., significantly lower pulse rate was found at 40 minutes up to 8th hour (p<0.05) in group receiving clonidine while in group where only saline was used [16]. Also, significantly lower blood pressure was recorded at 50 minutes up to 8th hour (p<0.05) in Group A while in Group B no statistically significant difference was found (p>0.05).
However, contrasting results were obtained in the study by Bernard JM et al., wherein a 30% fall in SBP was seen with 300 μg, 20% fall with 90 μg and 15% fall with 30 μg clonidine [1]. In the same study, with the highest dose of clonidine (300 μg) 4 patients out of 14 patients had one episode of hypoxaemia (SpO2 <90% lasting 20 sec or more). In our study we used only upto 90 μg of clonidine and no episode of hypoxaemia was noticed in any of the cases.
In the study by Gupta S et al., mean arterial pressure did not show significant change between the two groups in preoperative, intraoperative and postoperative period [14]. Both groups did not show significant changes in mean pulse rate during preoperative, intraoperative and postoperative period. In two studies [7,15] there were no statistically significant differences in the haemodynamic parameters (pulse rate, MAP, SpO2) between the clonidine groups and the placebo groups throughout the surgery and postoperatively. These two studies are comparable to the present study, which too did not show any significant differences in these parameters within the three groups.
Limitation
Different surgeries require different levels of pain relief. Hence one of the major limitations of present study is a well-defined cohort type of surgery which were done under supraclavicular block which may have slightly skewed the VAS scores.
Conclusion
In conclusion, 90 μg clonidine is an attractive alternative as an adjuvant with bupivacaine and lignocaine in the ultrasound guided supraclavicular block for upper limb surgical procedures especially in those that need quite long time with minimal side effects and excellent quality of postoperative analgesia. Clonidine fastens the onset time to sensory and motor block as compared to lignocaine and bupivacaine combined in a dose-dependent manner. Clonidine also provides better quality analgesia than LA drugs alone.