Dental implant treatment is a commonly used modality for replacement of the lost or missing teeth. However, this modality is not without complications. Thus, accurate assessment of the dimensions and morphology of bone must be carried out by clinical examination of the ridge at the site of implant placement. Selection of implant size depends on the width and height of bone and location of the inferior alveolar canal [1-3]. Complications may occur during surgery, in the recovery phase or even after loading. In most cases, it is necessary to ensure accurate positioning of drill and implant fixture by clinical and radiographic examination of the areas where bone needs to be removed [4]. Several techniques are used for evaluation of implant placement site such as palpation of the alveolar ridge, use of osteometer (A measuring device, is an appropriate physical method of measuring submylohyoid [1]. DTX200 steometer (A/S, Copenhagen, Denmark) is a commonly used osteometer) and diagnostic casts for assessment of intermaxillary relations and use of advanced imaging modalities [1].
Lingual concavity or undercut is a common finding in the posterior mandible, and ignoring this undercut may result in perforation of the lingual cortex [5], traumatisation of vital anatomical structures, neurologic injuries and severe bleeding in the floor of the mouth, which can be fatal if it causes upper airway obstruction [6]. Thus, in order to prevent these complications, accurate radiographs are required to quantify the amount of bone, assess the location of adjacent anatomical structures and select the proper size of fixture and proper implant placement site. Radiography can be a valuable surgical guide for this purpose [7]. Periapical and panoramic radiographs are often used to assess the site of implant placement. However, these techniques are two-dimensional and cannot provide adequate information about the bone width [8]. Cross-sectional analysis using CBCT is suitable for assessment of lingual undercuts and prevention of lingual cortex perforation and subsequent complications. It has been proven that CBCT is beneficial when visualisation of a second plane is required prior to implant placement [9,10]. CBCT scans of the mandible visualise the degree of concavity in the first molar site and can greatly help in selection of proper size, location and buccolingual angulation of implant fixture [2,11]. Thus, CBCT assessment of lingual concavity must be considered as part of dental implant treatment planning to prevent lingual plate perforation, hemorrhage, nerve damage and infection [12].
Lingual concavity is a potential risk in implant surgery, and studies on lingual concavity in the posterior mandible are limited. Thus, this study was designed to evaluate the prevalence and morphology of the concavity in the mandibular first molar site on cross-sectional CBCT images.
Materials and Methods
In this cross-sectional study, we evaluated CBCT scans of 164 patients retrieved from the archives of the Oral and Maxillofacial Radiology Department of Hamadan University of Medical Sciences. The CBCT scans taken during a one-year period (from January 2016 to January 2017) were selected using consecutive sampling. All CBCT scans were obtained by NewTom 3G (NewTom, Verona, Italy) with 1000×1000 pixel detector and 110 kVp, 1.2 mA and 5.4s. The inclusion criterion was absence of mandibular first molar. The CBCT scans with low resolution or artifacts and patients with pathologic lesions, alveolar bone grafts or dental implants in the posterior mandible were excluded. Two oral and maxillofacial radiologists assessed the CBCT scans in terms of lingual undercuts. Since NNT Viewer software (NewTom, Verona, Italy) was used for measurement of variables, the validity of measurements was acceptable.
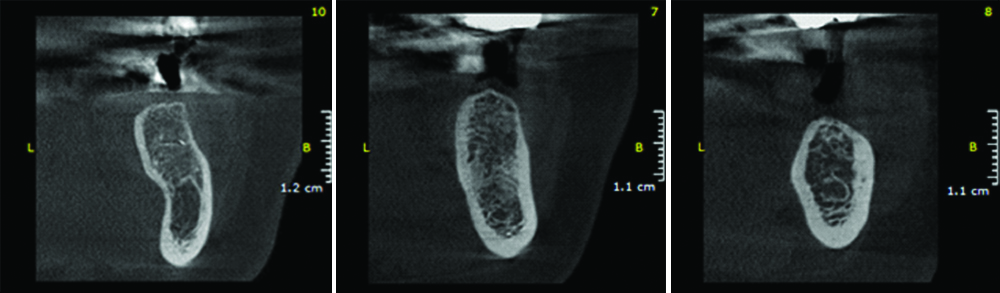
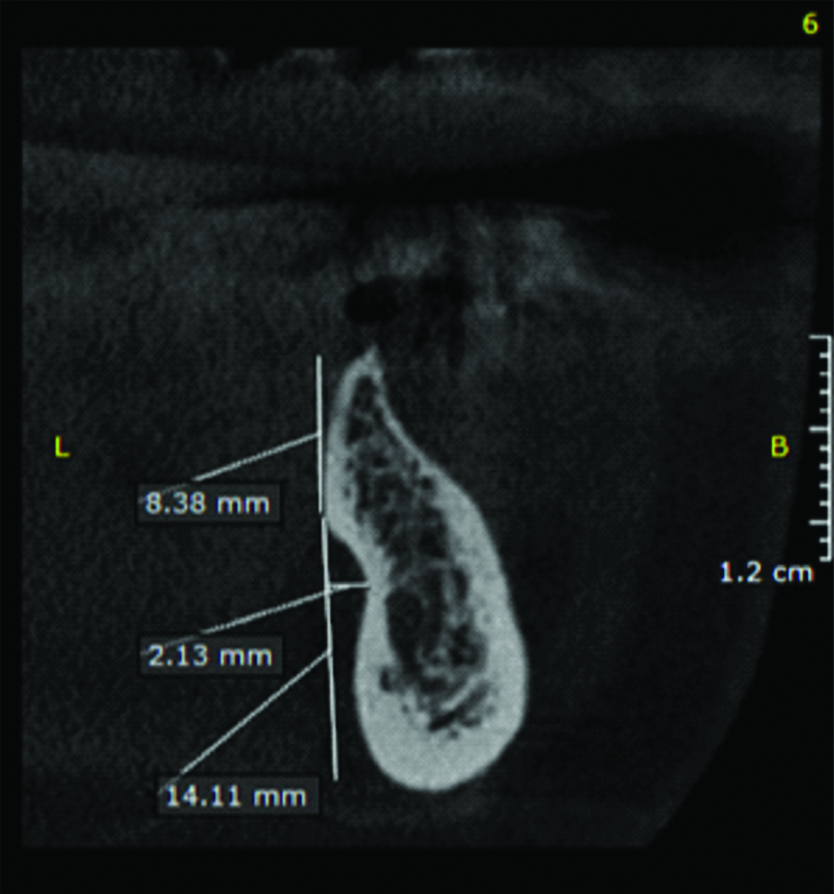
The lingual undercut was assessed on cross-sectional CBCT images. If the second molar tooth was present, the cross-sectional slice was selected at the mid-point of the mesiodistal distance between the second premolar and second molar teeth. If the second molar tooth was missing, the cross-sectional slice was selected 5 mm distal to the second premolar tooth [4]. Three types of ridge morphology were defined. Type U was defined as ridge base narrower than the alveolar crest and presence of lingual undercut. Type C or convex type was defined as ridge base wider than the alveolar crest. Type P or parallel type was defined as the parallel form of the ridge [Table/Fig-1] [4]. [Table/Fig-2] shows the location of cross-sectional slice on the panoramic image in presence and absence of second molar. On cross-sectional CBCT images, one line was drawn 2 mm above the inferior alveolar canal and another line was drawn 2 mm below the alveolar crest. The length of these lines and the vertical distance between the ridge crest and the line drawn 2 mm above the crest were measured by the ruler of NNT software [Table/Fig-3].
Types of ridge morphology on cross-sectional CBCT images (from right to left: type U, type P, type C).
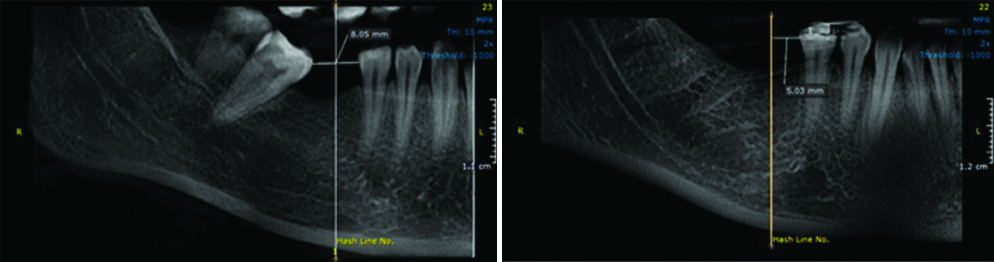
Location of cross-sectional slice on the panoramic image; Left: in presence of second molar; right: in absence of second molar.
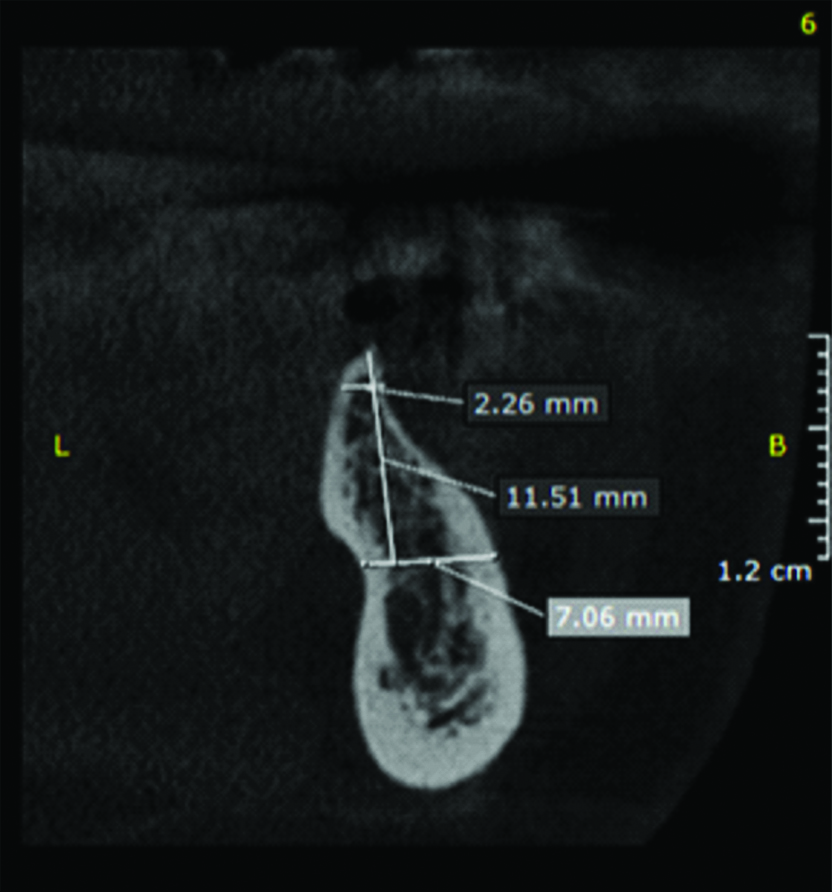
Ridge width 2 mm below the crest, 2 mm above the inferior alveolar canal and ridge height from the ridge crest to 2 mm above the inferior alveolar canal.
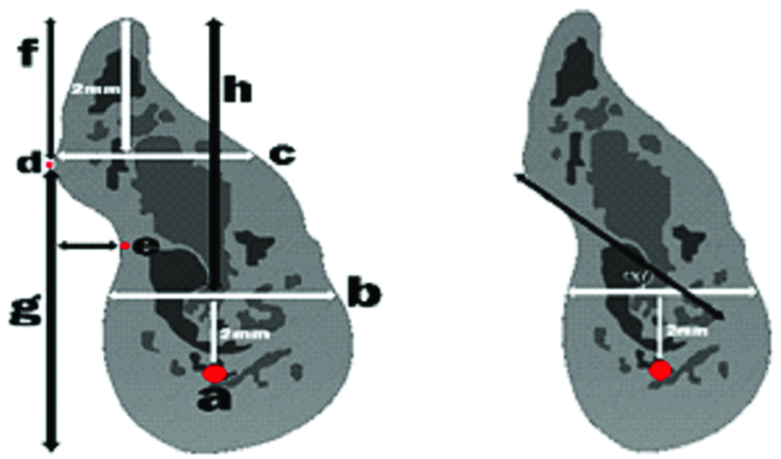
In cases with type U ridge morphology, in order to measure the depth of lingual undercut, a line tangent to the surface of the lingual ridge was drawn and the angle between this line and the line drawn 2 mm above the inferior alveolar canal was measured by the caliper of the software [Table/Fig-4]. The distance between the deepest point in the lingual surface and the line drawn perpendicular to the lingual surface was measured by the ruler of the software [4]. The distance between the most prominent point of the ridge in the lingual surface and the ridge crest and inferior border of the mandible was also measured [Table/Fig-5] [1].
Angle between the line tangent to the lingual ridge surface and the line drawn 2 mm above the canal.
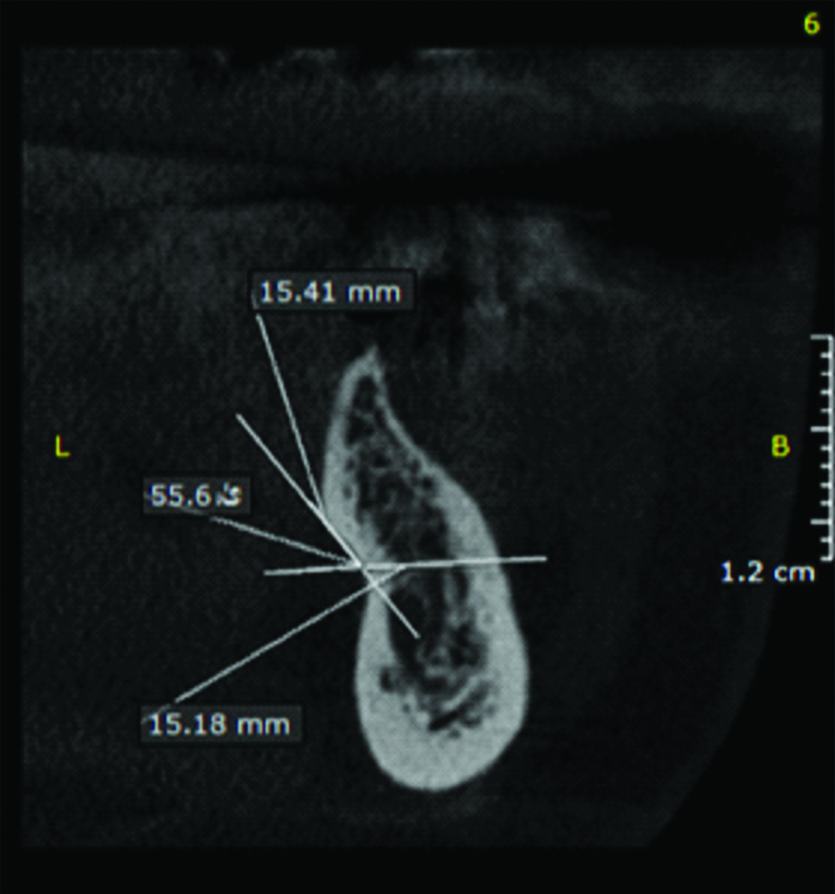
Distance from the deepest point of the undercut to the perpendicular line and the lingual surface and the distance between the most prominent point of the ridge in the lingual surface and the ridge crest and the inferior border of the mandible.
Statistical Analysis
Independent t-test and analysis of variance (ANOVA) were used to compare mean values of CBCT measurements between gender and age groups, respectively. Moreover, potential correlation between depth of lingual undercut/type of ridge and age was addressed. Statistical Package for Social Sciences (SPSS) version 20 was used to perform statistical analysis. The p-values less than 0.05 were considered statistically significant. To ensure reliability of the tool, the intra-class correlation coefficient was calculated.
Results
Of a total of 164 patients with a mean age of 43.9±12.3 years (range 18 to 82 years), 77 (47%) were males and 87 (53%) were females. The intra-class correlation coefficient was calculated to assess the agreement between the first and second observers and was found to be 94% and 99.5% for different variables, respectively. These values were acceptably high. The results showed that in terms of type of ridge morphology, type U had a frequency of 50% (47.6% in males and 52.4% in females), type C had a frequency of 26.2% (41.9% in males and 58.1% in females) and type P had a frequency of 23.8% (51.3% in males and 48.7% in females). Also, depth of lingual concavity was less than 2 mm in 29.4%, between 2-3 mm in 25.9% and over 3 mm in 44.7%.
[Table/Fig-6,7] show the mean values of the measured variables in males and females. Independent t-test showed that a significant difference existed between males and females in ridge height from the ridge crest to 2 mm above the inferior alveolar canal such that this distance was significantly greater in males (15.0 mm) than females (p=0.002).
Mean value of measured variables in males and females.
| Variable | Range (mm) | Gender | Number | Mean | Standard deviation | p-value |
|---|
| Ridge height | 5.7-62.2 | Male | 77 | 15 | 6.0 | 0.002 |
| Female | 87 | 12.7 | 2.3 |
| Ridge width (2 mm below the crest) | 1.7-26.6 | Male | 77 | 5.37 | 3.0 | 0.1 |
| Female | 87 | 4.76 | 1.5 |
| Ridge width (2 mm above the canal) | 4.5-16.6 | Male | 77 | 2.3 | 2.3 | 0.1 |
| Female | 87 | 1.8 | 1.8 |
| Angle | 40.0-79.0 | Male | 40 | 59.4 | 8.9 | 0.6 |
| Female | 42 | 60.2 | 9.8 |
| Undercut depth | 0.7-4.9 | Male | 40 | 2.9 | 1.0 | 0.6 |
| Female | 42 | 2.7 | 1.1 |
| Distance from the most prominent point to the inferior border of mandible | 4.0-16.4 | Male | 40 | 14.2 | 1.8 | 0.5 |
| Female | 42 | 13.8 | 2.7 |
| Distance from the most prominent point to the ridge crest | 9.9-24.5 | Male | 77 | 10.3 | 2.8 | 0.021 |
| Female | 87 | 8.9 | 2.5 |
Diagram of Mean value of measured variables in males and females.
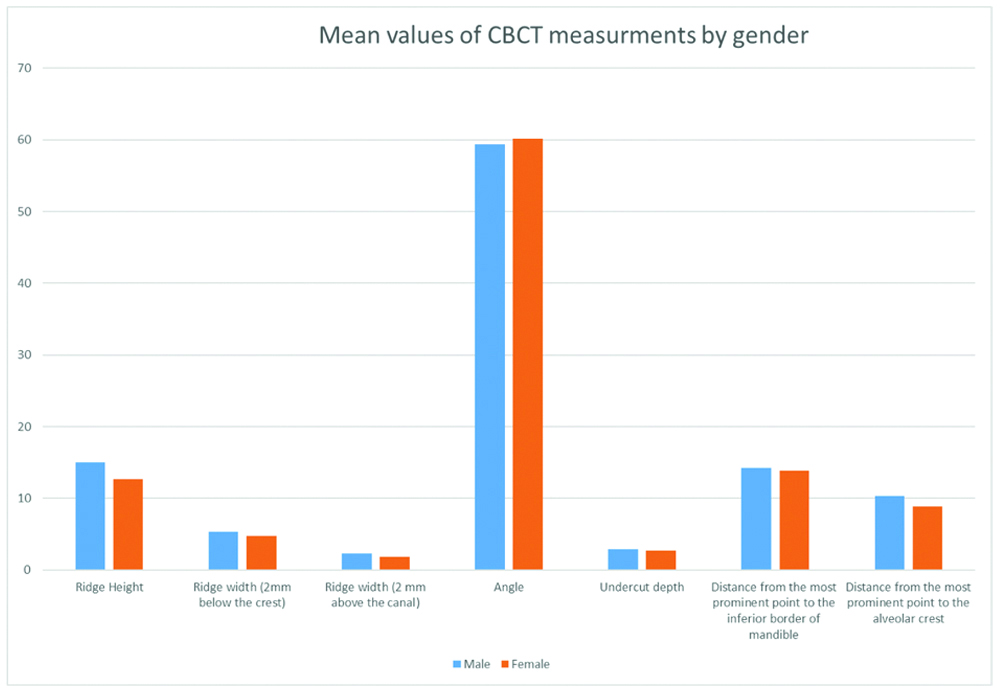
Also, the distance between the most prominent point of the ridge and the ridge crest was significantly greater in males (10.3 mm) than females (p=0.021). Other variables were not significantly different between males and females [Table/Fig-6]. The results of ANOVA revealed no significant difference between different age groups in any of the variables.
The chi-square test was used to assess the association between ridge morphology and age groups and found no significant association (p>0.05, [Table/Fig-8]).
Correlation of type of ridge morphology and age.
| Age group (years) | Ridge morphology type | Total | p-value |
|---|
| U | C | P |
|---|
| Younger than 30 (14.6%) | 12 (14.6%) | 6 (13.9%) | 6 (15.4%) | 24 (14.6%) | 0.6 |
| 30-45 (42.1%) | 34 (41.5%) | 22 (51.2%) | 13 (33.3%) | 69 (42.1%) |
| 45-60 (32.9%) | 26 (31.7%) | 11 (25.6%) | 17 (43.6%) | 54 (32.9%) |
| Over 60 (10.4%) | 10 (12.2%) | 4 (9.3%) | 3 (7.7%) | 17 (10.4%) |
| Total | 82 | 43 | 39 | 164 |
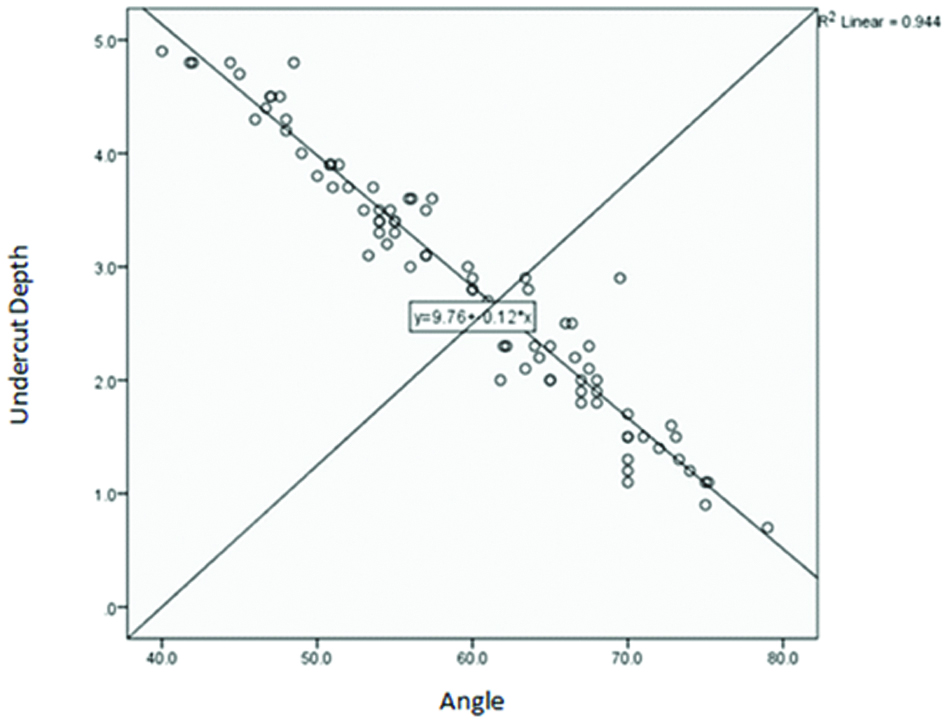
[Table/Fig-9] is the scatter plot of the lingual concavity depth and angle. To determine the correlation of depth of lingual concavity and other measured variables, the Spearman’s correlation coefficient was calculated. This value was 0.97 for the correlation of lingual concavity depth and angle. By an increase in angle, depth of lingual undercut decreased. [Table/Fig-10] shows the schematic view of measurements made on CBCT scans.
Scatter plot of the correlation of depth of lingual undercut with the angle between the line tangent to the lingual ridge surface and the line above the canal.
Schematic view of measurements made on CBCT scans. a: Inferior alveolar canal, b: line was drawn 2 mm above the inferior alveolar canal, c: line was drawn 2 mm below the alveolar crest, d: the most prominent point of the ridge, e: the deepest point in the lingual surface, f: the distance between the most prominent point of the ridge and the ridge crest, g: the distance between the most prominent point of the ridge in the lingual surface and inferior border of the mandible, h: the vertical distance between the ridge crest and the line drawn 2 mm above the inferior alveolar canal, α: the angle between the line tangent to the surface of the lingual ridge and the line drawn 2 mm above the inferior alveolar canal.
Discussion
Presence of lingual concavity in the posterior mandible can increase the risk of lingual cortex perforation in implant placement. On the other hand, the amount of bone at the site of implant placement must be evaluated prior to implant placement since, it plays an important role in implant Osseointegration [1,4]. Thus, this study assessed the morphology and dimensions of bone in the posterior mandible in patients requiring implant placement at the site of mandibular first molar. Cross-sectional CBCT images of 164 patients including 77 males and 87 females in the age range of 18 to 82 years were evaluated. The results showed that type U ridge morphology had a prevalence of 50%; this rate was 26.2% for type C and 23.8% for type P. Nickenig HJ et al., reported that type U had the highest prevalence (68%) in their study followed by type P (21%) and type C (11%) [9]. Watanabe H et al., classified the morphology of the mandible into three groups of A, B and C. In type A, the concavity was in the lingual side. In type B, the concavity was in the buccal side and type C was round ridge. Watanabe H et al., reported that type C was the most common form (59%) followed by type A (36%) [2]. In a study by Chan HL et al., type U had the highest prevalence (66%) [5]. These differences may be due to different classification systems used in studies, different races of study populations and presence/absence of teeth [2]. In the study by Watanabe H et al., patients were dentulous while in our patients; mandibular first molars had been extracted. However, both studies showed considerably high prevalence of lingual concavity.
In our study, in 29.4% of type U patients, depth of the lingual concavity was less than 2 mm; in 25.9%, this depth was 2-3 mm and in 44.7%, it was over 3 mm. In other words, 70.6% of patients with type U ridges had lingual undercuts with more than 2 mm of depth. In a study by Nickenig HJ et al., the mean depth of the lingual undercut was 3.7 mm (similar to our results with a mean undercut depth of over 2 mm) [9]. Lingual concavity deeper than 2 mm can be a potential risk for lingual plate perforation and complications during implant placement. Its high prevalence in different populations highlights the need for accurate assessment of implant site prior to implant placement. Kamburoglu K et al., reported the mean depth of sublingual concavity to be 1.3 mm [12] but Quirynen M et al., reported the lingual concavity depth to be 6±2.6 mm in 2.4% of the jaws [7]. These differences may be due to different reference points, distances measured and number of dentulous and edentulous patients [12].
In our study, similar to that of Parnia F et al., no significant differences were noted between age and depth of lingual undercut (p>0.05). This may be due to the fact that severe ridge resorption depends on many factors such as bone density and anatomy of the ridge [1]. However, Uchida Y et al., stated that changes in the volume of alveolar bone during edentulism causes a reduction in the depth of sublingual concavity [13].
In our study, no significant association was noted between type of ridge morphology and age and sex of patients; this was in line with the results of Chan HL et al., [4]. Yoon TY et al., found that the prevalence of lingual undercut in the posterior mandible had no significant association with sex or race but had a significant association with age such that in patients over 63 years, the prevalence of lingual undercut increased [14]. This finding may be due to bone resorption in edentulous areas, which increases with age [15].
In our study, ridge height was significantly different in males and females. Similarly, Watanabe H et al., [2] showed that ridge height was significantly greater in males than females and this can be due to faster bone resorption in females. Also, Zhang W et al., measured the mandibular ridge height by measuring the distance from the alveolar crest to the border of the mandible and the distance from the alveolar crest to the inferior alveolar canal and concluded that ridge height in males was significantly greater than that in females [16]. However, in contrast to the two afore-mentioned studies, Chan HL et al., found no significant difference in ridge height between males and females [4]. This difference may be due to the fact that number of females was twice that of males in the study by Chan HL et al., while in our study, number of males and females was close (77 males and 87 females). Also, difference in selected reference points for measurements and difference in duration of edentulism may explain the difference in the results [4].
In our study, the distance between the most prominent point of the ridge and the ridge crest in males was significantly greater than that in females. But in the study by Chan HL et al., this distance was not significantly different in males and females [4]. Controversy in the results of the two studies may be due to different measurement methods since Chan HL et al., measured the distance from the most prominent point of the ridge to the cementoenamel junction while we measured the distance from the most prominent point of the ridge to the ridge crest [4].
In our study, ridge width was not significantly different between males and females; this finding was similar to that of Chan HL et al., [4]. But Zhang W et al., measured ridge width as the distance between the external surface of buccal and lingual cortical plates and concluded that mandibular width was significantly greater in males than females [16]. These differences are probably attributed to the method of measurement and inclusion of dentate areas in the study.
Periapical and panoramic radiographs are often used to assess the site of implant placement. However, these techniques are two-dimensional and cannot provide adequate information about bone width [8]. CBCT compared to computed tomography has advantages such as lower patient radiation dose and cost and higher resolution and accuracy [1,17]. Thus, since lingual concavity is a potential risk in implant surgery, assessment of size and morphology of the mandibular ridge by use of CBCT can greatly help in prevention of possible complications.
Limitation
Since this study was performed on CBCT scans of patients retrieved from the archives, we did not had access to patients and therefore, we did not know how long had passed since the extraction/loss of first molars. We did not had adequate information about the presence/absence of parameters affecting bone tissue such as metabolic disorders in patients either. Therefore, these factors might have affected the results obtained in this study.
Conclusion
Type U ridge morphology had the highest prevalence in the respective site in our study population followed by type C and type P. Also, 70.6% of patients with type U ridge had lingual undercuts deeper than 2 mm. No significant association was noted between ridge morphology and age or sex. The distance from the most prominent point of the ridge to the ridge crest and ridge height measured from the ridge crest to 2 mm above the inferior alveolar canal in males were significantly greater than those in females. Ridge width was not significantly different between males and females. On the other hand, by an increase in angle, depth of lingual undercut decreased.