Diastema is a distinctive gap or space between two teeth. It is also called as “open-teeth” or “gapped teeth” [1]. Maxillary midline diastema being most common aesthetic problem in mixed and early permanent dentitions i.e., during ugly duckling stage but is usually a part of normal dental development during this stage (self-correcting malocclusion) [2]. Koora K et al., described midline diastema as anterior midline spacing greater than 0.5 mm between the proximal surfaces of adjacent teeth [3]. Aetiology of maxillary midline diastema can be a missing tooth, peg shaped lateral, midline supernumerary teeth, tooth size and arch length discrepancy, proclination of the upper labial segment, prominent frenum or oral habits, muscular imbalances, physical impediments and abnormal maxillary arch structure [4,5].
Diastemas based on tooth-size discrepancy are most amenable to restorative and prosthetic solutions. The most appropriate treatment is orthodontically closing the midline diastema. Labial and lingual orthodontics can be used for similar tooth movements, but they differ considerably in their biomechanics due to point of force application. In addition to their relative unobtrusiveness, lingual appliances obviate the need for etching the labial enamel, and the displacement of each tooth can be observed more clearly, with respect to the labial technique. Lingual technique is considered difficult and technique sensitive due to lingual anatomical variations, inability of direct access to lingual aspect of tooth and thereby resulting in accurate bracket positioning [3].
The main difference between the labial and lingual techniques is the distance between the point of application of the force that is transmitted through the bracket and the centre of resistance of the tooth. Analytical and experimental method like photoelasticity, inferometric holography and strain gauges have been traditionally used to assess the dental stresses during orthodontic tooth movement. Major limitation of these methods was its inability to detect the microenvironmental changes around the Periodontal Ligament (PDL) and within the bone [6].
The Finite Element Method (FEM) was initially developed in 1940s’ by R Courant for structural analysis in aeronautical engineering [7]. In 1972, Yettram strarted using FEM for orthodontic purposes. [8]. FEA also known as FEM is a method for numeric solution of field problems. Finite elements are formulated mathematically by differential equation or by integral expression. Individual finite elements are small pieces of a structure connected at points called nodes. This assemblage of finite elements is called finite element mesh [9]. Middleton J et al., stated that data obtained from FEA is more accurate than any of the other experimental methods. It allows for complete control over the variables in use while studying a homologous sample. It is non-invasive technique that accurately analyses the stress and strain induced by orthodontic forces in periodontium and alveolar bone [10].
Finite element method can be used to study the action of orthodontic forces on craniofacial complex. It is instrumental in orthodontic research for assessing stress distribution in periodontal ligament, alveolar bone and archwire during tooth movement. It makes the effect of orthodontic forces more predictable [11].
Lingual orthodontics is gaining popularity day by day. However very few information is present in literature regarding physiologic reaction that occurs after force application, efficacy and rate of tooth movement in lingual orthodontics when compared with labial orthodontics. Therefore, this study was designed for comparison of aforesaid parameters in midline diastema cases with both lingual as well as labial orthodontics. The main aim and objectives of this study was to compare the stress generated (structure) during midline diastema closure using labial and lingual orthodontics using Three Dimensional (3D) finite element models, to compare the instantaneous displacement of tooth (maxillary right and left central incisor) under labial and lingual loading during the midline diastema closure and to compare the efficacy of labial and lingual orthodontics for the closure of midline diastema.
Materials and Methods
This in vitro research was conducted in December 2017 at the Department of Orthodontics and Dentofacial Orthopaedics, Chhattisgarh Dental College and Research Institute, Rajnandgaon, Chhattisgarh, with technical assistance from Tejvi Techno Solution, Bengaluru, Karnataka, India. Ethical clearance was obtained from the institution.
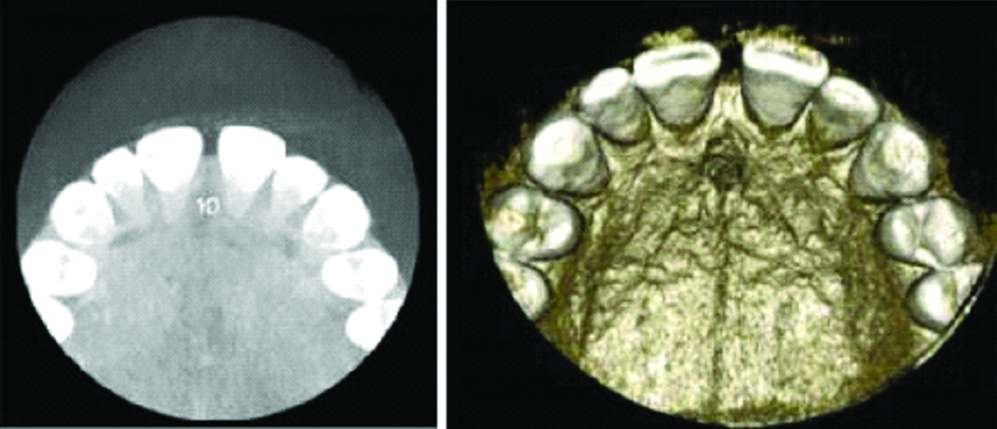
A patient of midline diastema was scanned by cone-beam computed tomography using a NewTom 3G (QR Srl, Verona, Italy) after taking his informed consent [Table/Fig-1]. The exposure parameters were: 110 kV, 0.50 mA, 12-inch field-of-view and 5.4-second exposure time.
CBCT image of midline diastema.
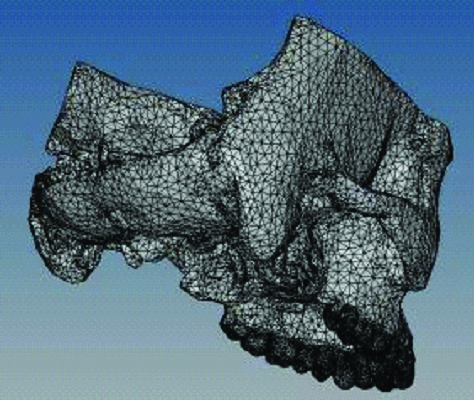
CBCT of the patient was then converted in geometrical form initially through STL (StereoLithography) file format [Table/Fig-2]. STL format was then imported in to hypermesh for finite element mesh.
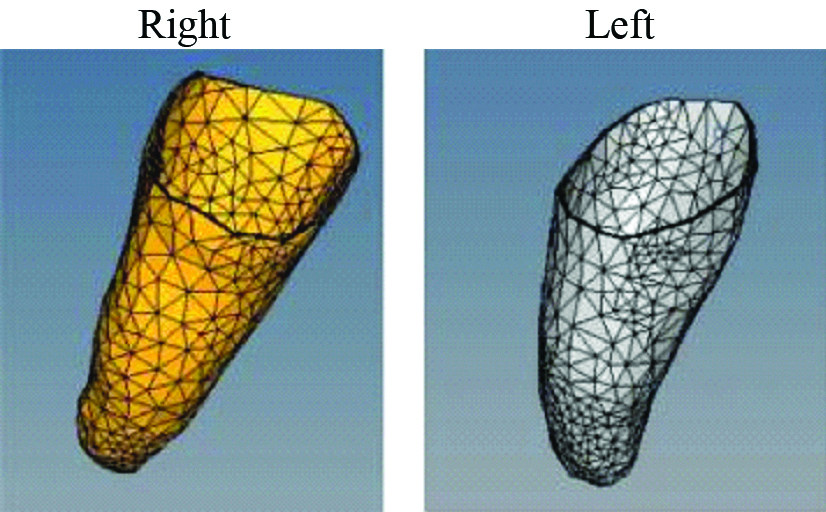
Mechanical properties of involved structure and material properties are given in [Table/Fig-3,4]. Bone geometry, teeth geometry, periodontium of 0.2 mm thickness around the teeth geometry was created [12-14]. The brackets of 0.018″ slot with the wire of 0.017″×0.025″ SS was built and assembled with teeth [Table/Fig-5,6 and 7].
Mechanical properties of involved structure.
| Details | Young’s Modulus (N/MM2) | Poison’s Ratio |
|---|
| Enamel | 84100 | 0.33 |
| Dentine | 18300 | 0.31 |
| PDL | 6.8×0-1 | 0.49 |
| Cementum | 15000 | 0.31 |
| Pulp | 2.03 | 0.45 |
| Cortical Bone | 13.7×109 | 0.3 |
| Trabecular Bone | 1.3×109 | 0.3 |
| Details | Young’s Modulus (N/MM2) | Poison’s Ratio |
|---|
| Teeth | 18600 | 0.31 |
| Wire, Brackets | 200000 | 0.3 |
| Peridontium | 0.667 | 0.45 |
| Bone | 10600 | 0.3 |
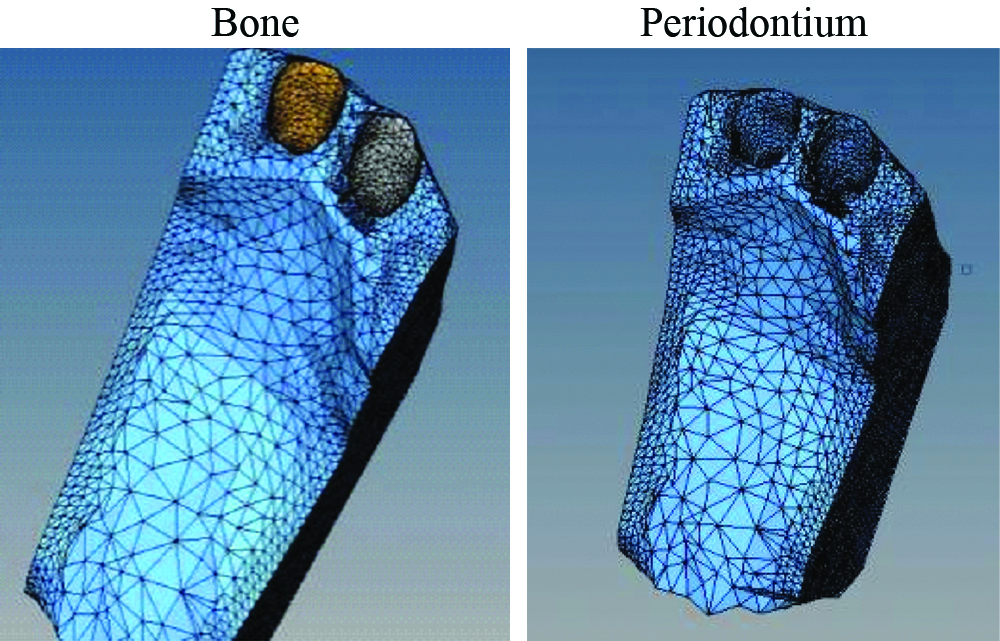
Mesh of the periodontium (0.2 mm thickness).
The teeth socket with bone and periodontium.
Complete assembly from labial and lingual side.
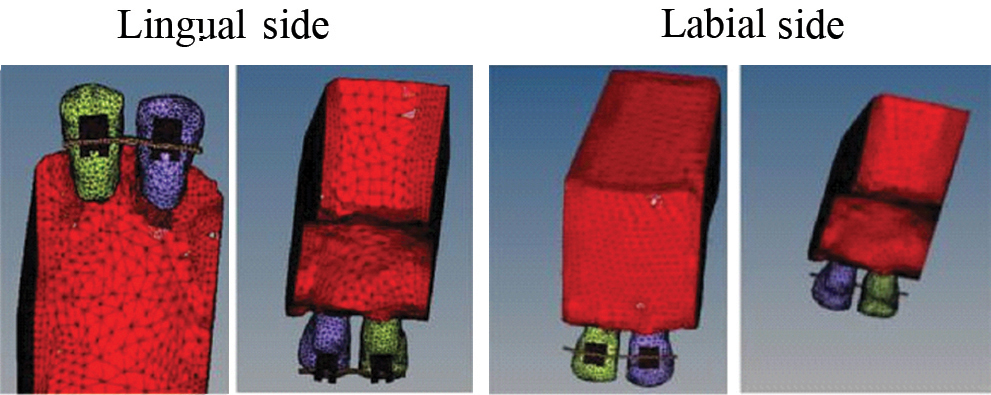
Mesh details from labial and lingual surface are described in [Table/Fig-8].
Labial and lingual mesh detail.
| Details | Labial | Lingual |
|---|
| Elements | Nodes | Elements | Nodes |
|---|
| Total | 73598 | 18352 | 73581 | 18341 |
| Bone | 38775 | 8974 | 18775 | 8974 |
| Periodontium | 5097 | 3508 | 3097 | 3508 |
| Teeth | 15148 | 3811 | 15148 | 3811 |
| Bracket | 14478 | 3718 | 14478 | 3718 |
| Wire Element | 100 | 101 | 83 | 84 |
The members were meshed separately and finite element connectivity was maintained for accurate results. Four noded tetrahedral elements were used to mesh the geometry. Coupling constraints along geometrical contacts were created for simulation of the loading process using algor program. The top outer geometry was constrained in all directions. The force of 100 grams (50 grams from each side) was applied for closure of midline diastema [15].
Results
The analysis results were captured to assess movement of the teeth towards the closure of the gap.
The result obtained during finite element analysis expressed visually with colour mapping, depicting intensity of the parameter of interest on labial technique as well as lingual technique. In case of this model, the parameters include: stress and instantaneous displacement of tooth using labial as well as lingual technique. Stress component such as vonmises stress in the bone, teeth, bracket, periodontium, and over all stress is calculated using labial and lingual technique. Displacement of teeth and overall displacement was seen in labial and lingual technique.
[Table/Fig-9] shows the maximum stress and instantaneous displacement of tooth for closure of midline diastema from labial and lingual orthodontics.
Maximum stress and displacement.
| Stress | Labial Technique | Lingual Technique |
|---|
| Von Mises stress in bone | 0.000356 Mpa | 0.000114 Mpa |
| Von Mises stress in teeth | 0.002442 Mpa | 0.000754 Mpa |
| Von Mises stress in bracket | 0.013 Mpa | 0.003 Mpa |
| Von Mises stress in periodontium | 0.000071 Mpa | 0.000025 Mpa |
| Overall stress | 2.28932 Mpa | 1.95 Mpa |
| Displacement of tooth | 0.0000118 mm | 0.00000395 mm |
| Overall displacement | 0.0000185 mm | 0.00000577 mm |
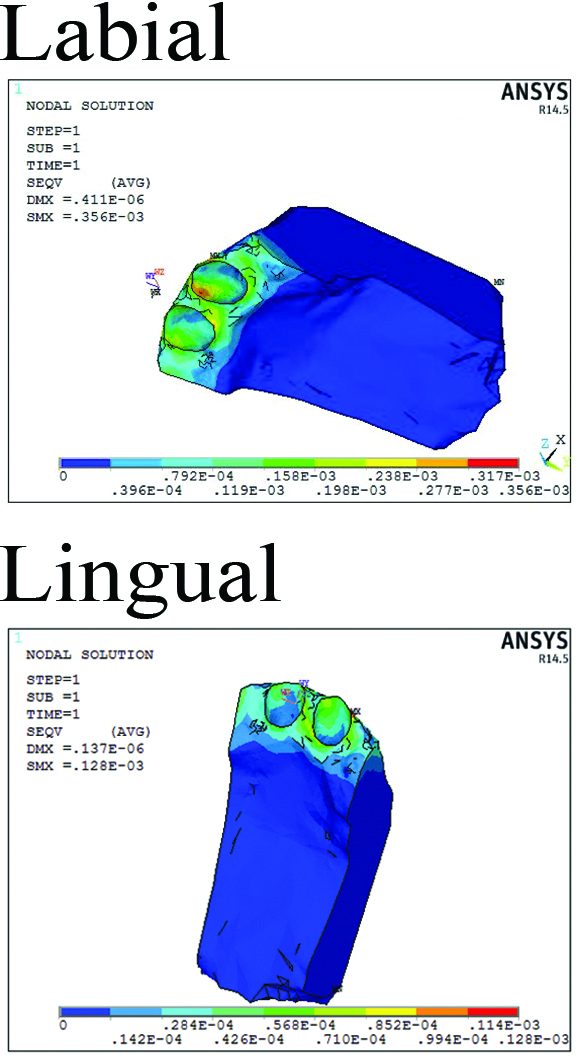
Von Mises Stress in the Bone
After applying force for closure of midline diastema, maximum stress 0.000356 Mpa was observed using labial technique, whereas 0.000114 Mpa was observed using lingual technique. Maximum stress location is shown by red colour along with a symbol of Mx. The colour code shows variation of stress along the bone geometry in [Table/Fig-10a].
Von Mises stress in bone.
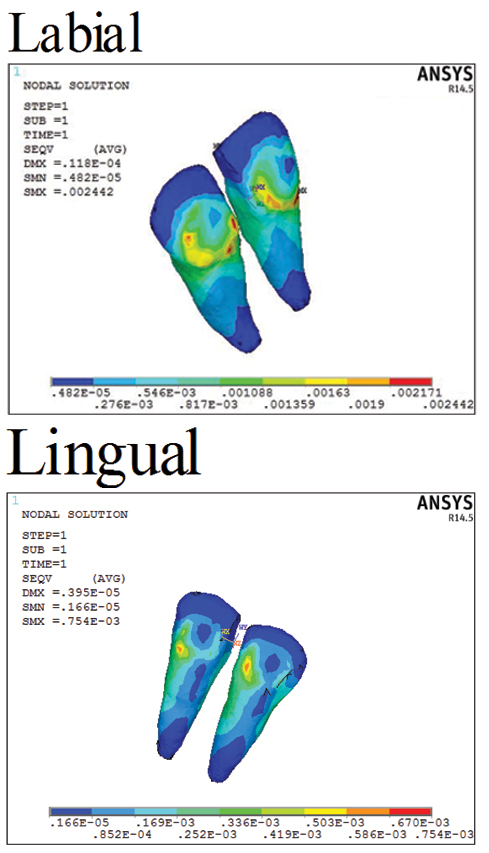
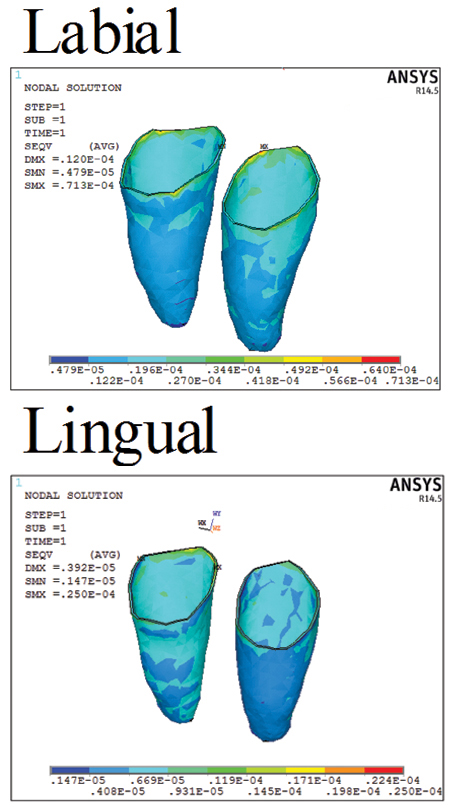
Vonmises Stress in the Teeth
Maximum stress of 0.002442 was observed for the teeth geometry in labial technique whereas 0.000754 was observed from lingual loading. Maximum stresses are shown by red colour region as in [Table/Fig-10b].
Von Mises stress in teeth.
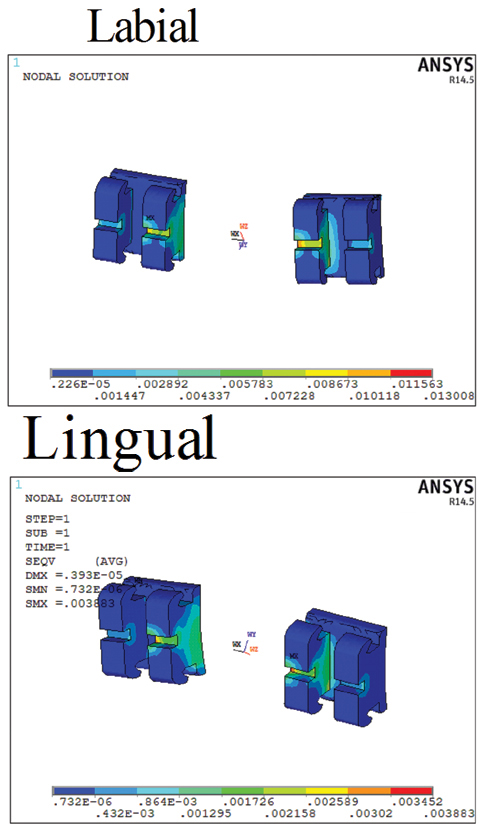
Von Mises Stress in Brackets
Maximum stress observed in bracket from labial loading was around 0.013 Mpa and 0.003 Mpa by using lingual technique as shown in the [Table/Fig-10c] with colour representation in the brackets.
Von Mises stress in brackets.
Von Mises Stress in the Periodontium
Maximum stress in periodontium was around 0.000071 Mpa in labial technique whereas from lingual technique it was around 0.000025 Mpa as shown in [Table/Fig-10d] with colour representation.
Von Mises stress in Periodontium.
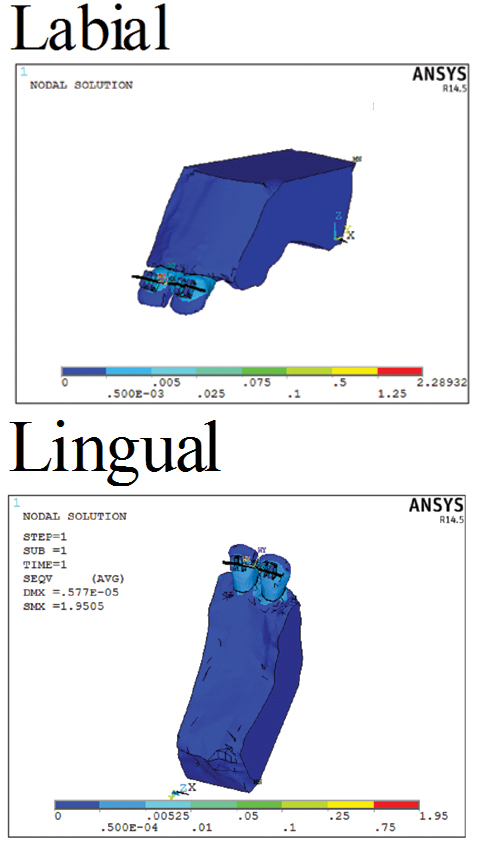
Over All Stress
Maximum stress of 2.28932 Mpa was seen using labial technique and 1.95 Mpa from lingual technique as shown in the [Table/Fig-11a] by red colour extreme value. The status bar with 9 colour representation shows variation of stress from zero. The stress in the individual members helps in finding the effect of loading on the members of the assembly.
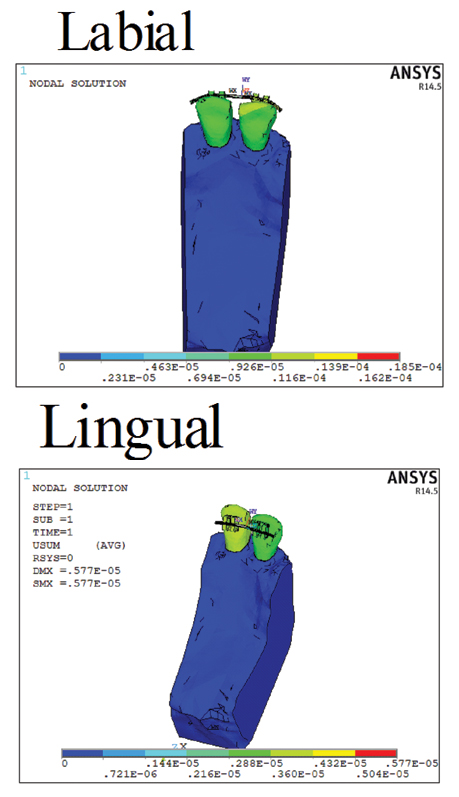
Overall Displacement
Maximum displacement value of 0.0000185 mm was observed using labial technique and 0.00000577 mm using lingual technique as shown in the [Table/Fig-11b] by red colour value in the status bar. More stress and displacement of teeth for closing the gap can be observed for labial loading compared to the lingual loading. By applying equal force labially and lingually, more bodily movement is seen in labial mechanics whereas lingual mechanics shows mesial crown tipping as well as bodily movement.
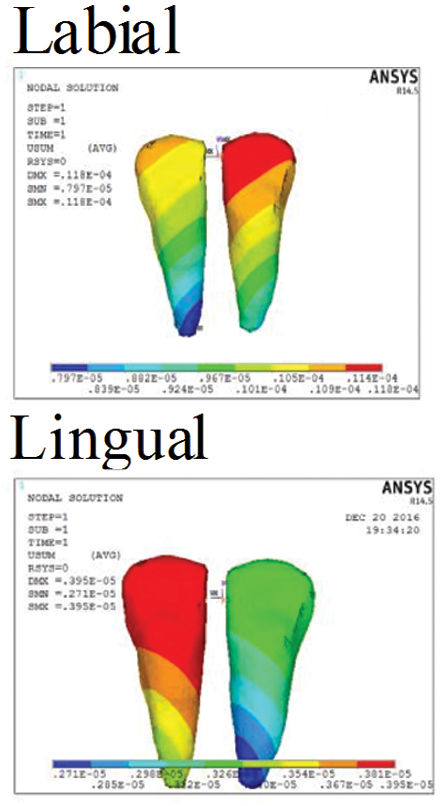
Displacement of Tooth
The [Table/Fig-12] shows displacement of the tooth. Maximum displacement was around 0.0000118 mm from labial technique and 0.00000395 mm using lingual technique. The colour pattern shows variation of displacement along the teeth geometry. The crest portion has the maximum displacement compared to the other region.
Discussion
The 3D FEM used in the present study provides the freedom to simulate orthodontic force applied clinically keeping in mind the material properties, load applied and boundary conditions and to analyse the response of the dentition to the force in labial and lingual orthodontics [16]. Initially, the objective of the present study was to compare the biomechanical responses to labial and lingual application of an orthodontic force on a maxillary midline diastema case. Finally, we evaluated the instantaneous displacement of the maxillary incisor through the FEM. To complete the picture, the stress distribution within the surrounding bony support was also calculated, to identify regions of tension and compression.
In this view, a model of maxillary midline diastema was developed with defined material properties in [Table/Fig-4]. The model was analysed to calculate stress and instantaneous displacement using labial and lingual technique, when force was applied from right and left central incisor for closure of diastema.
In this study, overall maximum stress seen in labial technique was 2.28932 Mpa as compared to lingual technique which was approximately 1.95 Mpa. However, significant difference was seen in stress of bone, teeth, periodontium by using labial as technique compared with lingual technique. Differences between the labial and lingual morphology have an important impact on the biomechanics of lingual orthodontic. Tooth movement depends on line of force application relative to centre of resistance of the tooth. Since the point of force application is different in labial and lingual technique therefore line of force relative to centre of resistance is different producing different tooth movements [17].
The lingual tooth aspect is more complex and versatile, therefore, every change in the bracket position on the lingual side may cause unpredictable or an extensive change in the torque and vertical tooth height [18]. Changing a bracket position on the lingual side will have a greater effect on the final tooth position than the same change when applied on labial bracket. These differences between the labial and the lingual technique can influence even small tooth movement [19].
Lombardo L et al., observed less lingual movement of the canines with the lingual archwire than with the labial appliance which may be due to the transverse bowing effect of the lingual retractional forces [20]. However, it was also observed that mesial movement of the maxillary incisor with the lingual archwire was less as compared with the labial appliance. Sung SJ et al., noted vertical bowing due to lingual tipping of incisors and mesial tipping of molars during canine retraction. He also reported transverse bowing due to rotation of the canine and buccal displacement of the premolars [21]. However, Gorman JC and Richard J, compared the treatment effect with labial and lingual fixed appliances and found no statistically significant differences in treatment results [22].
Lombardo L et al., compared the biomechanical response of mandibular incisors with labial and lingual force applications with a three-dimensional finite element model; apically directed vertical forces applied at the lingual points produced more uniform tooth displacements (intrusion) and stress distributions [12]. However, in this study by applying equal force labially and lingually more bodily movement is seen in labial mechanics whereas lingual mechanics shows tipping as well as bodily movement. Ranjit HK et al., studied the stress distribution pattern in maxillary central incisors with different root morphologies using FEM. They concluded that teeth with dilacerated morphology are at higher risk of root resorption [23]. Among others, Liang W et al., supports the conclusions that bodily (translatory) displacement of a tooth is more efficient by the application of the force on labial side [15].
Limitation
Although Fem is a non invasive method to determine precise forces used in orthodontics, yet sound knowledge of software is required which can be deterrent when proper digital aids are not available. Another limitation is the unavailability of accurate mathematical properties for tooth and bone in various regions. One must be aware of material properties, load applied and boundary conditions. Like any other technique, this also needs improvement so that more accurate results could be obtained. Third limitation of this study is that central incisors considered had normal root morphology, although studies in past have dealt with stress distribution in varying root morphology.
Conclusion
For a plausible system of forces acting on an upper incisor, bodily movement occurs when the force is applied labially, whereas a force applied lingually creates a bodily movement and intrusion of the upper incisor. Based on the results of this study, we can reckon that labial and lingual orthodontics has little effect on the type of tooth movement.