Wound infections in fishermen are more common mainly due to their working environment and the things they handle during their work [1]. Mostly fishermen have an unfavourable lifestyle and are vulnerable for injuries, other diseases [2]. Lacerations due to inanimate objects, puncture wounds due to fish hooks, propeller injuries, minor abrasions, trauma, water moccasin snake bites, Injuries by fish bones and spines are more common among fishermen during fishing [3]. At the time of injury, minor grazes and cuts remain unnoticed, but most often bacteria are transported to the wound from piece of metal, gut and also from fish slimes that leads to inflammation and formation of pus [4]. Cellulitis develops within 48 hours of exposure of the wound to water, which later progress to bullae formation, ecthyma gangrenosum, pustular eruptions myonecrosis and subcutaneous nodules [5]. Infection of open wounds is one of the major problem [6]. Moreover, poor sanitary conditions among such a community can result in further contamination of the wound which can even lead to surgical removal of damaged tissue and amputation [1]. Patients with hypertension, diabetes mellitus, cardiovascular diseases, chronic liver disease, immunological disorders such as HIV, Hepatitis and Leukaemia, are at a higher risk of developing sepsis [7]. The array of microorganisms causing soft tissue infection on exposure to water is extremely large [8]. Superficial trauma on water exposure are largely contaminated by Gram-negative bacilli which constitute the largest group of aquatic pathogens that cause skin infection [9], other pathogens include few gram-positive bacteria, mycobacteria and few marine bacterial pathogens such as Vibrio vulnificus, Mycobacterium marinum, Erysipelothrix rhusiopathiae and Aeromonas hydrophila [3]. Local trauma/injury associated with salt water/fresh water exposure can result in soft tissue infections. Salt water harbours unique bacteria which can further contaminate the wound causing secondary infection [10]. Fishing is not an occupation, its a way of life with own values and tradition. According to the geographical data, the coastal areas in and around Puducherry Union Territory in India is largely occupied by fishermen community [11] with 15 fishing villages in Puducherry district where 21,237 men are actively involved in fishing and fishing-related activities [12,13]. The working environment in fisheries sector is strenuous, tiring and exhausting [14]. Despite fishing being an arduous, dangerous and economically important occupation, very few researchers have been reported on fishermen safety and health and there is not much literature related to occupational injuries and infections of the fishermen community in this region [15]. Hence, the present study focuses on the bacterial pathogens and its drug resistance pattern in wound due to occupational injury among fishermen community of Puducherry and to assess their health seeking attitude.
Materials and Methods
A cross-sectional study was done among the fishermen residing in coastal areas of Puducherry conducted over a period of six months from February to July 2015 by the Department of Microbiology, Sri Lakshmi Narayana Institute of medical sciences, Pondicherry, India. The study population included only fishermen who were actively involved in fishing and fishing-related activities living in the coastal areas of Puducherry with any type of wounds. Ethical clearance (IEC/C-P/06/2014) for the study was obtained and Informed consent was obtained from all participants included in the study. The structured questionnaire was used to collect information regarding the type of fishing methods employed, habits of alcoholism, smoking, pan chewing, details of the clinical history was collected such as symptoms after injury, duration of wound, site of injury, source of injury, any vaccination taken after injury, visit hospital/treatment after injury and observation of records regarding the type of wound was done. Additional information regarding the socioeconomic status and health seeking attitude was collected. 292 Pus/wound swabs were collected from the wound of fishermen who were enrolled for the study visiting 13 villages of fishermen community in and around Puducherry. The sterile swab was held in contact with the wound for at least five seconds before any debridement was done [9,16]. The samples were placed in the sterile tube containing Amie’s transport medium without charcoal [17] in an ice pack box and transported carefully to the laboratory within 12 hours. The wound swabs were inoculated on to 5% Sheep blood agar, Chocolate agar, MacConkey agar, Thioglycollate broth and incubated at 37°C for 24 hours and prolonged incubation was done for 48 hours, if there is no growth after 24 hours. The growth was interpreted as no growth if the plates were found sterile after 48 hours polymicrobial if two or more species of a single microbe were present and mixed bacterial flora if >3 types of organisms were present. The organisms were identified/differentiated based on Gram staining, motility, catalase test, oxidase test and other routine biochemical tests like indole, methyl red test, mannitol motility test, Voges Proskauer test, citrate, urease, triple sugar iron agar test and coagulase test as per Cowan and Steels Manual 9. Antimicrobial susceptibility of the isolated organism was performed by Kirby Bauer disk diffusion method using CLSI guidelines [18,19] on Muller Hinton agar plate, the following antibiotics were tested- Amikacin 30 mcg, Gentamycin 10 mcg, Nitrofurantoin 300 mcg, Ceftazidime 30 mcg, Amoxyclav 30/10 mcg, Cefepime 30 mcg, Co-trimoxazole 25 mcg, Ceftazidime-clavulanic acid 30/10 mcg, Clindamycin 2 mcg, Vancomycin 30 mcg, Cefoxitin 30 mcg, Imipenem 10 mcg, Meropenem 10mcg, Imipenem with EDTA, Aztreonam 50 mcg, Gentamycin 120 mcg and Erythromycin 15 mcg. The zone diameter was measured.
Results
This study included 292 fishermen with wound due to occupational injuries. Of the 292 wounds swab/pus collected and cultured, 162 (55.5%) of the samples showed the single type of growth, 47 (16.1%) showed polymicrobial growth, 14 (4.8%) had mixed growth and 69 (23.6%) showed no growth [Table/Fig-1]. The bacteriological profile of wound/pus swab is summarised in [Table/Fig-2].
The results of pus/wound culture.
| S.No | Culture Result | No. of samples | Percentage (%) |
|---|
| 1. | Samples with Single Type of Growth | 162 | 55.5% |
| 2. | Samples with Polymicrobial Growth | 47 | 16.1% |
| 3. | Samples with Mixed Bacterial Flora | 14 | 4.8% |
| 4. | No Growth | 69 | 23.6% |
| Total Number of Samples | 292 | 100% |
Bacteriological profile of wound in culture positive cases.
Total number of isolates: 256
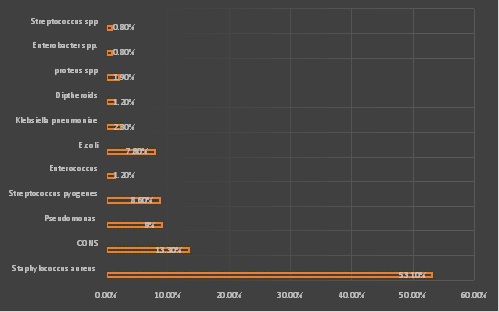
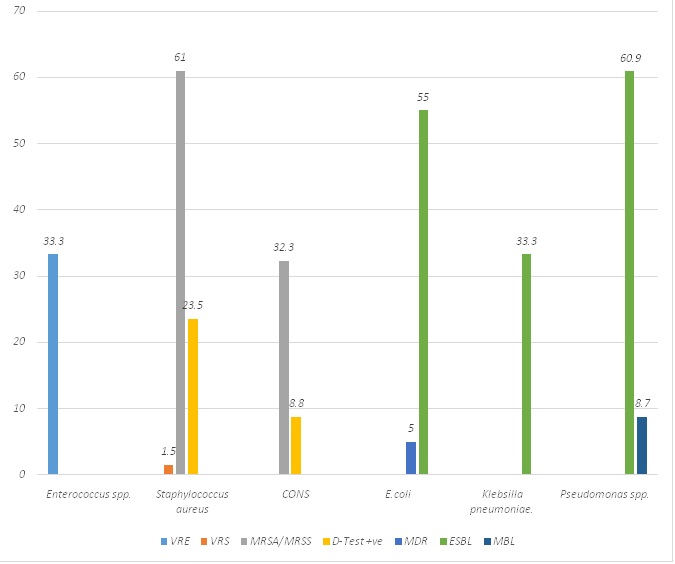
A total of 256 isolates were obtained from culture positive cases. In the present study, the most common pathogen isolated was Staphylococcus aureus 136 (53.1%) followed by Coagulase Negative Staphylococcusspp. (CONS) 34 (13.3%), Pseudomonasspp. 23 (9.0%), Streptococcus pyogens 22 (8.6%), E.coli 20 (7.8%) and other pathogens isolated were Klebsiella pneumoniae 6 (2.3%), Proteusspp. 5 (1.90%), Enterococcusspp. 3 (1.20%), Diphtheriods 3 (1.20%), Enterobacterspp. 2 (0.80%) and Streptococcusspp. 2 (0.80%). The results of Antimicrobial Susceptibility Testing (AST) presented in [Table/Fig-3] revealed 83 (61.0%) of Staphylococcus aureus were Methicillin-Resistant Staphylococcus Aureus (MRSA), 32 (23.5%) were D-test positive (inducible clindamycin resistance) [Table/Fig-4] and 2 (1.5%) were resistance to vancomycin. Out of 34 CONS, 11 (32.3%) were methicillin-resistant, 3 (8.8%) showed inducible clindamycin resistance and 1 (33.3%) Vancomycin Resistant Enterococcus (VRE) was found in the study. The AST results of gram-negative bacilli revealed 14 (60.9%) of Pseudomonas spp., 11 (55.0%) of E.coli and 2 (33.3%) of Klebsiella pneumoniae isolates were ESBL. In the present study, 2 (8.7%) of Pseudomonas spp. reported was Metallo β lactamase (MBL) producers and 1 (5.0%) Multidrug Resistant (MDR) E.coli was isolated. In the present study out of 292 fishermen enrolled 201 (68.8%) were found to use non mechanised fishing crafts such as catamarans and canoes. Mechanised fishing methods were employed by 63 (21.6%) and 28 (9.6%) of fishermen used motorised fishing crafts. Age wise distribution of fishermen with wound revealed 108 (36.9%) of the study subjects were in the age group 25-35 years. followed by 82 (28.1%) were <25 years [Table/Fig-5]. Details of clinical findings and analysis of health seeking behaviour of fishermen is listed in [Table/Fig-6]. Among the 292 study subjects 89 (30.5%) of fishermen presented wound/injuries in the lower extremities, 86 (29.5%) presented injuries in the upper extremities followed by 49 (16.8%) in other body sites. In the present study nearly 74 (25.3%) of the study population reported injury due to fishing gear, 68 (23.3%) of injuries occurred while handling fishing nets, 62 (21.2%) of fishermen were injured due to fish hooks and forks. About 15 (5.1%) reported due to spines while sorting the fishes. In the study, 27 (9.2%) fishermen suffered from major injuries. Minor injuries such as laceration in 203 (69.5%) and cuts were observed in 42 (14.4%). The investigation regarding the health seeking behaviour of fishermen in this community showed 275 out of 292 (94.2%) of fishermen with injury/wound has not taken any vaccination after injury. A total of 269 (92.1%) of the study subjects has failed to avail first aid after injury and 254 (87.0%) reported lack of the visit to hospital after injury [Table/Fig-6].
Antimicrobial resistance pattern of the isolated strains.
VRE: Vancomycin resistance enterococci; ESBL: Extended spectrum β lactamases; MBL: Metallo β lactamase; MDR: Multi drug resistance; MRSA: Methicillin resistant staphylococcus aureus; MRSS: Methicillin resistant staphylococcusspp.; D- Test +Ve: Inducible Clindamycin Resistance; VRS: Vancomycin resistant staphylococcus aureus
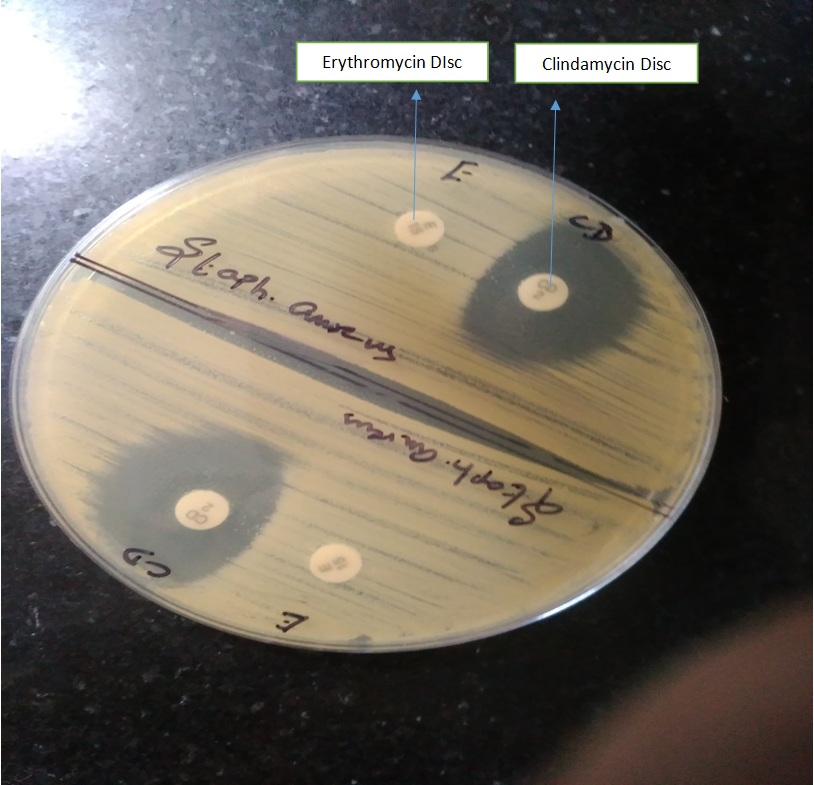
AST plate with D- test +ve: Inducible clindamycin resistance shown by Staphylococcus aureus.
Socio demographic characteristics of study subjects/study population and age wise distribution of fishermen with wound infection.
| S. No. | Demographic characteristics | Subjects (n=292) | Percentage (%) |
|---|
| 1. | Type of fishing methods used |
| a. Mechanised | 63 | 21.6% |
| b. Non- mechanised | 201 | 68.8% |
| c. Motorised | 28 | 9.6% |
| 2. | Illiterates | 223 | 76.4% |
| 3. | Smokers | 116 | 39.8% |
| 4. | Non smokers | 176 | 60.3% |
| 5. | Alcoholics | 256 | 87.7% |
| 6. | Non-alcoholics | 36 | 12.3% |
| 7. | Pan/Beetle chewing | 197 | 67.5% |
| 8. | Age in years |
| < 25 | 82 | 28.1% |
| 25-35 | 108 | 36.9% |
| 35-45 | 65 | 22.3% |
| > 45 | 37 | 12.6% |
Details of clinical findings and analysis of health seeking behaviour of fishermen.
| Clinical findings | No. of Cases (n=292) | Percentage (%) |
|---|
| Site of wound/injury |
| Upper extremity | 86 | 29.5% |
| Lower extremity | 89 | 30.5% |
| Head | 9 | 3.1% |
| Neck | 23 | 7.9% |
| Multiple sites | 36 | 12.3% |
| Other sites | 49 | 16.8% |
| Source of injury/wound |
| Fish hooks and forks | 62 | 21.2% |
| Spines | 15 | 5.1% |
| Metals/tools | 25 | 8.6% |
| Nets | 68 | 23.3% |
| Fish gear | 74 | 25.3% |
| Others | 48 | 16.4% |
| Type of injuries/wound |
| Major injuries | 27 | 9.2% |
| Minor injuries: |
| Cuts | 42 | 14.4% |
| Laceration | 203 | 69.5% |
| Blow with objects/tools/net | 94 | 32.2% |
| Puncture wounds | 65 | 22.3% |
| Contusion | 38 | 13.0% |
| Others | 12 | 44.1% |
| Vaccination after injury |
| Yes | 17 | 5.8% |
| No | 275 | 94.2% |
| First aid after injury |
| Yes | 23 | 7.9% |
| No | 269 | 92.1% |
| Treatment after injury |
| Yes | 105 | 35.4% |
| No | 187 | 64.0% |
| Visit to hospital after injury |
| Yes | 38 | 13.0% |
| No | 254 | 87.0% |
Discussion
A total of 292 wound/pus samples collected from wound infection due to occupational injuries among fishermen population of Puducherry was the basis of this study. In the present study, nearly 55.5% of the wound samples collected from fishermen showed growth with the majority of the isolates were organisms causing secondary bacterial infection. Interestingly in this study, 16.1% showed polymicrobial growth, indicating broad spectrum antibiotics are required to treat water-related infections. Polymicrobial soft tissue infections often need surgical debridement and treatment with the combination of antimicrobials [18,20]. Moreover, water related wound infection requires prolonged antibiotic treatment for more than 3-12 months [9]. Wound/injury among fishermen often progresses to variable severity resulting in cellulitis, ulcers, necrotising vasculitis, myositis and septicemia [21] moreover the severity of the disease also increases if there is any systemic illness [3,7]. Sepsis due to cellulitis is common among fishermen [11]. Hence, wound infection in fishermen is of major concern, requires early detection and management to prevent complications such as sepsis.
In the present study, it was found that bacteria causing secondary infection such as Staphylococcus aureus, CONS, Streptococcus pyogens, Gram-negative bacilli such as Pseudomonas spp., E. coli, Klebsiella pneumoniae, Enterobacter spp. and Proteus spp. were isolated from wound samples collected from fishermen. A similar study has shown wound infection exposed to salt water had growth of aquatic pathogen such as Staphylococcus, Pseudomonas, Vibrio and Streptococcus [8,9,22]. Majority of the isolates (53.1%) was Staphylococcus aureus, this could be due to prolonged exposure of wound to saltwater. The antimicrobial-resistance pattern varies in each population and community. It’s quite alarming that the overall percentage of drug resistance strain isolated in the study was higher. A 61.0% MRSA, 60.9% ESBL Pseudomonas spp, 55% ESBL E.coli, 33.3% ESBL Klebsiella pneumoniae, 33.3% VRE and 32.3% Methicillin-resistant CONS were isolated from the wound infections of the fishermen in this community. The results of the present study is in concordance with an earlier study in which it was proved due to resistance developed against most of the antibiotics available, bio active compounds are essential for the treatment against MRSA strains isolated from wound infection of fishermen [18]. A total of 8.7% MBL producing Pseudomonas spp. and 5% MDR E.coli was also isolated in this study. Moreover the 61.0% MRSA and 32.3% Methicillin-resistant CONS isolated in this study could also contribute to community-acquired Methicillin-resistant Staphylococcus spp. The increased drug resistance strains reported in this community with more of their negligence towards a visit to the hospital and their poor access to health care facilities is an issue to be monitored.
Globally there is a degradation of the coastal community, despite fishing being hazardous and stressful of all occupations [23]. Most fishermen living in the coastal areas of Puducherry had low socioeconomic status and were of the traditional type still following older methods of fishing [11,13]. A 68.8% of fishermen in this study were found to use non-mechanised fishing crafts. Catamaran and canoes were used by majority of the fishermen as fishing vehicles. Work related injuries have been reported high among fishermen [23,24]. In the present study, 9.2% of fishermen suffered from major injuries and majority 69.5% had lacerations. European safety commission had also reported work-related injuries are more in fishermen population than in manufacturing factories and the rate of injury to be high in this community [25]. Another study has also reported fishermen faced fatal injuries and are at high risk for accidents [24,26]. Studies on fishermen showed that they suffered from injuries, fractures, dislocations and contusions relating it to their vulnerable lifestyle and strenuous work [2,26-28]. In the majority of the study population injuries were confined to the extremities. Most common injuries were reported in the lower extremities 30.5% followed by 29.5% in the upper extremities. Studies have shown the high prevalence of ulceration, fissures, sores and erosion mostly in the limbs region of fishermen [29] and the injuries were more concentrated in the arms [24,30]. Similar results were observed among Indian rural fishing community of Karnataka [31]. The present study also found that fishery workers in this community were largely injured due to fishing gear, nets and hooks which occurred mainly during hauling of fish gear and sorting the fishes. Hence, the findings of the present study suggest that fishermen in this community need to be trained in modern methods of fishing and introduce safety measures to reduce occupation-related injuries and minor problems.
Age wise distribution shows the majority of fishermen with wound injuries were in the age group 25 to 35 years and less than 25 years might be because they are actively involved in fishing and their frequent exposure to the aquatic environment [12,13]. Fishermen in this study were backwards and socially marginalised due to various reasons. About 76.6% of fishermen enrolled in the study were illiterates. Alcohol intake and pan chewing were found to be high among fishermen of this community compared to smoking. Similar results were observed among fishermen of Dharwad district, Karnataka [32] and Puducherry [13]. Despite fishing being a risky, traumatic and dangerous occupation with long hours of work under poor weather conditions. Furthermore, their personal habits, lifestyle, lack of healthcare facilities make their condition worse [2,15,27,33].
In addition, a total of 87.0% of fishermen in the present study ignored visit to the hospital after injury and reported self-medication. About 94.2% of fishermen had not taken any vaccination after injury. Fishermen were unable to access the medical services available mainly due to their long hours of strenuous work [34]. Poor or delayed utilisation of health facilities, lack of education, underlying systemic illness, low standards of personal hygiene and habits are the pivotal reasons for high proportion of wound sepsis and cellulitis associated sepsis among fishermen [2]. Hence, the present study highlights health education and first aid promotion to be very essential in this population. The findings of the study imply that fishery workers need to be educated on healthy lifestyle and its mandatory to include health surveillance camps and pre-employment checks for this population.
Limitation
In most of the patients from whom CONS were isolated had associated co-morbidities. The results of which were not presented in the present manuscript due to space constraint. The 13.3% of CONS isolated in the study also requires follow-up, which was not done due to financial and logistical reasons. More follow-up studies in such population are essential in order to prove any change in behaviour could impact infection rate and prognosis or not. Further detailed analyses/root causes analysis is needed to justify whether self-medication in this community has led to increased drug resistance.
Conclusion
Increased secondary bacterial wound infection was found among fishermen’s of Puducherry mainly because people living in the coastal environment are socially marginalised and have poor access to healthcare centres. The present study provides clues on most common marine bacterial flora that can cause wound infection and guide for empirical therapy. The percentage of drug resistance in this community was higher which is a major issue to be addressed. To conclude fishermen in this community require frequent health camps, knowledge on immunisation and drawbacks of self-medication, emphasis and training on first aid, exposure to healthcare facilities and education on complications related to late wound care. Furthermore, fishermen in this community need to be trained in modern methods of fishing in order to prevent occupation-related injuries.