Sinus of Valsalva Aneurysm Dissecting into Interventricular Septum Compressing RVOT
Nishu Raj1, Pallavi Sinha2, Neeraj Wadhva3, Sunil Kumar Puri4
1 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
2 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
3 Senior Resident, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
4 Head, Department of Radiodiagnosis, GB Pant Hospital, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Nishu Raj, 125 A/1, Savitri Nagar, New Delhi-110017, India.
E-mail: nishuraj2003@gmail.com
Aneurysm of sinus of valsalva is a rare disorder. Rupture of sinus of valsalva into the right atria, right ventricle and the left ventricle is more commonly seen. Dissection of sinus of valsalve into the interventricular septum is rare, moreover right ventricular outflow tract obstruction due to it is still rarer. We present a case of ruptured sinus of valsalva aneurysm into the interventricular septum causing right ventricular outflow tract obstruction presenting with heart block.
Interventricular septum dissection, Heart block, Rupture of sinus
Case Report
A 26-year-old man presented to the emergency department with history of syncope. Patient complained of chest discomfort, dyspnea on exertion, with his blood glucose levels within normal limits. His blood pressure was 130/84 mmHg and he had past history of dyspnoea on exertion and a stent placed in his left anterior descending artery. An ECG was obtained which showed complete heart block. CT revealed aneurysm in the right sinus of valsalva.
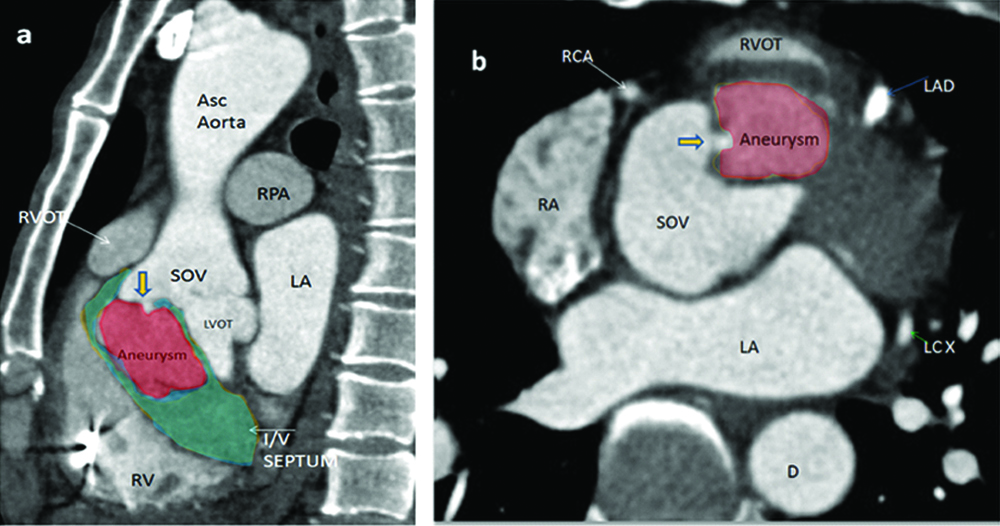
A large 34×45×40 mm contrast filled outpouching arising from the right sinus of valsalva, with a neck of 2 mm, directed posteroinferiorly and dissecting into the interventricular septum was seen [Table/Fig-1a]. It caused mass effect in the form of obstruction to the right ventricular outflow tract [Table/Fig-1b]. There was a stent in LAD otherwise coronary arteries were normal [Table/Fig-1c]. No E/O VSD, bicuspid aortic valve or aortic root dilatation was seen. Patient was kept for cathter angiography to plan for further surgical management but the patient left against medical advice.
Saggital image 1(a) and axial image 1(b) showing sinus of valsalva aneurysm (solid red colour) arising from right sinus. Yellow arrow shows neck of aneurysm. It can be seen dissecting into the interventricular septum (solid green colour) and compressing the Right Ventricular Outflow Tract (RVOT) causing its obstruction.
LA: Left atria; LAD: Left coronary artery; LCX: Left circumflex artery; RCA: Right coronary artery; RPA: Right pulmonary artery; RVOT: Right ventricular outflow tract; SOV: Sinus of valsalva
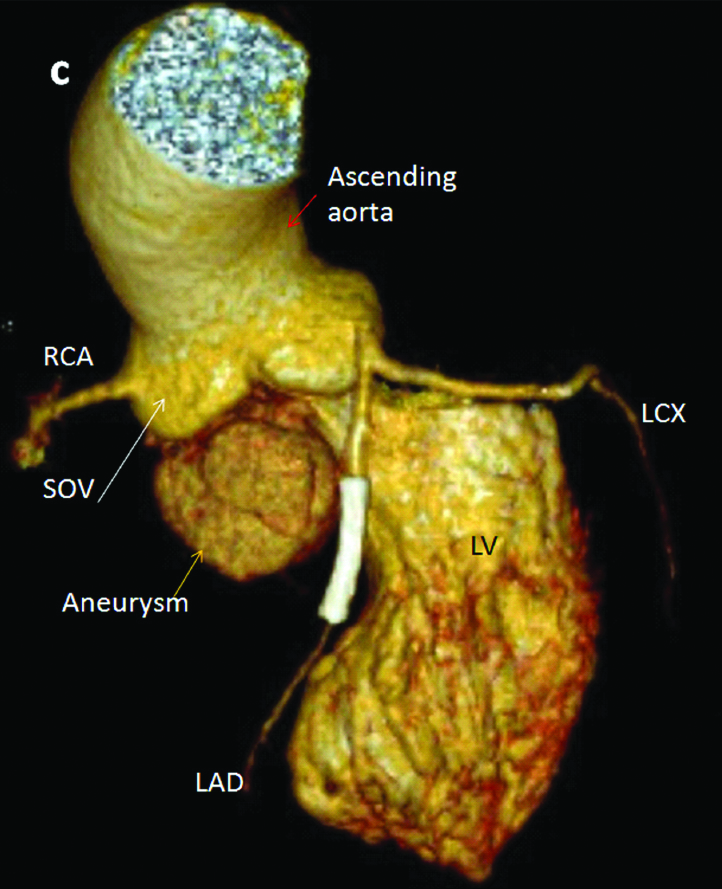
Volume rendered image showing sinus of valsalva aneurysm (aneurysm) arising from right Sinus of Valsalva (SOV).
LAD: Left anterior descending; LCX: Left circumflex artery; LV: Left ventricle; RCA: Right coronary artery
Discussion
Aneurysms of sinus of valsalva are a rare disorder with their incidence reported to be 0.15% in open heart surgery patients, with being more common in males as compared to females, ratio being 3:1 [1]. Common complication associated with sinus of valsalva is that they rupture into right ventricle or the right atrium [2]. The complication of dissection into the interventricular septum leading to the right ventricular outflow tract obstruction is still rarer. The dissection of sinus of valsalva into interventricular septum is reported to be less than 2% of sinus of valsalva ruptures [3].
Sinus of valsalva aneurysm occurs between the aortic annulus and the sinotubular ridge. They can be congenital or acquired. Congenital ones are reported to be associated with VSD, bicuspid aortic valve, coronary artery anomalies and aortic regurgitation. Acquired ones can be caused due to infective endocarditis, tuberculosis, syphilis and atherosclerosis. Dissection into the interventricular septum was first reported by Warthen RO in 1947 [4]. The most popular school of thought believes it to be due to discontinuity between the aortic tunica media and aortic valve annulus, which is congenital in origin [5]. It may present with various clinical symptoms. They are known to be formed above the aortic valve ring and can extend in any direction. Rarely, it is asymptomatic. Depending upon the size of aneurysm, the rapidity with which it ruptures, the cardiac chamber with which it communicates, the symptoms of ruptured aneurysm of valsalva may include severe dyspnea, chest pain, haemodynamic compromise, insidious heart failure with fatigue and volume overload [2]. Disrupted aortic root anatomy can cause kinking or compression of coronary ostia with resultant myocardial ischemia [6]. Rupture into pericardial space may lead to cardiac temponade. Sinus of valsalva aneurysm most commonly presents with rupture into one of the cardiac chambers. Sinus of valsalva aneurysm causing right ventricular outflow tract obstruction is very rare.
Some of the indications for surgical repair of non ruptured sinus of valsalva aneurysm include ventricular outflow tract obstruction, arrhythmia and interventricular dissection. However, in asymptomatic patients with small nonruptured aneurysm, surgical intervention is controversial and follow up is recommended. Large aneurysm may be repaired to avoid complications [2]. The mean duration of survival after diagnosis of a ruptured valsalva sinus aneurysm is 3.9 years [7]. The main stay of treatment for ruptured aneurysm is cardio pulmonary bypass surgery. The aneurysm is closed with a pericardial or polyester patch or with sutures [2].
Conclusion
A case of right sinus of valsalva aneurysm dissecting into interventricular septum and causing right ventricular outflow tract obstruction is a distinct entity, in respect to its presentation, diagnosis, complications and treatment. Early diagnosis with advanced imaging like three dimensional volume rendered images helped in better demonstration of the anatomy to the surgeons and help in preventing the unnecessary complications.
[1]. Takach TJ, Reul GJ, Duncan JM, Cooley DA, Livesay JJ, Ott DA, Sinus of Valsalva aneurysm or fistula: management and outcomeAnn Thorac Surg 1999 68(5):1573-77.10.1016/S0003-4975(99)01045-0 [Google Scholar] [CrossRef]
[2]. Bricker AO, Avutu B, Mohammed T-LH, Williamson EE, Syed IS, Julsrud PR, Valsalva sinus aneurysms: findings at CT and MR ImagingRadioGraphics 2010 30(1):99-110.10.1148/rg.30109571920083588 [Google Scholar] [CrossRef] [PubMed]
[3]. Lee DH, Kang E-J, Park T-H, Woo JS, Hong SH, Kim Y-D, A case of right sinus of valsalva rupture with dissection into interventricular septum causing left ventricular outflow tract obstructionKorean Circ J 2013 43(11):77010.4070/kcj.2013.43.11.77024363754 [Google Scholar] [CrossRef] [PubMed]
[4]. Warthen RO, Congenital aneurysm of the right anterior sinus of Valsalva (interventricular aneurysm) with spontaneous rupture into the left ventricleAm Heart J 1949 37(6):975-81.10.1016/S0002-8703(49)90947-3 [Google Scholar] [CrossRef]
[5]. Edwards JE, Burchell HB, The pathological anatomy of deficiencies between the aortic root and the heart, including aortic sinus aneurysmsThorax 1957 12(2):125-39.10.1136/thx.12.2.12513442955 [Google Scholar] [CrossRef] [PubMed]
[6]. Lijoi A, Parodi E, Passerone GC, Scarano F, Caruso D, Iannetti MV, Unruptured aneurysm of the left sinus of valsalva causing coronary insufficiency: case report and review of the literatureTex Heart Inst J 2002 29(1):40-44. [Google Scholar]
[7]. Ring WS, Congenital Heart Surgery Nomenclature and Database Project: aortic aneurysm, sinus of valsalva aneurysm, and aortic dissectionAnn Thorac Surg 2000 69(3):147-63.10.1016/S0003-4975(99)01242-4 [Google Scholar] [CrossRef]