Haemangioma of Cervix - A Case Report
Manan B Shah1, Kalyani Raju2
1 Resident, Department of Pathology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
2 Professor, Department of Pathology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kalyani Raju, Professor, Department of Pathology, Sri devaraj Urs Medical College, Sri Devaraj Urs Academy of Higher Education, Kolar-563101 Karnataka India.
E-mail: drkalyanir@rediffmail.com
Haemangiomas are very common benign vascular lesions. However, haemangioma of cervix is very rare. They are more common in 2nd and 3rd decades of life. Most of them are asymptomatic and discovered incidentally. Surgical excision remains the treatment of choice in most of the cases and alternatively conservative treatment can also be considered which is helpful in preserving fertility in the young females. We present a case of cervical haemangioma in a 38-year-old female which was diagnosed incidentally.
Cervical haemangioma, Surgical excision, Vascular lession
Case Report
A 38-year-old female, G2P2L2, presented with pain in abdomen and dyspareunia since 6 months. Her menstrual cycle had been regular and of normal flow and duration. No history of vaginal infection. Per speculum examination shows reddish blue discoloration of cervix and it bleeds on touch. No history of intake of oral contraceptive pills. No significant past obstetric history. Ultrasonography (USG) showed bulky uterus and adenomyosis in posterior wall of uterus. Patient underwent total abdominal hysterectomy.
Gross examination of specimen showed uterus and cervix measuring 10x9x4 centimeters. External surface of the uterus was unremarkable. Cut section showed trabeculations of myometrium. External surface of cervix was unremarkable, cut section showed bluish discoloration involving stroma of whole of the cervix [Table/Fig-1]. On microscopy section studied from cervix showed multiple thin walled vascular channels of varying size in cervical stroma having erythrocytes within the lumen, suggestive of capillary and cavernous type. These features were consistent with vascular haemangioma (Mixed type) [Table/Fig-2]. Section studied from myometrium showed features of adenomyosis. Patient had no postoperative complication. Patient was lost for follow-up.
Gross photograph of cut section of Uterus and cervix, uterus shows trabaculations and cervix showing bluish discoloration.

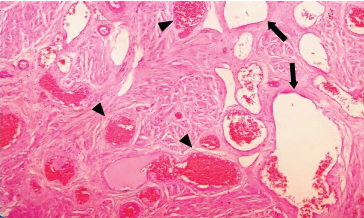
Microphotograph of cervical haemangioma showing vascular channel of both cavernous and capillary type (H&E X100). Arrow showing Large cystically dilated vessels with thin walls containing RBCs and Arrow head shows thrombosed blood vessels.
Discussion
Haemangiomas/vascular hamartoma are very common benign vascular lesion. Among these, capillary haemangiomas are the most common type. It commonly occurs in the skin, subcutaneous tissue and oral cavity as well as liver, spleen and kidneys. However haemangioma of cervix is very rare and about 55 cases are reported in literature till date [1,2]. One of the very first reports of the haemangioma cervix was described by weed in 1948 [3]. Though they are commonly congenital in origin, they can be developmental with potential to proliferate [4]. They are more common in 2nd and 3rd decades of life and parity has no significant role [5]. In the present case of cervical haemangioma, the age of the patient was 38 years.
Due to their small size, most of them are asymptomatic and discovered incidentally [3]. Only one third of the cases are symptomatic [6]. Patient may present with menorrhagia, inter-menstrual spotting, post-coital bleeding, infertility, dyspareunia and also associated with use of oral contraceptive pills [7,8]. It can also mimic endometriosis [9]. The obstetrical complications are the premature rupture of membranes, the intra-uterine fetal death, post partum haemorrhage and disseminated intravascular coagulation. Rare cases of coexistence of cervical haemangioma with pregnancy are also reported. Association with oral contraceptive pills and pregnancy indicates role of hormone in development of cervical haemangiomas [10]. Due to variation in hormonal levels in pregnancy, it may aggravate the symptoms of existing haemangiomas. It is shown that oestrogen has an important role in the development of haemangioma, by presence of oestrogen receptor in endothelial cells of haemangioma [1,11]. Riggs J et al., reported one case of haemangioma of cervix with intractable bleeding even after termination of pregnancy despite curettage and suturing, ultimately hysterectomy was done [12]. Padmanabhan V et al., reported one case of cervical haemangioma along with focal nodular hyperplasia of liver in a 34-year-old women with history of intake of oral contraceptive pills [13]. Djolai M et al., reported a case of cervical haemangioma associated with dysplasias in endocervical epithelium [6]. In the present case patient presented with dyspareunia. No history of use of oral contraceptive pills was noted. Grossly haemangioma can be described as port wine or brownish discoloration. They are small and well circumscribed or diffuse and sometimes may also involve vagina and vulva [14]. Haemangiomas should be differentiated from microvascular proliferations due to chronic infections because similar clinical presentation can be seen in case of chronic cervicitis [10]. In present case the cervical haemangioma showed diffuse brownish discoloration involving both lips of cervix.
The cervical cavernous haemangioma can be associated with generalized vascular malformations such as Blue rubber bleb nevus syndrome, which is a rare disease showing venous malformations of the skin, gastro-intestinal tract and other internal organs. Tanaka N et al., reported a case who presented with the blue rubber bleb nevus syndrome disease with multiple haemangiomas on the uterine cervix during pregnancy [15]. The present case was not associated with any syndrome.
Surgical excision remains the treatment of choice in most of the cases and alternatively conservative treatment can also be considered, such as cryotherapy, LEEP, Sclerosing agents and carbon dioxide laser in preserving fertility in the young females. Though, normal delivery is possible, caesarean is recommended many times [11]. Now, hysterectomy has been limited to cases in which conservative management or surgical excision has failed [16]. Transcatheter arterial embolisation can also be considered after delivery in rapidly growing vaginal haemangioma. Spontaneous regression of haemangioma is reported [17]. In the present case hysterectomy was done for adenomyosis of uterus and cervical haemangioma was diagnosed incidentally.
Conclusion
Cervix is a rare site for the occurrence of haemangioma. Clinical manifestation is varied. It can be an incidental finding as in the present case which was quite asymptomatic or can present with frank gynaecological as well as obstetrical complications. The final diagnosis can only be made by the Histopathological examination.
[1]. Busca A, Parra-Herran C, Hemangiomas of the uterine cervix: Association with abnormal bleeding and pain in young women and hormone receptor expression. Report of four cases and review of the literaturePathol Res Pract 2016 212(6):532-38.10.1016/j.prp.2016.03.00327067810 [Google Scholar] [CrossRef] [PubMed]
[2]. Bharti P, Shah SN, Cavernous haemangioma of cervix--a case reportJ Indian Med Assoc 2012 110(4):258 [Google Scholar]
[3]. Douglas JM, Hemangioma of the cervixObstet Gynaecol 1961 17(2):191-93. [Google Scholar]
[4]. Shann SM, Dunham RJC, Wilson JD, Hemangioma of the uterine cervixInternational Journal of STD and AIDS 2004 15:486-88.10.1258/095646204121113515228736 [Google Scholar] [CrossRef] [PubMed]
[5]. Kondi-Pafiti A, Kairi-Vassilatou E, Spanidou-Carvouni H, Kontogianni K, Dimopoulou K, Goula K, Vascular tumours of the female genital tract: a clinicopathological study of nine casesEur J Gynaecol Oncol 2003 24(1):48-50. [Google Scholar]
[6]. Djolai M, Bošković T, Djurdjević S, Dajko ST, Visnjić BA, Rajović R, Hemangioma of uterine cervix associated with high-grade squamous intraepithelial lesionVojnosanit Pregl 2015 72(6):541-44.10.2298/VSP1506541D26226728 [Google Scholar] [CrossRef] [PubMed]
[7]. Gada RP, Simmons PS, Wilson TO, Coddington CC, A hemangioma of the cervix in childhood can be a harbinger of menorrhagia and infertility as an adultJ Pediatr Adolesc Gynaecol 2014 27(6):139-41.10.1016/j.jpag.2014.02.00325085019 [Google Scholar] [CrossRef] [PubMed]
[8]. Dahiya N, Dahiya P, Kalra R, Marwah N, Jain S, Cavernous hemangioma of uterine cervix – a rare cause of postcoital bleedingIjpsr 2011 2(5):1209-11. [Google Scholar]
[9]. Jaouad K, Youssef B, Hanane R, Driss M, Mohammed D, Haemangioma of the Cervix Micking Cervical Endometriosis: A Case ReportJournal of Gynaecology and Obstetrics 2015 3(3):66-68.10.11648/j.jgo.20150303.15 [Google Scholar] [CrossRef]
[10]. Ahern JK, Allen NH, Cervical hemangioma: A case report and review of literatureJ Reprod Med 1978 21(4):228-31. [Google Scholar]
[11]. Bonetti RL, Boselli F, Lupi M, Bettelli S, Schirosi L, Bigiani N, Expression of oestrogen receptor in haemangioma of the uterine cervix: Reports of three cases and review of the literatureArchives of Gynaecology and Obstetrics 2009 280(30):469-72.10.1007/s00404-009-0928-019148658 [Google Scholar] [CrossRef] [PubMed]
[12]. Riggs J, Bertoni M, Schiavello H, Weinstein A, Kazimir M, Cavernous hemangioma of the cervix with intractable bleeding. A case reportJ Reprod Med 2003 48(9):741-43. [Google Scholar]
[13]. Padmanabhan V, Mount SL, Eltabbakh GH, Cavernous hemangioma of the cervix in association with focal nodular hyperplasia of the liver. A case reportJ Reprod Med 2001 46(12):1067-70. [Google Scholar]
[14]. Cherkis RC, Kamath CP, Haemangioma of the uterine cervix and pregnancy: a case reportJ Reprod Med 1988 33:393-95. [Google Scholar]
[15]. Tanaka N, Tsuda M, Samura O, Miyoshi H, Hara T, Kudo Y, Blue rubber bleb nevus syndrome: Report of a patient with haemangiomas of the vaginal portion of the cervix appearing during pregnancyJournal of Obstetrics and Gynaecology Research 2007 33:546-48.10.1111/j.1447-0756.2007.00568.x17688627 [Google Scholar] [CrossRef] [PubMed]
[16]. Powell JL, Zwirek SJ, Sankey HZ, Hemangioma of the cervix managed with the Nd: YAG laserObstet Gynaecol 1991 78(5):962-64. [Google Scholar]
[17]. Emoto M, Tamura R, Izumi H, Sukimoto S, Kawarabayashi T, Shirakawa K, Sonodynamic changes after transcatheter arterial embolization in a vaginal haemangioma: case reportUltrasound Obstet Gynaecol 1997 10:66-67.10.1046/j.1469-0705.1997.10010066.x9263427 [Google Scholar] [CrossRef] [PubMed]