Is Serum Lactic Acid a Reliable Indicator for Diagnosing Fat Embolism Syndrome?
Chandra Sekhar Bhumireddy1, Surendra Umesh Kamath2, Sunil Lakshmipura Krishnamurthy3
1 Postgraduate, Department of Orthopaedics, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
2 Professor and Head, Department of Orthopaedics, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
3 Senior Resident, Department of Orthopaedics, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Surendra Umesh Kamath, Professor and Head, Department of Orthopaedics, Kasturba Medical College Hospital, Attavar, Mangalore-575001, Karnataka, India.
E-mail: skamath3@hotmail.com
Introduction
The incidence of Fat Embolism Syndrome (FES) has been reported to occur in 0.5 to 3% of patients with isolated long bone fracture. FES is most commonly associated with long bone fractures, if associated with polytrauma then the chance of manifestation increases by 11%. Fat embolism is a clinical entity diagnosed mainly by Gurd’s criteria which includes clinical signs and blood parameters. There is no single blood parameter to detect FES at earliest. A high lactate level is an early sign of tissue hypoxia. In patients with femur shaft fracture tissue hypoxia is the most important cause of increased lactate levels. Increased blood lactate level is related to increased mortality.
Aim
To establish the relationship between serum lactic acid and fat embolism in patients with fracture shaft of the femur.
Materials and Methods
The present was a prospective study done at Kasturba Medical College Hospitals, Mangalore, Karnataka, India, on 40 patients with femur shaft fracture. Statistical analysis was done using SPSS (version 17.0).
Results
In the present study, four patients out of 40 had FES (Gurd’s criteria), whose serum lactic acid was high (>25) within 72 hours of injury. Fourteen patients had elevated lactic acid (>20) but did not develop FES. All patients with FES had elevated serum lactic acid which was statistically significant (p-value 0.003), yet serum lactic acid estimation was less sensitive 28.7%.
Conclusion
In conclusion serum lactic acid is specific (100%) for fat embolism but not sensitive (28.7%). By using serum lactic acid level, development of fat embolism can’t be predicted however, elevated lactic acid level will help us in risk stratification.
Acidosis, Gurd’s criteria, Hypoxia, Long bone shaft fracture
Introduction
Fat Embolism Syndrome (FES) is a constellation of neurological, pulmonary, dermatological and haematological symptoms [1]. In 1873, Bergmann described the first clinical case of fat embolism in a patient with a distal femur fracture [2]. The incidence of FES has been reported to occur in 0.5 to 3% of patients with isolated long bone fracture [3]. FES is most commonly associated with long bone fractures, if associated with polytrauma then the chance of manifestation increases by 11% [3].
With increased incidence of high-velocity accidents, there are increasing trends towards polytrauma conditions involving more than one fracture and more than one system involvement [4]. These patients are at high risk of developing FES. Fat embolism is also seen in patients with pelvic fractures but the mortality in pelvic fractures is mainly due to hypovolemic shock [4]. In FES respiratory system is most commonly involved followed by neurological manifestations [1].
The patho-physiology of these condition mechanisms has been based on both, biochemical and mechanical theories. The first theory propagates a hormonal or an enzymatic (lipoprotein lipase) background and second the mechanical theory hypothesises that a mechanical block of the pulmonary vasculature by embolised fat globules is the culprit. [5].
Mortality rate following FES has been reported to be as high as 20%, hence early diagnosis and management of this condition is important [4]. The study shows respiratory distress is the frequent cause of mortality in patients of fat embolism [1].
Fat embolism is a clinical entity diagnosed mainly by Gurd’s criteria which includes clinical signs and blood parameters [2]. There is no single blood parameter to detect FES at earliest [5].
Gurd described fat embolism as a triad of hypoxia, petechiae and confusion [2]. Gurd has described major and minor criteria. A diagnosis of FES can be made, if two major criteria and two minor criteria are present. Schonfeld proposed the fat embolism index to aid in diagnosing FES as a cumulative score of five or more over the first three days of hospitalisation [5,6]. Gurd’s criteria most commonly are used for diagnosing FES because it is simple and easily accessible and detect FES early.
A high lactate level is an early sign of tissue hypoxia [7]. In femur shaft fracture patient’s tissue hypoxia is the most important cause of increased lactate levels [5]. Increased blood lactate levels are related to increased mortality [7-9]. Serum lactic acid level estimation is easy, and inexpensive. It may be helpful in the early diagnosis as well as may predict the severity and outcome. Hence, authors conducted the present study. The present prospective study aimed to establish the relationship between serum lactic acid and fat embolism in patients with fracture shaft of the femur.
Materials and Methods
After obtaining Institutional Ethics Committee clearance (IEC KMC MLR12-15/291), a prospective study was carried out, from January 2016 to August 2017. The present study was performed on 40 patients, between 20-40 years of both sexes presented to the emergency orthopaedic services following an injury within 12 hours and known to have isolated femur shaft fracture were included. The convenient sampling method was used. Patients with age more than 40 years, any pathological fracture of femur shaft and with head injury, chest injury were excluded.
All the patients were managed as per Advanced Trauma Life Support protocol. Relevant history of all details regarding the nature of the accident, any prior treatment other extra-skeletal injuries, and pre-existing comorbid illnesses were obtained.
After initial resuscitation and splinting, appropriate imaging for the skeletal injuries was done. Clinical parameters such as pulse rate, respiratory rate, temperature, blood pressure, urine output were recorded at the admission and four hourly. Routine investigations at admission included haematological biochemical and arterial blood gas results and serum lactic acid.
The following parameters related to FES were recorded regularly for 72 hours following admission:
four hourly records of temperature, pulse rate, blood pressure, respiratory rate, and urine output;
Fundus and urine examination for fat globules;
Posterior-anterior radiograph of the chest;
Arterial blood gas analysis;
Blood investigations included haemoglobin, packed cell volume, total and differential counts and serum lactate levels.
The diagnosis of FES was made using the Gurd’s criteria. Serum lactate estimation was done by the oxidase and peroxidase method. The clinical and laboratory parameter, serum lactate levels obtained at admission were analysed. Patients were observed subsequently for features of FES.
Statistical Analysis
Statistical analysis was done using sensitivity, specificity, positive and negative predictive value for lab value and Mann-Whitney test z-values using SPSS version 17.0. Mann-Whitney test is a non-parametric test and z-value in the present study was calculated for association of serum lactic acid levels in fat embolism. A p-value of 0.003 was considered to be significant.
Results
The study included 40 patients with the mean age of 28 years, of which 33% were between 31 to 35 years, 32% were between 26 to 30 years, 22% were between 20 to 25 years and remaining 13% were between 36 to 40 years 6 out of 40 were females [Table/Fig-1].
Patients with femur shaft fracture.
| Age group distribution | 20-25 years | 26-30 years | 31-35 years | 36-40 years |
|---|
| Number of patients | 9 | 13 | 13 | 5 |
| Number of females | 1 | 3 | 2 | - |
| Number of fat embolism patients | - | 3 | 1 | - |
| Number of patients who had elevated serun lactic acid level but no fat embolism syndrome | 1 | 4 (1 Female) | 3 | 2 |
Four patients (10%) developed FES and had elevated serum lactic acid level (mean of 30 mg/dL) which is statistically significant with a p-value (0.003). Ten patients had elevated serum lactic acid level (mean of 24 mg/dL) with no features of FES. The normal range of serum lactic acid is <20 mg/dL. Mann-Whitney z-value of lactic acid for fat embolism in the present study was found to be 2.966.
All four patients with fat embolism had hypoxia and chest x-ray showed features of pulmonary oedema, three patients had tachycardia, three patients had neurological manifestation and depression. Petechiae were not present in any patient [Table/Fig-2].
Clinical manifestations of patients with FES.
| Patients developed fat embolism | Hypoxia | Neurologic manifestation | Tachycardia | Petechia |
|---|
| Patient 1 | + | + | - | - |
| Patient 2 | + | + | + | - |
| Patient 3 | + | - | + | - |
| Patient 4 | + | + | + | - |
Pyrexia was present in all four patients with FES. One patient had a sudden drop in platelets. No one had emboli in the retina in fundus examination and urine for fat globuli was negative in all four patients with fat embolism.
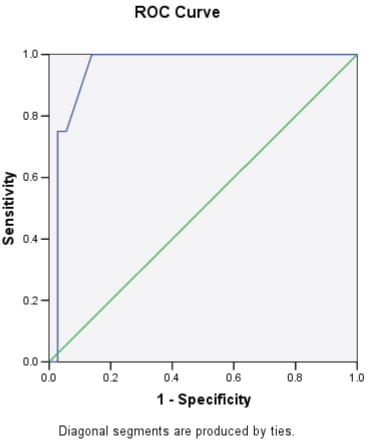
In the present study, 29% had fat embolism with elevated serum lactic acid mean (30) but 71% had elevated serum lactic acid mean (25) without fat embolism, i.e., 14 patients had elevated serum lactic acid level and four developed FES. Serum lactic acid has 100% specificity but it has only 28.57% sensitivity to detect fat embolism. ROC curve shows if serum lactic acid was more than 25 mg/dL sensitivity will increase to 75% from 28% [Table/Fig-3a,b].
Coordinates of the Curve.
| Positive if Greater Than or Equal To (a) | Sensitivity | 1-Specificity |
|---|
| 7.00 | 1.000 | 1.000 |
| 8.50 | 1.000 | 0.944 |
| 9.50 | 1.000 | 0.917 |
| 10.50 | 1.000 | 0.806 |
| 11.50 | 1.000 | 0.778 |
| 12.50 | 1.000 | 0.639 |
| 13.50 | 1.000 | 0.611 |
| 15.00 | 1.000 | 0.500 |
| 17.00 | 1.000 | 0.333 |
| 19.50 | 1.000 | 0.278 |
| 21.50 | 1.000 | 0.250 |
| 23.00 | 1.000 | 0.222 |
| 25.00 | 1.000 | 0.139 |
| 27.00 | 0.750 | 0.056 |
| 28.50 | 0.750 | 0.028 |
| 29.50 | 0.500 | 0.028 |
| 33.00 | 0.250 | 0.028 |
| 37.00 | 0.000 | 0.028 |
| 39.00 | 0.000 | 0.000 |
Test Result Variable(s): Serum lactic acid level in mg/dl
Coordinates of the Curve.
Discussion
The femur shaft fracture not only initiates the influx of marrow fat into the systemic and pulmonary vasculature, but also induce a systemic inflammatory response that produces cytokines capable of causing pulmonary damage [5,7]. The number of clinically evident cases of respiratory distress in such a scenario only represents the tip of the iceberg, with a large number of lung injury remaining clinically in apparent [8,10,11].
The present study was designed to measure the reliability and rapid accessibility of clinical or laboratory parameters that may help us in emergency management of femur shaft fracture patients. On assessment, in 40 patients, the correlation of clinical and radiological parameters observed at admission and the development of FES within 72 hours. All patients were tested for serum lactic acid level initial 72 hours. Serum lactic acid was repeated in all FES positive.
In the present study, four patients had FES as per Gurd’s criteria, in that one patient underwent intubation and recovered after 15 days. Remaining three patients were treated with oxygen supplementation and supportive care was given. By using these data serum lactic acid sensitivity and specificity calculated to predict fat embolism early. In the present study FES was observed in 10% of the patients with isolated femur shaft fracture and all patients who developed FES had at least one episode of drop in saturation (hypoxia) within 72 hours of the trauma. In the present study no mortality was observed after FES.
A study done by Gopinathan NR et al., points the importance of serum lactic estimation (within 12 hours) of injury and continuous Sa02 monitoring for 72 hours. Their study showed serum lactic acid was 88% specific in predicting FES [5]. Study done by Lamichhane P et al., showed, elevated blood lactate is a reliable marker in predicting survival, as longer the duration of elevated blood lactate the more chance of developing Multi Organ Dysfunction Syndrome (MODS) and complications [9]. Similarly, Javali RH et al., have stressed the importance of serum lactate estimation in predicting 24-hour mortality, blood transfusion requirement and intensive care admission [12].
Limitation
The study has few limitations including small sample size and lack of continuous pulse oximeter monitoring for early detection of hypoxia. Power of the present study was 80%.
Conclusion
Patients with the serum lactic acid level above 25 mg/dL should be kept on close watch as they are at the risk of developing FES. Hence, estimation of serum lactic acid level helps in prognosticating and triaging rather than diagnosing FES.
Test Result Variable(s): Serum lactic acid level in mg/dl
[1]. Talbot M, Schemitsch EH, Fat embolism syndrome: history, definition, epidemiologyInjury 2006 37(4):03-07.10.1016/j.injury.2006.08.03516990059 [Google Scholar] [CrossRef] [PubMed]
[2]. Rodriguez-Gutiérrez R, Rodarte-Shade M, González-González JG, Lavalle-González FJ, Bergman’s Triad: fat embolism syndromeAm J Med Sci 2015 349(2):18610.1097/MAJ.0b013e3182a19e4824172235 [Google Scholar] [CrossRef] [PubMed]
[3]. Akoh CC, Schick C, Otero J, Karam M, Fat embolism syndrome after femur fracture fixation: a case reportIowa Orthop J [Internet] 2014 34:55-62. [Google Scholar]
[4]. Taviloglu K, Yanar H, Fat embolism syndromeSurg Today 2007 37(1):05-08.10.1007/s00595-006-3307-517186337 [Google Scholar] [CrossRef] [PubMed]
[5]. Gopinathan NR, Sen RK, Viswanathan VK, Aggarwal A, Mallikarjun HC, Manoharan SRR, Early, reliable, utilitarian predictive factors for fat embolism syndrome in polytrauma patientsIndian J Crit Care Med 2013 17(1):38-42.10.4103/0972-5229.11215523833475 [Google Scholar] [CrossRef] [PubMed]
[6]. Karagiorga G, Biochemical parameters of bronchoalveolar lavage fluid in fat embolismIntensive Care Med 2006 32(1):116-23.10.1007/s00134-005-2868-x16322975 [Google Scholar] [CrossRef] [PubMed]
[7]. Bakker J, Schieveld SJ, Brinkert W, Serum lactate level as a indicator of tissue hypoxia in severely ill patientsAfdeling Intensive Care 2000 144(16):737-41. [Google Scholar]
[8]. Ahmed N, Fouldien A, Fourie C, Hardcastle T, Early onset fat embolism syndrome: Case report and literature reviewInjury Extra 2008 39(9):305-08.10.1016/j.injury.2008.03.013 [Google Scholar] [CrossRef]
[9]. Lamichhane P, Shrestha S, Banskota B, Banskota AK, Serum Lactate -An indicator of morbidity and mortality in polytrauma and multi-trauma patientsNepal Orthopaedic Association Journal 2011 2(1):07-13.10.3126/noaj.v2i1.8134 [Google Scholar] [CrossRef]
[10]. Blokhuis TJ, Pape HC, Frölke JP, Timing of definitive fixation of major long bone fractures: Can fat embolism syndrome be prevented?Injury 2017 48:S3-6.10.1016/j.injury.2017.04.01528449860 [Google Scholar] [CrossRef] [PubMed]
[11]. Huang BK, Monu JUV, Wandtke J, Pulmonary fat embolism after pelvic and long bone fractures in a trauma patientEmerg Radiol 2009 16(5):407-09.10.1007/s10140-008-0757-718696131 [Google Scholar] [CrossRef] [PubMed]
[12]. Javali RH, Prithvishree R, Patil A, Srinivasarangan M, Mundada H, Adarsh SB, A clinical study on the initial assessment of arterial lactate and base deficit as predictors of outcome in trauma patientsIJCCM 2017 21(11):719-25.10.4103/ijccm.IJCCM_218_1729279631 [Google Scholar] [CrossRef] [PubMed]