Substance abuse, the physically hazardous uses of various psychoactive drugs results in significant modification of brain structure and functional activity related to motor functions [1]. Recent studies show a significant rise in substance users in Nepal, which is eventually leading to severe healthcare burden [2]. Psychomotor functions are tasks that essentially give prominence to timing, accuracy, coordination, steadiness, and strength with less or negligible cognitive demands [3,4]. Further, the deleterious effect of motor functions is more significant than cognitive impairments in substance abuse [5]. Relapse of recovering substance abuser is predicated on motor functions obtained at the end of treatment [6]. Numerous data has revealed that lack of inhibitory control [7] and higher trait impulsivity [8], contributes to the progress and relapse of the disorder. Further, a recent study reported a significant dearth of neural motor inhibition, which correlates with altered inhibitory control in substance abusers, which in turn emphasised the motor function as a new biomarker [9]. Hence, it is essential to take into account the motor functions of substance abusers in the proposed treatment.
Yoga, a system of ethical, psychological, and physical practices, has shown encouraging results in the management of addictive behaviours [10]. Further, studies showed a lower risk of relapse to substance use [11], symptomatic improvements in psychiatric disorders [12], and psychophysiological effects following yoga-based intervention [13]. Furthermore, previous findings have shown augmentation of motor functions following yoga and physical exercise-based intervention [14-17].
Materials and Methods
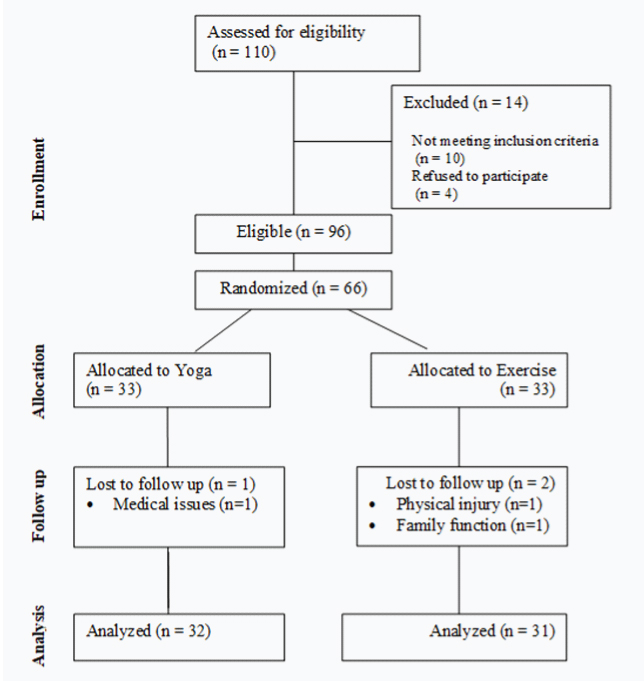
This randomised, open-label active control study, recruited a random subset of newly admitted substance abusers (n=66) from an in-house rehabilitation care unit at Kathmandu Valley, Nepal. A priori computation of sample size using G* Power come out 54 participants, with an effect size 1.016 [19] at an alpha value of 0.05 and with the actual power of 0.95. The research study was carried out between August 2016 to March 2017. Participants were 18–40 years of age, met the DSM-V criteria [20] for substance use disorder, stability in psychological symptoms, and three weeks of sobriety or abstinence in which they underwent medically supervised detoxification. Individuals who had a legal case that interfered during the study period were excluded. Further, patients with the acute major psychiatric disorder and active infectious diseases (HIV and tuberculosis) were not included.
Baseline Assessment
The study was reviewed and received ethical approval (631-02/10/16) from the Nepal Health Research Council Kathmandu, Nepal. Each participant was fully informed about the study protocol and provided written consent to participate. After collecting baseline data on demographic profile, years of substance abuse, type of drug addiction, fine motor speed, dexterity, and arm-hand steadiness, the participants were randomly assigned to yoga intervention (n=33) or physical exercise (n=33) for twelve weeks, in addition to treatment as usual based on simple random allocation generated using computer software (a free on-line Randomizer) [21].
Intervention
Details of the yoga and physical exercise intervention have been published previously [18]. The intervention was administrated weekly six sessions of 90 minutes duration over 12 weeks in the morning 6.30-8.00 am under the supervision of a trained yoga therapist and physical instructor. The yoga protocol consisted of loosening practices, kapalabhati kriya and sun salutation. Further, asanas (standing, sitting, supine, & prone posture), breathing techniques, pranayama (bhastrika, bhramari, nadhisuddhi, & cooling) and meditation (Om meditation & cyclic meditation). Between the practices, different relaxation techniques such as Instant Relaxation Techniques, Quick Relaxation Techniques, and Deep Relaxation Techniques were administered. The physical exercise program includes loosening, warm-up, stretching to enhance flexibility and strengthening exercise. Further, moderate aerobics which included different types of walking (drill and brisk) and various forms of jogging (forward, backward, and side).
Assessments
Finger Tapping Test
The finger-tapping test provides an easily quantifiable measure of fine motor speed. Subjects were seated in optimal comfort position with forearms laid on a table in front of them. Participants were instructed to rest their hand on wooden board raised on one side and place the index finger on a small lever connected to a mechanical counter. When the lever was pressed down all the way and released, the counter increased the reading by one. Further, participants were tutored to oscillate the index finger as quickly instead of the wrist. After explaining the procedure, a brief practice session was given before the actual recording. Readings of taps at the interval of 10, 20 seconds, and final reading in 30 seconds were noted. Higher the scores better the fine motor skill [22].
Tweezer Dexterity Test
Subjects sat comfortably in front of a table on which the dexterity board was placed. The board consists of two halves. One half has a square plate approximately 15×15 cm with ten rows of 10 holes to insert the pins, and the other half contains a shallow tray to keep the sufficient number of pins. The test required the use of tweezers, in placing a single pin in each approximately 0.16cm diameter hole, as quickly as possible. The individual is instructed to fill the holes beginning left to right and from top row to the bottom. To familiarize with the test, participants were given trials of filling two rows before the actual test. Timing was measured in seconds starting when the subject picked up the tweezer and ended with filling 100 holes. The lesser the score, the higher the efficiency in performance [23].
Automatic Mirror Tracer
The subjects were asked to take a seat restfully in front of a table where the Automatic Mirror Tracer was set up. The Automatic Mirror Tracer (Lafayette, Model 58024A) consists of an aluminum plate with a non-conducting black star pattern anodized into the surface. A metal shield on the instrument prevents the subject from viewing the black star pattern. Subjects were able to see the pattern by looking in a mirror placed vertically behind the star. Participants were instructed to hold a metallic-tracing stylus in their preferred hand and trace as fast and accurately as possible, attempting to stay within the pattern, from a starting mark. The aluminum plate and the metallic-tracing stylus are both connected to the Silent Impulse Counter (Lafayette, Model 58024C), errors tallied automatically when stylus touch outside the margins of the non-conducting black star pattern. The time and error committed were recorded [19].
Statistical Analysis
All statistical analyses were done with the R platform (version 3.4.0). Descriptive statistics were stated in mean±SD for continuous variables. Categorical variables quantified as frequencies (percentage). The hypothesis of normality was assessed by Shapiro-Wilk tests and visual examination of the standard Q&Q plot. Univariate statistics on the differences between baseline variables calculated from the chi-square test, the Mann-Whitney test or Student t-test. A paired sample t-test and Wilcoxon signed-rank test were used to determine whether there was a statistically remarkable mean difference of pre- and post-yoga intervention. Further, effect size, Cohen’s d, was calculated (Cohen, 1988). All analyses were considered statistically significant was considered at p <0.05.
Results
In total 66 recruited patients, data for 63 were included for final analysis. The dropout reasons are highlighted in [Table/Fig-1]. Further, [Table/Fig-2], summarizes baseline information and outcome parameters between the yoga and physical exercise groups. A significant enhancement in tapping speeds between 0-10 seconds (TSI) were observed in both the yoga (p< 0.05, d = -0.53) and the exercise group (p<0.026, d= -0.42). Post intervention shows differences in 10-20 seconds (TS2), statistically significant increased mean in yoga (p < 0.036, d = -0.35) and exercise (p <0.032, d = -0.40). Furthermore, on the 20-30 seconds (TS3), improvement were noted in yoga (p < 0.078, d = -0.32) and exercise group (p< 0.478, d = -0.13), but not statistically significant. The results from the tweezer dexterity were significantly better, when post scores were compared with their respective pre-scores following yoga (p< 0.001, d = 0.99) and exercise (p< 0.001, d = 0.82). Furthermore, a significant reduction was seen in Mirror time after yoga (p< 0.034, d = 0.39) and exercise (p< 0.006, d = 0.53), with differences high in exercise group following three months. Wilcoxon signed-rank test showed a statistically significant median decrease in mirror error score when subjects imbibed the yoga (17) compared to the pre (19.50), z = -1.991, p =.046. While following physical exercise, median reduced in mirror error score (18) compared to the pre (21), z = -1.590, p =.112, but not statistically significant. The details have been highlighted in [Table/Fig-3].
Baseline characteristics of the yoga and exercise groups.
| | Yoga Mean±SD [Min-Max] | Physical Mean±SD [Min-Max] | | p-value |
|---|
| Age^ | | 24.25±5.59(18-40) | 24.77±5.02(18-40) | U= 447, z = -0.676 | 0.499 |
| Education+ | ≤Intermediate level | 23(71.9) | 20(64.5) | χ2(1)=0.394 | 0.530 |
| Bachelor and above | 9(28.1) | 11(35.5) |
| Marital+ | Married | 7(21.9) | 8(25.8) | χ2(1)=0.134 | 0.714 |
| Unmarried | 25(78.1) | 23(74.2) |
| Alcohol+ | No | 5(15.6) | 5(16.1) | χ2(1)=0.003 | 0.956 |
| Yes | 27(84.4) | 26(83.9) |
| Cannabis+ | No | 4(12.5) | 5(16.1) | χ2(1)=0.169 | 0.681 |
| Yes | 28(87.5) | 26(83.9) |
| Opiates+ | No | 6(18.8) | 11(35.5) | χ2(1)=2.23 | 0.135 |
| Yes | 26(81.2) | 20(64.5) |
| Tranquillizers+ | No | 12(37.5) | 16(51.6) | χ2(1)=1.27 | 0.260 |
| Yes | 20(62.5) | 15(48.4) |
| Stimulants+ | No | 12(37.5) | 15(48.4) | χ2(1)=0.762 | 0.383 |
| Yes | 20(62.5) | 16(51.6) |
| Inhalants+ | No | 18(56.3) | 16(51.16) | χ2(1)=0.136 | 0.712 |
| Yes | 14(43.8) | 15(48.4) |
| Variables | | Mean±SD | Mean±SD | | |
| Years Intake Drug^ | | 7.06±5.70 | 6.61±5.05 | U=475.5,z = -0.296 | 0.788 |
| Tapping10s@ | 37.00±7.81 | 38.45±7.72 | t (61) = -0.741 | 0.461 |
| Tapping20s@ | 35.28±8.02 | 35.71±7.73 | t(61) = -0.216 | 0.830 |
| Tapping30s@ | 26.59±8.44 | 28.03±8.65 | t(61) = -0.668 | 0.507 |
| Tweezer Dexterity@ | 471.94±81.79 | 458.32±90.68 | t(61) = 0.626 | 0.534 |
| Mirror Time@ | 83.25±37.45 | 71.32±30.11 | t(61) = 1.39 | 0.169 |
| Mirror Error^ | 29.00±30.12 | 32.45±31.40 | U= 462,z = -0.468 | 0.640 |
Mann-Whitney test, @Student t-test and+Chi-square test
Comparison of motor function in yoga and physical exercise groups following 12 weeks of intervention.
| Yoga (n=32) | Exercise (n=31) |
|---|
| Measures | Pre | Post | 95% CI | t | p | d | Pre | Post | 95% CI | t | p | d |
|---|
| Tapping 10s | 37.00 (7.81) | 40.16 (7.44) | (-5.29 to -1.01) | -3.005 | 0.005 | -0.53 | 38.45 (7.72) | 40.81 (6.35) | (-4.41 to -.30) | -2.34 | 0.026 | -0.42 |
| Tapping 20s | 35.28 (8.02) | 37.59 (7.33) | (-4.47 to -.16) | -2.19 | 0.036 | -0.35 | 35.71 (7.73) | 38.39 (6.004) | (-5.11 to -.24) | -2.24 | 0.032 | -0.40 |
| Tapping 30s | 26.59 (8.45) | 29.19 (7.17) | (-5.49 to .30) | -1.82 | 0.078 | -0.32 | 28.03 (8.65) | 29.06 (6.39) | (-3.96 to1.90) | -.72 | 0.478 | -0.13 |
| TweezerDexterity | 471.91(81.79) | 412.62(76.92) | (37.85 to 80.77) | 5.64 | 0.000 | 0.99 | 458.32(90.68) | 393.65(88.99) | (35.87 to 93.48) | 4.58 | 0.000 | 0.82 |
| Mirror Time | 83.25(37.46) | 67.50(35.19) | (1.24 to 30.25) | 2.21 | 0.034 | 0.39 | 71.32(30.17) | 58.19(28.64) | (4.05 to 22.21) | 2.95 | 0.006 | 0.53 |
Paired sample t-test for compare with-in group
Differences between the yoga and physical exercise groups, summarised in [Table/Fig-4]. However, when the between-group changes in the parameters were compared, there were no significant differences between the yoga and exercise group in any of the evaluated motor functions.
Mean difference comparisons between pre-test and 12 weeks post-intervention scores
| Yoga | Exercise | t value | p-value |
|---|
| Variables | Mean±SD | Mean±SD |
|---|
| Tapping10s | 3.15±5.94 | 2.35±5.60 | t(61)=-0.551 | 0.584 |
| Tapping20s | 2.31±5.98 | 2.68±6.64 | t(61)=0.229 | 0.819 |
| Tapping30s | 2.59±8.03 | 1.03±7.99 | t(61)=-0.773 | 0.443 |
| Tweezer Dexterity | -59.31±59.52 | -64.67±78.52 | t(61)=-0.310 | 0.760 |
| Mirror Time | -15.75±40.24 | -13.13±24.74 | t(61)=0.310 | 0.765 |
| Mirror Error | -10.34±27.66 | -10.54±28.63 | t (61)=-0.029 | 0.977 |
* Mean scores were computed as differences between pre-test and post-test intervention. Differences were analysed using independent samples t-test
Discussion
Based on authors’ review of literature, this is the first randomised comparative clinical study assessintg the add-on effect of yoga or physical exercise on motor functions among substance abusers. The partakers enrolled from a rehabilitation center providing a standard therapeutic environment for detoxification to SUDs. Tasks of motor function, including fine motor speed, dexterity, and arm-hand steadiness observed significant impairment in SUDs. The present study has demonstrated 12 weeks of yoga, or physical exercise training in addition to conventional therapies producing substantial recovery of motor function in substance abuser in a residential rehabilitation center. Enhancements due to yoga and physical exercise were not significantly different.
The results are consistent with previous studies that demonstrated enrichment of motor function such as strength, dexterity, speed, flexibility, gait, and steadiness following yoga and physical exercise-based intervention in healthy adults [15,22,24], the elderly population [16,17,25] and in patients [26-28]. Dopamine (DA) is a neurotransmitter that is essential in regulating brain processes connected with motor function [29]. Previous results provide evidence that substance abuse at dose levels and long-term leads to reductions in the brain dopamine transporter, associated with significant motor function impairment [30,31]. Further, the results emphasise, interventions that enhance dopamine activity may improve motor performance irrespective of age [32]. There is an initial finding from a yoga-based intervention that showed an increased release of dopamine [33]. Furthermore, preliminary results demonstrate that substance abuse induced deficits in the dopamine system are reversible in human subjects, and exercise training can facilitate the process [34]. Increased endogenous dopamine release may be a potential mechanism by which practice of exercise or yoga enhanced motor function among SUDs. Further, the yoga-based intervention has demonstrated significant stress-reduction on psychological and physiological indices of stress among SUDs [35]. Furthermore, a recent review has highlighted moderate and high-intensity aerobic exercises, and the mind-body interventions can be an effective and sustainable treatment for those with SUDs [36].
Limitation
There are several methodological shortcomings of the present study. The lack of a control group, raising the possibility that the observed effects can attribute to the natural recovery due to 12 weeks of sobriety, or to the rehabilitation interventions. However, the normal trends of substance abuse rehabilitation, may not show improvements in the magnitude revealed in our results. The assessments were done only for the upper limb activity. The upcoming study should in co-operate lower limbs and further areas such as steadiness, strength, gait, and flexibility. Further, prospective studies should include diagnostic evaluation of understanding the individuals with severe motor impairment. Future research should explore whether integrating yoga and physical exercise would lead to more benefits than yoga or physical exercise alone. Furthermore, current research sample consist of male participants precludes the generalis ation of the results to another group.
Conclusion
Our results suggest that the add-on yoga or exercise-based intervention has shown an enhancement of motor functions. Yoga appears to be as good as physical exercise. The clinical application of findings is noteworthy, stumbling and uncoordinated motor functions quelled with sobriety, as the enhanced motor function will be a mediating factor in promoting well being and prevention of relapse. Further rigorous trials are required to explore the long-term effect and its application in the relapse prevention and to evaluate the underlying mechanisms.
Mann-Whitney test, @Student t-test and+Chi-square test
Paired sample t-test for compare with-in group
* Mean scores were computed as differences between pre-test and post-test intervention. Differences were analysed using independent samples t-test